Cardio.Lect.3 Prof.Dr.Hussain Al-Janabi MRCP(UK),FRCP(Lond.)
Ischemic Heart Disease(IHD). IHD refers to a group of clinical syndromes caused by myocardial ischemia often as a consequence of atherosclerotic coronary artery disease. Coronary Arteries: two coronary arteries originate from the left side of the heart at the beginning (root) of the aorta, just after the aorta exits the left ventricle. The left coronary artery(LCA) originates from the left aortic sinus, while the right coronary artery(RCA) originates from the right aortic sinus. LCA devides within 2-3cm of its origin where it is called left main stem(LMS) into left anterior descending A(LAD)&left circumflex A(LCX).

Diagram showing main coronary arteries&their territorial supply. Coronary artery dominance:The artery that supplies the posterior descending artery (PDA) determines the coronary dominance&the coronary circulation is 70% right-dominant, 20% co-dominant&10% are left-dominant as PDA is supplied by RCA in 70% of population,by both RCA& LCX in 20% of population&by LCX in 10% of population. Teritorial supply(See text). Consequence of occlusion.(see text).
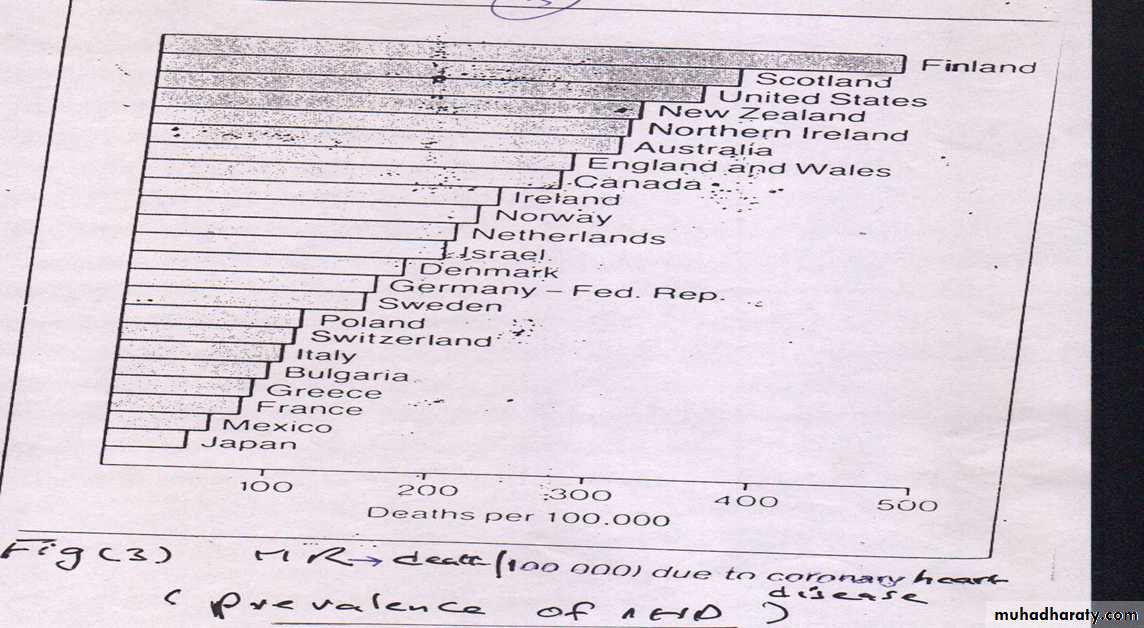
Epidemiology of IHD:It's a world wide disease with geographical variation in it's prevalence.
Causes of IHD: A.coronary causes. 1.coronary atheromatous disease is commonest cause. 2.Other rare causes like arteritis involving coronary arteries as polyarteritis nodosa&systemic vascultis,coronary spasm&embolic occlusions as atrial fibrillation. B.Non coronary causes:include aortic valve disease esp.aortic stenosis, severe pulmonary hypertension& severe anemia(why→IHD).
Pathological changes of coronary atherosclerosis:Atherosclerosis is a progressive inflammatory disease of the arteries involving lipid deposition,macrophage activation,smooth muscles migration to the intima& proliferation with fibrous tissue formation&the process is often a pachy process that lead to focal atheromtous lesions called atheromas or atheromatous plaques.The plaques either concentric&are less liable to complication &hence lead to stable angina or eccentric& liable to complications(*fissuring,ulceration or rupture *Thrombosis at site of ulceration or *Haemorrhage within it)causing critical occlusion of CA lumen leading to acute coronary syndrome i.e acute MI or unastable angina.
Risk factors of IHD. 1.Smoking. 2.Hypertension.3.Dyslipidaemia:refers to abnormalities of serum lipids: Lipids carried in the blood on protein prarticles&hence called lipoproteins:they include:1.very low density lipoprotein(VLDL) caries mainly triglycerides. 2.low density lipoprotein(LDL) caries mainly cholesterol which is the atherogenic cholestrol. 3.high density lipoprotein(HDL) caries mainl cholesterol which is the protective cholestrol.4.lipoprotein-a(Lp-a): lipoprotein that caries an apo-protein which is higly glycated protein Present in diabetic patients&is highly atherogenic lipoprotein. Normal values; N-Tc <200 & N-TG<160 mg/100 ml. the atherogenic index(AI) = Tc/ HDL-c&If AI <3(ideal)&If >5( ↑Risk of IHD). 4.Diet. Atherogenic diet→excess saturated fat(Dairy products).-Less unsaturated fat(Olive oil,Fish oil). -Antioxident deficient (Vit.C&E).5.DM. 6.Age.( (≥ 55 years for men, ≥ 65 for women) 7.Male gender.8.+Ve Family history(of premature IHD ;men <55 years, female <65 years old. 9.Excess coagulation factors;Fibrinogen,FVII.10.Hyperhomocysteinaemia. 11.Obesity (BMI ≥30 kg/m2) Doubles risk of major ischemic events.Obesity not only aggravates others but act as an indepedent RF. –Waist/Hip ratio&BMI both are predictors of IHD. 12.Sedentary life style. 13.Kidney disease ( HYPERLINK "http://en.wikipedia.org/wiki/Microalbuminuria" \o "Microalbuminuria" microalbuminuria or GFR<60 mL/min. 14. prolonged psychosocial stress
Clinical Types of IHD(modes of presentations). 1.Angina pectoris. 2.AMI. are classic&common. 3.Heart failure 4.Sudden cardiac death(SCD).5.Asymptomatic IHD i.e subclincal. Angina pectoris(Angina,Anginal syndrome). Angina defined as chest pain caused by reversible myocardial ischemia due to imbalance between myocardial O2 supply& O2 demand. Causes of angina& Major risk factorsSee under IHD). Pathophysiology of angina: normally, myocardial O2 supply = myocardial O2 demand & blood flow&normal O2 supply can→angina due to O2 imbalance .
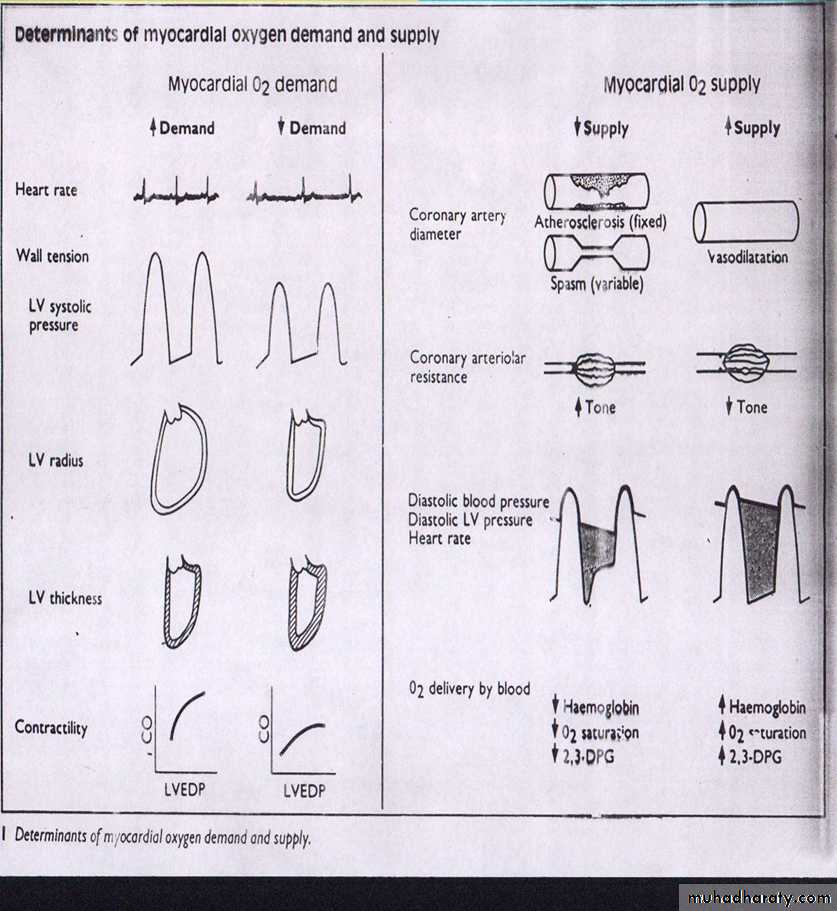
Factors determining O2 demand& O2 Supply. A.Fcators determine O2- DEMAND. 1.Heart Rate. 2.Ventricular wall tension;inturn determined by: * *LV systolic pressure *LV radius.*LV wall thickness. 3.Myocardial contractility. B.Factors determine O2-SUPPLY. 1.Coronary blood flow that inturn determined by *CA diameter. *Coronary arteriolar resistance.*Difference between diastolic blood pressure&left ventricular diastolic pressure measured as LV-end-diastolic pressure(LVEDP). *Heart rate 2. O2 availability;inturn determined by*Hb conc.*O2 saturation of blood. *Red cell 2,3 diphosphoglycerate(2,3DPG) content.
Features&clinical types of angina :--Angina has TWO main clinical types:1.Stable angina,also known as effort angina, the typical presentation of stable angina is that of chest pain or discomfort precipitated by some activity (running, walking, etc.) &greatly improved or completely relieved by rest or after sublingual nitroglycerin. Symptoms typically abate several minutes following cessation of precipitating activities and recur when activity resumes. 2.Unstable angina. (UA) is a form of acute coronary syndrome)&defined as angina pectoris that changes or worsens.It has at least one of following features:*it occurs at rest (or with minimal exertion), *usually lasting >10 min;*it is of new onset (i.e., within the prior 4–6 weeks);* and/or it occurs with a crescendo pattern (i.e., distinctly more severe, prolonged, or frequent than before) *Angina partially or not relieved by GTN.*Post-infarct angina(within 2 weeks). 3.Microvascular angina. (Angina Syndrome X) is characterized by chest pain caused by spasm of coronary arterioles. Pain often associated with SOB, sleep problems& fatigue.More common in women. It’s symptoms often are first noticed during daily activities like cooking, cleaning or going to work&at times of mental stress&less likely during physical activity (such as jogging or walking fast). 4.Prinzmetal angina(variant angina):due to critical coronary artery spasm→severe chest pain&almost always at rest,often late at night&causes are*exposure to cold stress,medication&smoking &its prognosis excellent. Symptoms of angina:Typical retrosternal chest pain is the cardinal symptom of angina.Pt.may point with clenched fist to location of chest pain at center of sternum(Levine sign)or clenched fist sign .Criteria of anginal chest pain can be eilicited by asking the patient EIGHTquestions about:*Site.*Radiation.
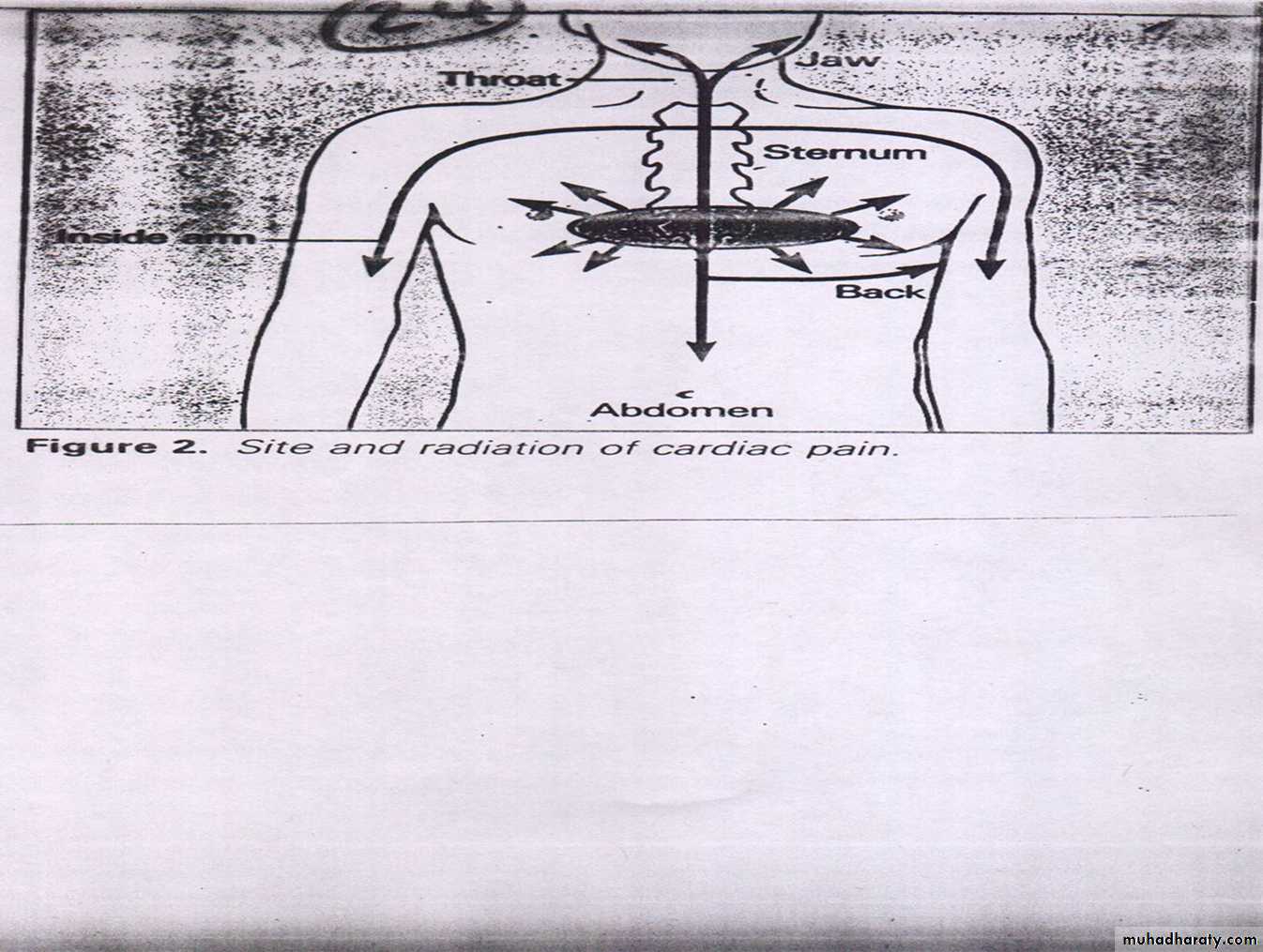
*Character.* duration. *Severity.*Associated symptoms.*Precipitating and * Relieving factors.
Signs:Often none but look for signs of possible underlying cause like AS→basal SM&search for RFs like hyperlipidemia,HTN&smoke stain etc.