Oxygen Therapy
Oxygen was discovered independently by the Swedish apothecary Karl W.Scheele, in 1772, and by the English amateur chemist Joseph Priestly,in August 1774.Priestley first liberated oxygen by intensely heating 'mercurius calcinatus' (mercuric oxide) placed over liquid mercury in a closed vessel. He called this new gas "dephlogisticated air, "oxygenated."
Joseph Priestley and Carl Wilhelm Scheele both independently discovered oxygen, but Priestly is usually given credit for the discovery.
Priestley called the gas produced in his experiments 'dephlogisticated air' and Scheele called his 'fire air'.
The name oxygen was created by Antoine Lavoisier who incorrectly believed that oxygen was necessary to form all acids.
The Element Oxygen
Atomic Number: 8Atomic Weight: 15.9994
Melting Point: 54.36 K (-218.79°C or -361.82°F)
Boiling Point: 90.20 K (-182.95°C or -297.31°F)
Density: 0.001429 grams per cubic centimeter
Phase at Room Temperature: Gas
Element Classification: Non-metal
Period Number: 2
Group Number: 16 Group Name: Chalcoge
Oxygen is a drug
Colorless, odorless, tasteless gas, makes up 21% of room air .It is NOT flammable but does support combustion.should be regarded as a drug .
Has a Drug Identification Number (DIN)
Oxygen must be prescribed in all situations (except for the immediate management of critical illness).
Oxygen should be prescribed to achieve a target saturation (Sp02), which should be written on the drug chart .
Basic Concepts of Oxygen
Composition of Room Air Nitrogen 78.08% ~78% Oxygen 20.946% ~21% Trace gases ~1%
Normal PO2 in arterial blood (PaO2) ≥ 95mmHg: decrease with age.
PO2 in mitochondria ≥ 18 mmHg required to generate high energy phosphate bonds e.x ATP
At rest the average adult male consumes about 225-250 ml of O2/min.
This can increase up to 10 folds during exercise.
There’s very small O2 reserve that can be consumed within 4-6 minutes of cessation of spontaneous ventilation.
Oxygen content of blood
The theoretical maximum oxygen carrying capacity is 1.39 ml O2/g Hb, but direct measurement gives a capacity of 1.34 ml O2/g Hb.1.34 is also known as Hüfner’s constant.The oxygen content of blood is the volume of oxygen carried in each 100 ml blood.It is calculated by: (O2 carried by Hb) + (O2 in solution) = (1.34 x Hb x SpO2 x 0.01) + (0.023 x PaO2)
Basic Concepts of Oxygen
Oxygen Cascade:Inspired = 150 mmHg at Sea Level ↓ Alveolar PO2= 103
↓ Arterial=100
↓ Capillary= 51
↓ Mitochondrial= 1-10
(FiO2 expressed as 0.21-1.0 or 21- 100%)
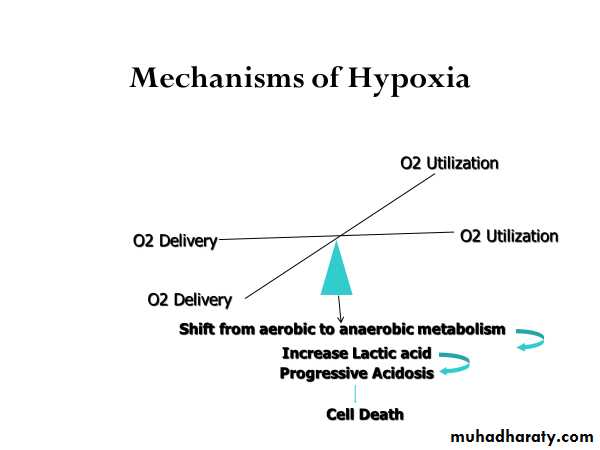
Clinical Conditions With Increased Risk of Hypoxia
Myocardial infarction
Acute pulmonary disorders
Sepsis
Drug overdose
Liver failure
Head trauma
CHF
Hypovolemic shock
Blunt chest trauma
Acute neuromuscular disease
Acute abdomen (splinting)
Acute pancreatitis
Spinal cord injury
Indications for Oxygen Therapy
Tachypnea
Cyanosis
Restlessness
Disorientation
Cardiac arrhythmias
Slow bounding pulse
Tachycardia
Hypertension
Dyspnea
Coma
Labored breathing (use of accessory muscles, nasal flaring)
Lethargy
Tremors/seizure activity
“Generally speaking”, a patient who is breathing less than 12 and more than 24 times a minute needs oxygen of some kind
Oxygen therapy To ensure safe and effective treatment
Oxygen is required for the functioning and survival of all body tissues and deprivation for more than a few minutes is fatal.In immediately life threatening situations oxygen should be administered.
Hypoxaemia. Acute hypotension. Breathing inadequacy. Trauma. Acute illness. CO poisoning. Severe anaemia. During the peri-operative period.
Oxygen therapy Humidification Is recommended if more than 4 litres/min is delivered.
Helps prevent drying of mucous membranes.
Helps prevent the formation of tenacious sputum.
Oxygen concentrations will be affected with all delivery systems if not fitted correctly or tubing becomes kinked and ports obstructed.
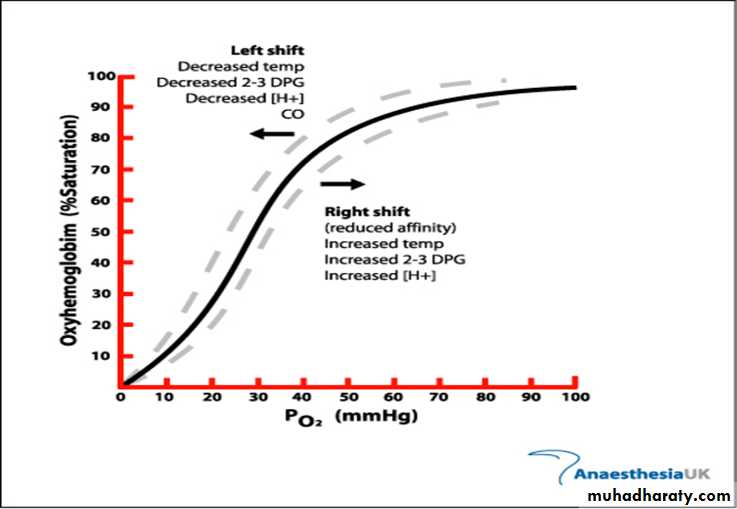
The oxyhaemoglobin dissociation curve showing the relation between partial pressure of oxygen and haemoglobin saturation
Methods of Oxygen Delivery
Most common methods of oxygen delivery includeNasal Cannula
Venturi Mask
100% Non-Rebreather Mask
Mechanical Ventilation
Nasal Cannula
Comfortable, convenient, mouth breathing will not effect % of O2 deliveredLiters/min = %
2 l/m = 24-28%
3 l/m = 28-30%
4 l/m = 32-36%
5 l/m = 36-40%
6 l/m = 40-44%
Cannot administer > 6 liters/minute (44%)
Provides limited oxygen concentration
Used when patients cannot tolerate mask
Prongs and other uses
Concentration of 24 to 44%
Flow rate set between 1 to 6 liters
For every liter per minute of flow delivered, the oxygen concentration the patient inhales increases by 4%
Venturi Mask
FiO2 Delivery
Blue 24% Yellow 28%
White 31% Green 35%
Pink 40%
Concerns
Tight seal is a must Interferes with eating/drinking
Condensation collection
Provides precise concentrations of oxygen
Entrainment valve to adjust oxygen delivery
Mostly used in the hospital setting for COPD patients


100% Non-Rebreather
Delivery percentages6 l/min = 55 – 60 %
8 l/min = 60 – 80 %
10 l/min = 80 – 90 %
>12 l/min = 90 + %
Benefit: Has a one way expiratory valve that prevents re-breathing expired gases
Concern
May lead to O2 toxicity


100% Non-Rebreather Mask partial rebreather Mask
Mechanical Ventilation
Allows administration of 100% oxygenControls breathing pattern for patients who are unable to maintain adequate ventilation
Is a temporary support that “buys time” for correcting the primary pathologic process
Indications for Mechanical Ventilation
Mechanical FailureVentilatory Failure
Oxygenation Failure
General Anesthesia
Post-Cardiac Arrest

Two categories of ventilators
Negative pressure ventilators
Iron lung
Cuirass ventilator
Positive pressure ventilators
Two categories
Volume-cycled (volume-preset)
Pressure-cycled (pressure-preset)
Mechanical Ventilation PEEP
Description
Maintains a preset positive airway pressure at the end of expiration
Increases PaO2 so that FiO2 can be decreased
Increases DO2 (amt of delivered O2 to tissue)
Maximizes pulmonary compliance
Minimized pulmonary shunting
Indications
PaO2 < 60 on FiO2 > 60% by recruiting dysfunctional alveoli
Increases intrapulmonary pressure after cardiac surgery to decrease intrathoracic bleeding (research does not support this idea)
Advantages
Improves PaO2 and SaO2 while allowing FiO2 to be decreased
Decreases the work of breathing
Keeps airways from closing at end expiration (esp. in pts with surfactant deficiency)
Disadvantages
Increased functional residual capacity (increases risk for barotrauma)
Can cause increased dead space and increased ICP
In pts with increased ICP, must assure CO2 elimination
Contraindicated: hypovolemia, drug induced low cardiac output, unilateral lung disease, COPD


Mechanical Ventilation CPAP
DescriptionConstant positive pressure is applied throughout the respiratory cycle to keep alveoli open
Indications
To wean without having to remove the ventilator and having to connect to additional equipment
Mechanical Ventilation CPAP
Advantages
Takes advantage of the ventilator alarm systems providing psychological security of the ventilator being there
Disadvantages


Patient may sense resistance as he breathes through the ventilator tubing
Mechanical Ventilation Complications
Respiratory arrest from disconnectionRespiratory infection (VAP)
Acid-base imbalances
Oxygen toxicity
Pneumothorax
GI bleeding
Barotrauma
Decreased cardiac output
Ventilator Weaning
Vital Capacity at least 10 – 15 ml/kg
Tidal Volume > 5 ml/kg
Resting minute volume > 10 L per minute
ABG’s adequate on < 40% FiO2
Stable vital signs
Intact airway protective reflexes (strong cough)
Absence of dyspnea, neuromuscular fatigue, pain, diaphoresis, restlessness, use of accessory muscles
Primary Acid-base Disorders:
Respiratory alkalosis - A primary disorder where the first change is a lowering of PaCO2, resulting in an elevated pH. Compensation (bringing the pH back down toward normal) is a secondary lowering of bicarbonate (HCO3) by the kidneys; this reduction in HCO3- is not metabolic acidosis, since it is not a primary process.Primary Event Compensatory Event
HCO3- ↓HCO3-
↑ pH ~ ------- ↑ pH ~ --------
↓ PaCO2 ↓ PaCO2:
Respiratory acidosis - A primary disorder where the first change is an elevation of PaCO2, resulting in decreased pH. Compensation (bringing pH back up toward normal) is a secondary retention of bicarbonate by the kidneys; this elevation of HCO3- is not metabolic alkalosis since it is not a primary process.
Primary Event Compensatory Event
HCO3- ↑ HCO3-
↓ pH ~ --------- ↓ pH ~ ---------
↑PaCO2 ↑ PaCO2
Metabolic acidosis - A primary acid-base disorder where the first change is a lowering of HCO3-, resulting in decreased pH. Compensation (bringing pH back up toward normal) is a secondary hyperventilation; this lowering of PaCO2 is not respiratory alkalosis since it is not a primary process.
Primary Event Compensatory Event
↓ HCO3- ↓HCO3-
↓ pH ~ ------------ ↓ pH ~ ------------
PaCO2 ↓ PaCO2
Metabolic alkalosis - A primary acid-base disorder where the first change is an elevation of HCO3-, resulting in increased pH. Compensation is a secondary hypoventilation (increased PaCO2), which is not respiratory acidosis since it is not a primary process. Compensation for metabolic alkalosis (attempting to bring pH back down toward normal) is less predictable than for the other three acid-base disorders.
Primary Event Compensatory Event
↑ HCO3- ↑HCO3-
↑ pH ~ ------------ ↑ pH ~ ---------
PaCO2 ↑PaCO2
Some Clinical Causes
METABOLIC ACIDOSIS ↓HCO3- & ↓ pHIncreased anion gap
lactic acidosis; ketoacidosis; drug poisonings (e.g., aspirin, ethylene glycol, methanol)
Normal anion gap
diarrhea; some kidney problems (e.g., renal tubular acidosis, interstitial nephritis)
METABOLIC ALKALOSIS ↑ HCO3- & ↑ pH
Chloride responsive (responds to NaCl or KCl therapy): contraction alkalosis, diuretics, corticosteroids, gastric suctioning, vomitingChloride resistant: any hyperaldosterone state (e.g., Cushing’s syndrome, Bartter’s syndrome, severe K+ depletion)
RESPIRATORY ACIDOSIS ↑PaCO2 & ↓ pH
Central nervous system depression (e.g., drug overdose)
Chest bellows dysfunction (e.g., Guillain-Barré syndrome, myasthenia gravis)
Disease of lungs and/or upper airway (e.g., chronic obstructive lung disease, severe asthma attack, severe pulmonary edema)
RESPIRATORY ALKALOSIS ↓PaCO2 & ↑ pH
Hypoxemia (includes altitude)
Anxiety
Sepsis
Any acute pulmonary insult (e.g., pneumonia, mild asthma attack, early pulmonary edema, pulmonary embolism)