1
Fifth stage
Surgery
Lec-4
د
.
مثنى الحموشي
13/12/2016
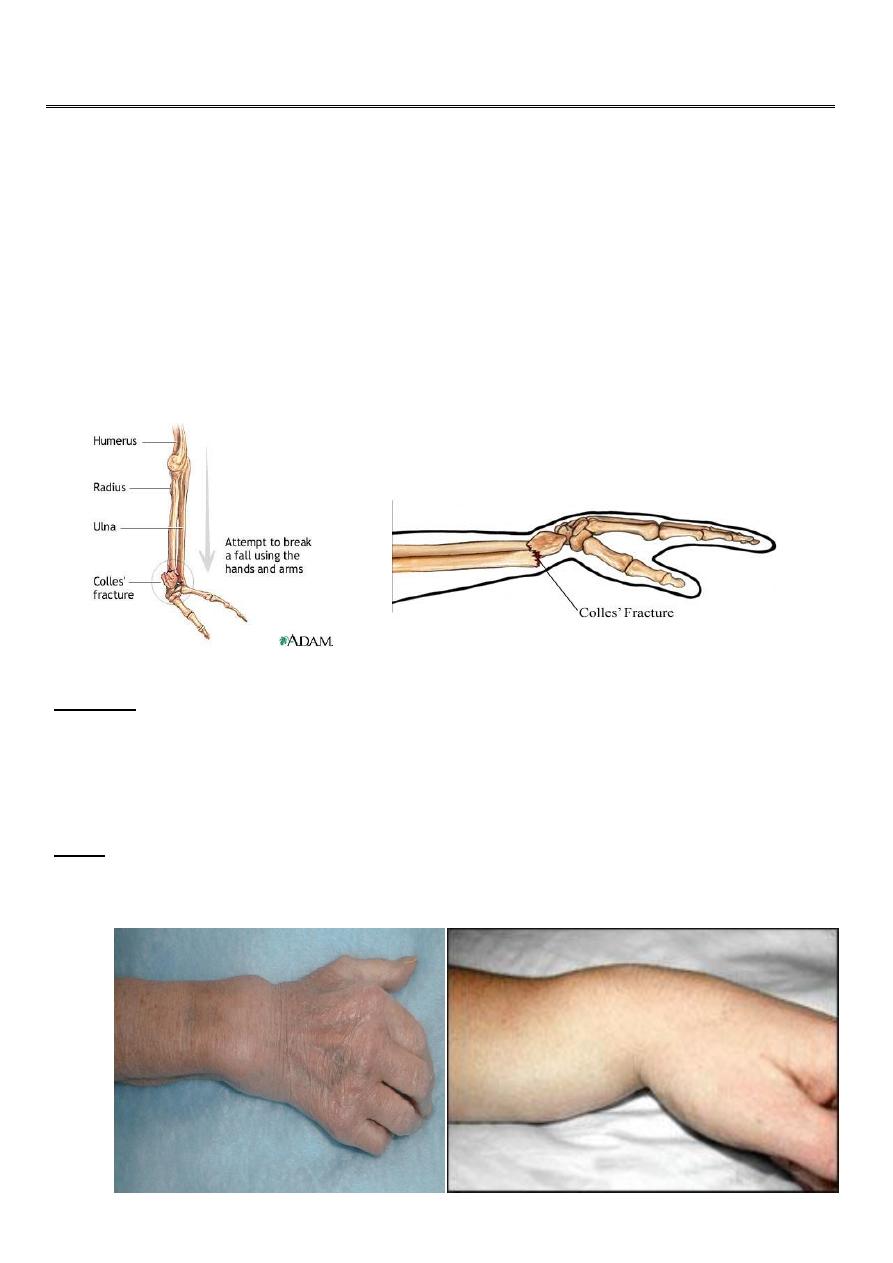
Fractures of the distal radius
Colles` fracture
This fracture is described by Ibraham colles` in 1814 .
It is a transverse fracture of the distal end of the radius with posterior displacement of the
distal fragment.
It is the most common of all fractures in the human being ; mainly in old osteoporotic
people , but it occur in all age groups .
It is occur due to fall on out stretched hands
:
Clinically
The deformity of this fracture called dinner – fork deformity .
The patient also has the sign and symptoms of any other fracture like pain , tenderness ,
loss of function , swelling …..etc .
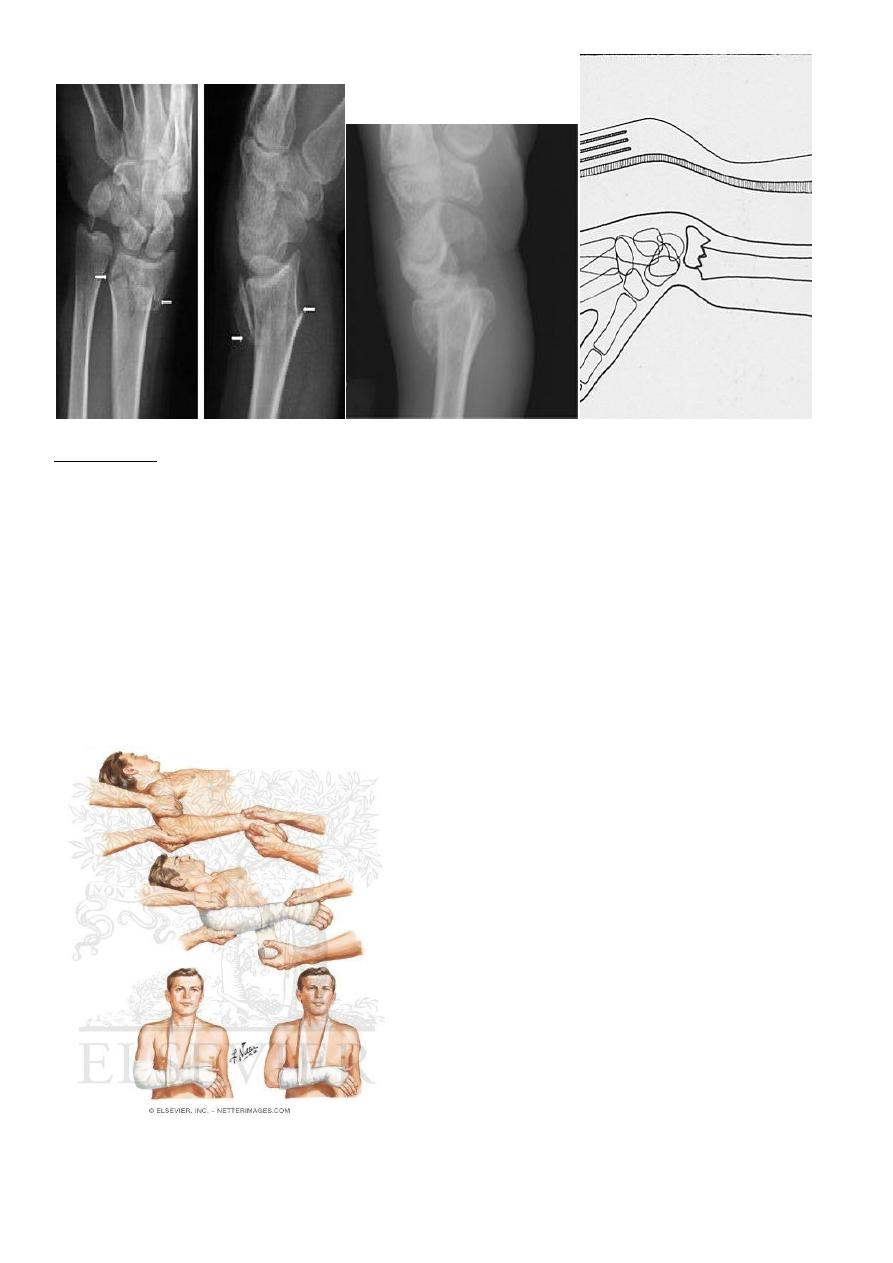
junction , and
cancellous
–
radius at the cortico
e
: there is transverse fracture of th
ray
-
X
the distal fragment is displaced posteriorly ; some time it is severely comminuted or
crushed
2
Treatment :
It must be reduced under general anesthesia, the reduction will be by traction on the hand
in the length of the bone , the distal fragment then pushed into place by pressing on the
dorsum while manipulating the wrist into flexion , ulnar deviation and pronation
Then put back slab and check by x-ray .
The back slab from below elbow to the neck of the metacarpals .
Extreme pronation , flexion and ulnar deviation must be avoided ; 20` in each direction is
adequate .
Shoulder and fingers exercise then started .
After 7-10 days remove the slab and do full
p.o.p. . The fracture usually unite in 6 weeks
3
Complication :
:
early
1-vascular damage
radial artery (rare) .
2- nerve damage median nerve (rare) .
:
Late complication
1- malunion : it is common due to
unreduced fracture or due to
redislpacement .
2- delayed union and non union .
3-stiffness of the wrist ,fingers, elbow and shoulder
4-tendon rupture of extensor polices longus .
5- sudeck`s dystrophy (localized sympathetic over
activity).
6-carpal- tunnel syndrome .
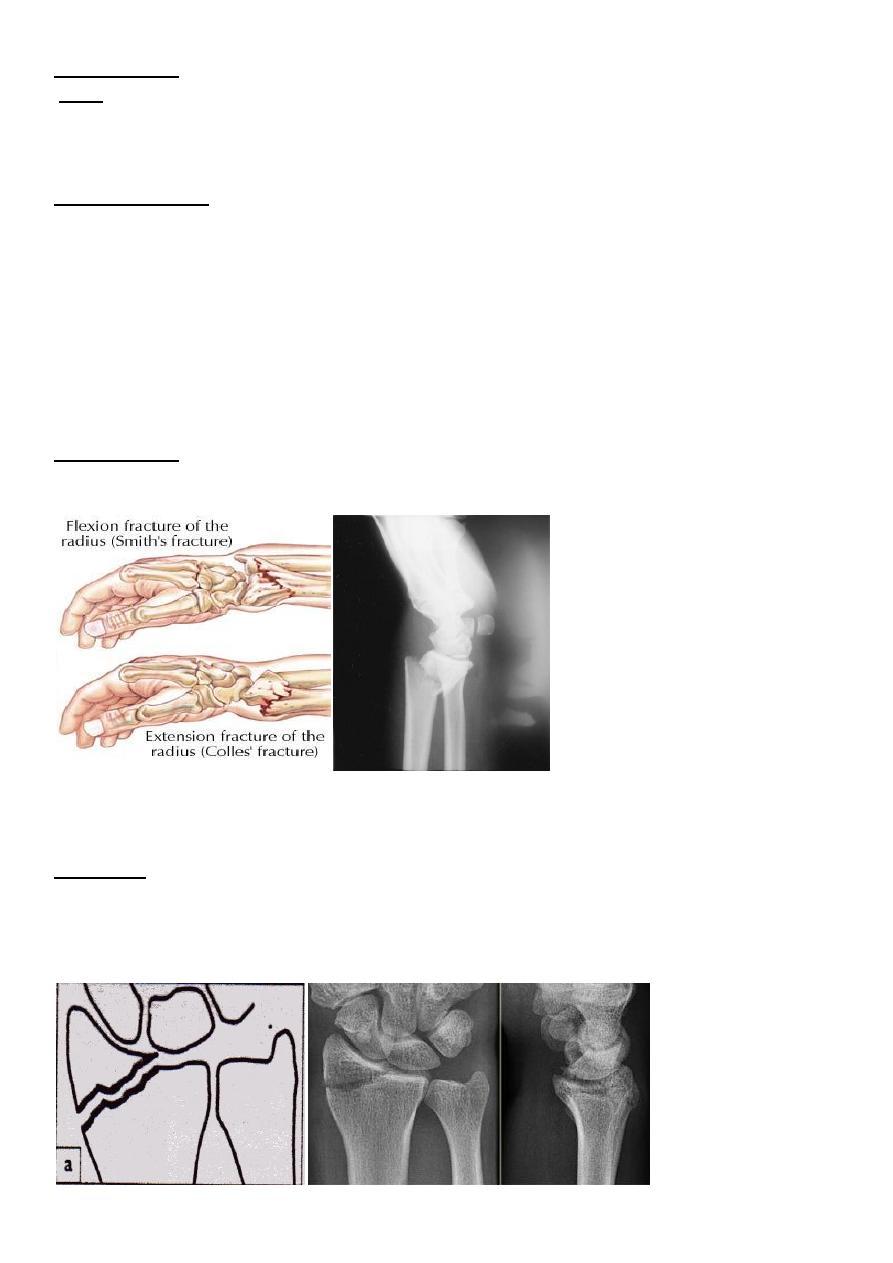
:it is the same as colles` fracture but the distal segment is displaced
Smith fracture
anteriorly .
Radial styloid process fracture :
Here the fracture line extend from the articular surface of the radius laterally .
:
Treatment
If there is displacement , the fracture should be reduced by manipulation under anesthesia ,
then back slab below elbow tell the neck of the metacarpal ; imperfect reduction will lead
to osteoarthritis , so if the fracture not reduced perfectly by manipulation then open
reduction and fixation by screw or k wire .
4
BARTON`S FRACTURE
It is intra articular fracture of the lower end of the radius with subluxation of the wrist joint.
It is of two types :
sociated with volar subluxation of
it as
called true Barton fracture and
`:
volar Barton's
-
1
the carpus . The fracture line run obliquely across the volar lip of the radius into the wrist
joint . The distal segment displaced anteriorly carrying the carpus with it .
s unstable so it can easily redisplaced so the
the fracture easily reduced but it i
:
Treatment
treatment will be by open reduction and fixation by special plate called Buttress plate .
it is the reverse of the volar one .
:
dorsal Barton`s
-
2
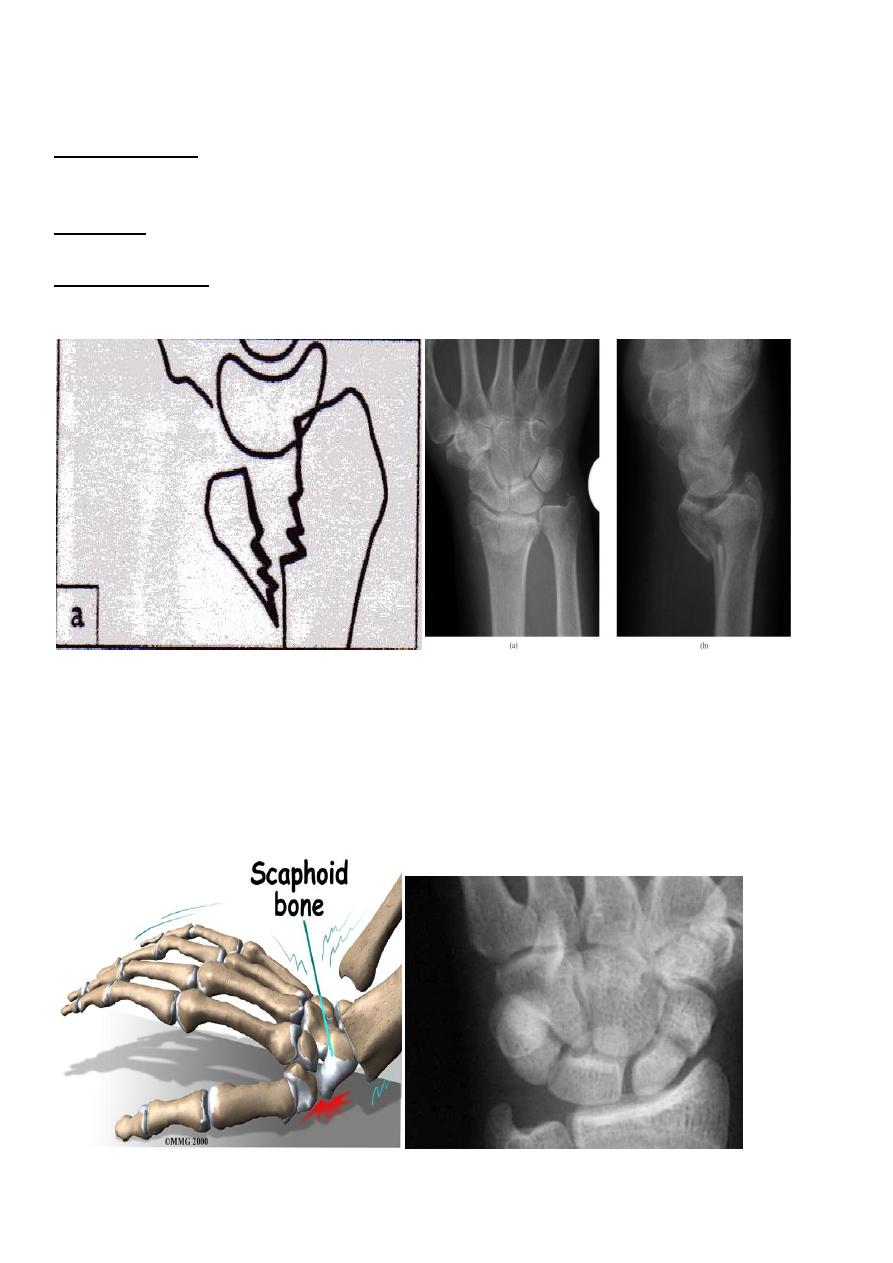
Fracture scaphoid bone
It is caused by fall on out stretched hands ; the most important point in scaphoid is its blood
supply inter the bone from distal to proximal direction , so the blood supply is decreased
from distal to proximal ; this fact explain why only 1% of the fracture in the distal third of
scaphoid , 20% of the fract. In the middle third and 40% of the proximal third fract. Will
develop avascular necrosis and non union .

5
stic
: there is fullness and tenderness in the anatomical snuff box ; other diagno
Clinically
sign is that, proximal pressure along the axis of the thumb is painful .
p , lateral and oblique views are all essentials . Some time recent fracture show it
-
: a
ray
-
X
self only in oblique view .
Usually the fracture is transverse and through the narrowest part of the bone (the waist) ,
but it could be in the proximal pole or in the tubercle ; few weeks after injury the fracture
will be more obvious.
If union is delayed , cavitation appear on either side of the fracture .
In old ununited fracture there will be sclerosis at the edge and the appearance will be as
there is extra carpal bone .
Sclerosis of the proximal fragment is path gnomonic of avascular necrosis of the proximal
fragment .
Treatment :
p.o.p. cast in 90% of the cases will heal ;
: conservative treatment by
Undisplaced fracture
the cast will be applied from upper forearm to just short of the metacarpophalangeal joint
of the fingers but it should incorporating the proximal phalanx of the thumb ; the wrist is
held in dorsiflexion and the thumb forward in ( GLASS HOLDING ) position and it should be
retained for 6 weeks .
After 6 weeks the p.o.p. removed and the wrist examined clinically and radiologically , if
there is no tenderness and the x-ray show sign of healing , the wrist is left free
If there is local tenderness or the fracture is still visible in x-ray , the p.o.p. is reapplied for
further 6 weeks and after that either the wrist become painless and the fracture healed so
the p.o.p. removed or the x-ray show sign of delayed healing then we should do fixation
and bone grafting .
: treatment by open reduction and fixation by compression screw .
Displaced fracture
6
Complication
:
avascular necrosis
-
1
the proximal fragment may die especially with proximal pole fracture , it will appear
dense on x-ray .
: by excision of the proximal fragment .
Treatment
: after 3 months if fracture not united it will be obvious that the fracture will
non union
-
2
not unite at all .
symptomatic , non union may
:in old people and in those who are completely a
Treatment
be left untreated .
In young patients treatment by fixation and bone grafting .
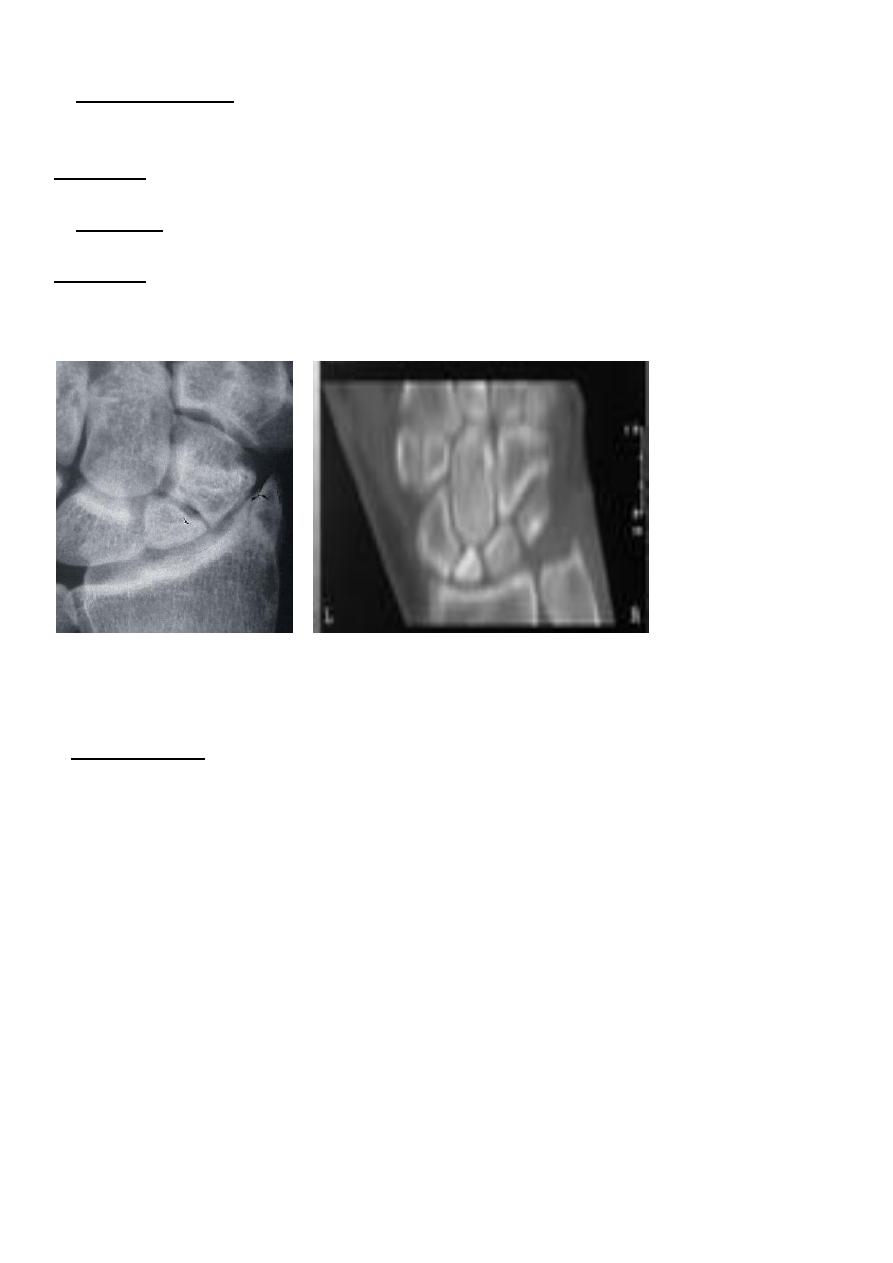
Avascular necrosis of proximal segment of scaphoid frac.
non union fracture scaphoid
If the graft fail then do excision of the scaphoid and fusion of the carpel bones .
osteoarthritis :
-
3
non union and avascular necrosis may lead to secondary osteoarthritis .