1
Fifth stage
Pediatrics
Lec-3
Dr. Athal
23/11/2016
Infectious disease
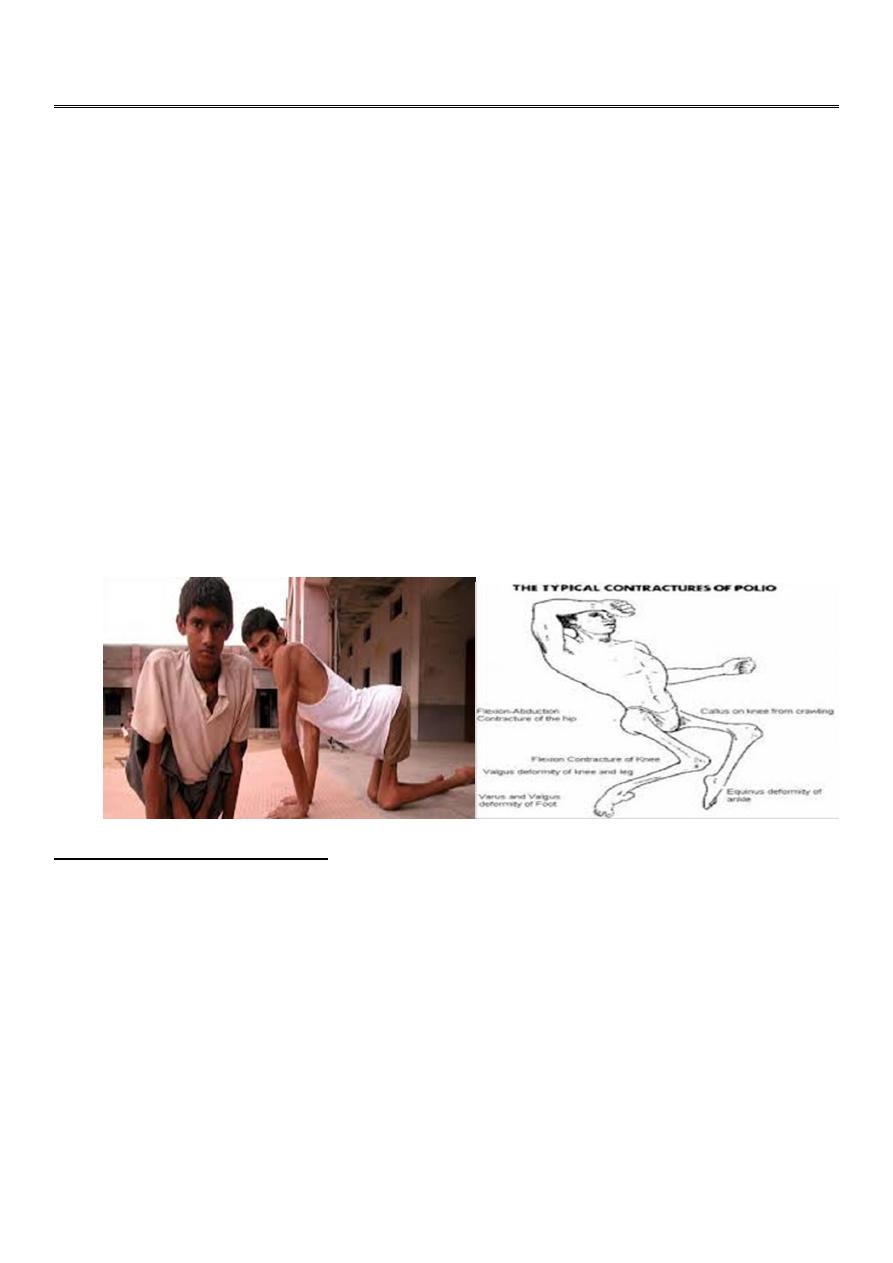
Polioviruses
The polioviruses are nonenveloped, positive-stranded RNA viruses.
Consist of 3 antigenically distinct serotypes (types 1, 2, and 3)
The most devastating result of poliovirus infection is paralysis, although 90-95% of
infections are inapparent but induce protective immunity.
The virus spread by the fecal-oral route. It has been isolated from feces for longer than 2
wk before paralysis to several weeks after the onset of symptoms.
Poor sanitation and crowding have permitted the increase transmission of poliovirus.
Infants acquire immunity transplacentally from their mothers. Transplacental immunity
disappears at a variable rate during the 1st 4-6 mo of life. Active immunity after natural
infection is probably lifelong but protects against the infecting serotype only; infections
with other serotypes are possible.
CLINICAL MANIFESTATIONS
The incubation period of poliovirus from contact to initial clinical symptoms is usually
considered to be 8-12 days, with a range of 5-35 days.
Poliovirus infections with wild-type virus may follow 1 of several courses:
1. Inapparent Infection: which occurs in 90-95% of cases and causes no disease and no
sequelae.
2. Abortive Poliomyelitis:
approximately 5% of patients, a nonspecific influenza-like syndrome which is short lived,
lasting up to 2-3 days. Recovery is complete, and no neurologic signs or sequelae develop.
3. Nonparalytic Poliomyelitis:
in approximately 1% of patients infected with wild-type poliovirus, signs of abortive
poliomyelitis are present, as are more intense headache, nausea, and vomiting, as well as

2
soreness and stiffness of the posterior muscles of the neck, trunk, and limbs. Fleeting
paralysis of the bladder and constipation are frequent. Approximately two thirds of these
children have a short symptom-free interval between the 1st phase (minor illness) and the
2nd phase (CNS disease or major illness). Nuchal rigidity and spinal rigidity are the basis for
the diagnosis of nonparalytic poliomyelitis during the second phase.
4. Paralytic Poliomyelitis:
approximately 0.1% of persons infected with poliovirus, causing 3 clinically recognizable
syndromes. These are:
Spinal paralytic poliomyelitis.
Bulbar poliomyelitis.
Polioencephalitis.
DIAGNOSIS
Poliomyelitis should be considered in any unimmunized or incompletely immunized child
with paralytic disease.
VAPP should be considered in any child with paralytic disease occurring 7-14 days after
receiving the orally administered polio vaccine (OPV) or even later. The combination of
fever, headache, neck and back pain, asymmetric flaccid paralysis without sensory loss,
and pleocytosis does not regularly occur in any other illness.
The WHO recommends that the laboratory diagnosis of poliomyelitis be confirmed by
isolation and identification of poliovirus in the stool, with specific identification of wild-
type and vaccine-type strains.
In suspected cases of acute flaccid paralysis, 2 stool specimens should be collected 24-48
hr apart as soon as possible after the diagnosis of poliomyelitis is suspected. Poliovirus
concentrations are high in the stool in the 1st wk after the onset of paralysis, which is
the optimal time for collection of stool specimens.
In polioencephalitis, the serologic testing demonstrates seroconversion or a 4-fold or
greater increase in antibody titers from the acute phase of illness to 3-6 wk later.
DIFFERENTIAL DIAGNOSIS
There are numerous other causes of acute flaccid paralysis. In most conditions, the
clinical features are sufficient to differentiate between these various causes, but in some
cases nerve conduction studies and electromyograms, in addition to muscle biopsies,
may be required.
Guillain- Barré syndrome.
Transverse myelitis.
Traumatic paralysis.
3
TREATMENT
There is no specific antiviral treatment for poliomyelitis .
The management is supportive and aimed at limiting progression of disease.
All intramuscular injections and surgical procedures are contraindicated during the
acute phase of the illness, especially in the 1st wk of illness, because they might result in
progression of disease.
PROGNOSIS
The outcome of inapparent, abortive poliomyelitis and aseptic meningitis syndromes is
uniformly good, with death being exceedingly rare and with no long-term sequelae .
The outcome of paralytic disease is determined primarily by degree and severity of CNS
involvement.
PREVENTION
Vaccination is the only effective method of preventing poliomyelitis.
Hygienic measures help limit the spread of the infection among young children.
Epstein-Barr Virus (EBV)
EBV is a double-stranded DNA virus that is a member of the γ-herpesviruses and causes
>90% of cases of infectious mononucleosis (IMN) .
As many as 5-10% of infectious mononucleosis–like illnesses are caused by primary
infection with CMV, Toxoplasma gondii, adenovirus, hepatitis virus, HIV, and possibly
rubella virus.
EBV infects more than 95% of the world’s population.
In children, it is transmitted primarily via oral secretions.
4
CLINICAL MANIFESTATIONS
The incubation period of IMN in adolescents is 30-50 days.
The majority of cases of primary EBV infection in infants and young children are clinically
silent. In older patients, the onset of illness is usually insidious and vague.
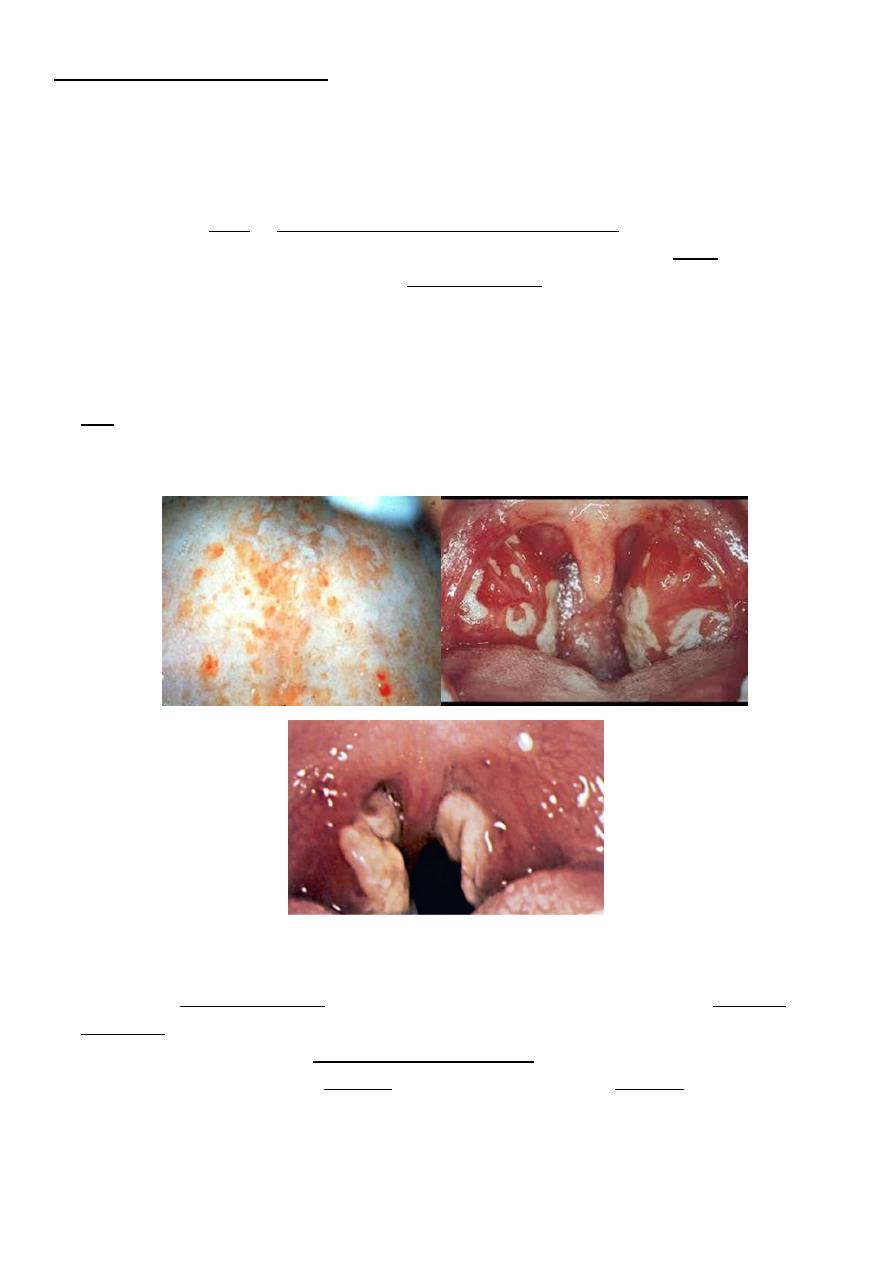
The classic presentation of EBV infectious mononucleosis in children and young adults
consists of the triad of fever, sore throat, & lymphadenopathy.
Patients may complain of malaise, fatigue, acute or prolonged(>1wk) fever, headache,
nausea, abdominal pain, and myalgia .The sore throat which is often accompanied by
moderate to severe pharyngitis with marked tonsillar enlargement, occasionally with
exudates. Palatal petechiae at the junction of the hard and soft palate are frequently
seen. The pharyngitis resembles that caused by streptococcal infection. This prodromal
period may last 1-2 wk.
LAP occurs most commonly in the anterior and posterior cervical nodes and may be
generalized. Epitrochlear LAP is particularly suggestive of IMN.
Splenomegaly in (50% of cases), and hepatomegaly in (10% of cases).
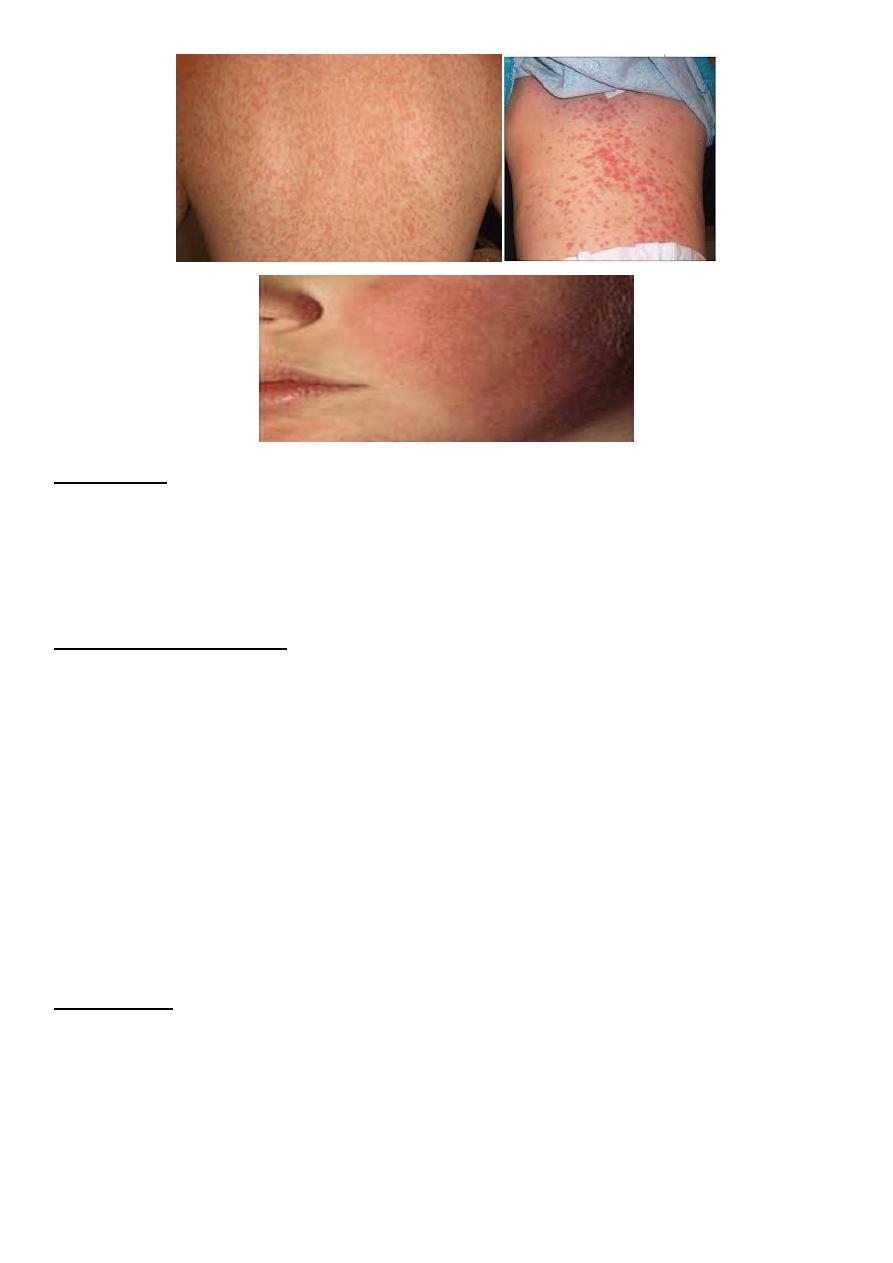
Rashes are usually maculopapular and have been reported in 3-15% of patients .
Patients with infectious mononucleosis treated with ampicillin or amoxicillin may
experience “ampicillin rash”. This morbilliform, vasculitic rash is probably immune
mediated and resolves without specific treatment.
EBV is also associated with Gianotti-Crosti syndrome, a symmetric rash on the cheeks
with multiple erythematous papules, which may coalesce into plaques and persist for
15-50 days.
5
DIAGNOSIS
Presence of typical clinical symptoms .
Leukocytosis with atypical lymphocytosis in the peripheral blood.
The diagnosis is usually confirmed by serologic testing (antibodies detection).
Culture of EBV.
COMPLICATIONS (imp.)
splenic rupture.
Swelling of the tonsils and oropharyngeal lymphoid tissue may be substantial and may
cause airway obstruction.
Headache, with severe neurologic manifestations, such as seizures and ataxia.
Perceptual distortions of sizes, shapes, and spatial relationships, known as the Alice-in-
Wonderland syndrome (metamorphopsia).
Guillain-Barré syndrome .
Reye syndrome.
Hemolytic anemia, TCP & neutropenia .
Myocarditis or interstitial pneumonia may occur, both resolving in 3-4 wk .
Other rare complications include pancreatitis, parotitis, and orchitis.
PROGNOSIS
The prognosis for complete recovery is excellent.
The major symptoms typically last 2-4 wk followed by gradual recovery within 2 mo of
onset of symptoms.
Occasional persistence of fatigue for a few years after infectious mononucleosis is well
recognized.

6
TREATMENT
o There is no specific treatment for IMN. The mainstays of management is supportive as
rest, encouraging adequate fluid and nutrition intake, and symptomatic treatment with
acetaminophen or NSAI agents to manage fever, throat discomfort, and malaise.
o advise against participation in contact sports and strenuous athletic activities during the
1st 2-3 wk of illness or while splenomegaly is present.
o Short courses of corticosteroids (<2 wk) may be helpful for selected complications of
IMN, include airway obstruction, thrombocytopenia with hemorrhaging, autoimmune
hemolytic anemia, seizures, and meningitis.