OBTURATION
The three-dimensional filling of the entire root canal system as close as possible to the cementodentinal junctionAmerican Association Of Endodontists (AAE), 1994
• definitionRATIONALE FOR OBTURATION
“Bacteria are the primary source of persistent periradicular inflammation and endodontic failure”(Ingle & Bakland, 5th Ed)
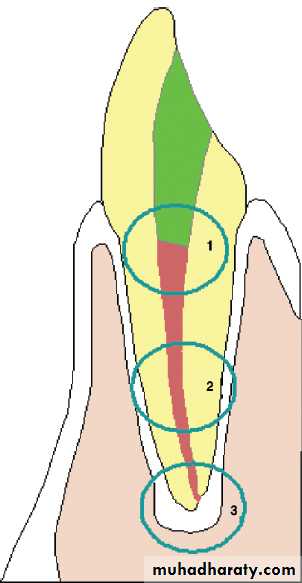
• Coronal seal
Lateral seal:Apical seal
When to Obturate ??Tooth is asymptomatic, or very mildly symptomatic with definite, ongoing symptom resolution
Canal preparation dries completely to its terminus
Canal is relatively “free” of bacteria
No foul odor is noted upon canal system entry
Temporary restoration intact and uncompromised
No sinus tract is present (debatable)
No signs of active infection
Grossman’s Criteria (1940)
Easily introducedSeal laterally as well as apically
Not shrink after being inserted
Impervious to moisture
Bacteriostatic
• Ideal requirements of root canal filling materials
Radiopaque
Not stain tooth
Not irritate periradicular tissues
Sterile or sterilizable
Easily removed
• classification
OBTURATING MATERIALS
Core materials
sealers
MetalsPlastics
Pastes/ Cements
Plastics
Cements
Pastes
CORE FILLING MATERIALS
• Metal• Silver
• Stainless steel files
Gold
Iridioplatinum
Tantalum
Titanium
• Amalgam
Plastics
GP
Hydron
Resilon
Pastes/ Cements:
N2 – Sargenti technique
Resorcinol – formaldehyde resin (Russian Red Cement)
Calcium phosphate cement (CPC)MTA
GP/Sealer Obturation Techniques
Lateral compaction (old term –“condensation”)Vertical compaction
Thermo mechanical
Thermoplasticized
Hybrid (thermo- and non Thermoplasticized combined)
Master apical impression
Lateral Compaction
Advantages
Long track recordReplicates canal adequately
Seals well
Inexpensive
Requires little armamentarium
Disadvantages
Moderately time consuming
Can vertically fracture roots
May leave vertical voids
ISO-normed and color-coded gutta percha.
Gutta percha points from various manufacturers.Gutta percha and finger
spreaders for lateral condensation.Hand spreaders with increasing sizes.
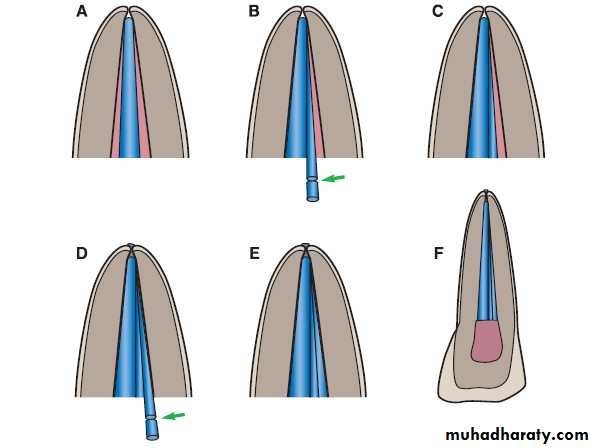
The spreader is inserted adjacent to the master
point to 1mm short of the apical foramen.Insertion and subsequent lateral condensation
of the gutta percha master point.Insertion and subsequent lateral condensation
of the gutta percha master point.Because of the irregularity of the canal walls, the gutta percha master point does not completely fill it.
Following initial condensation, the gutta
percha point is deformed and pressedagainst the canal walls.
A sealer-coated secondary gutta percha
point is inserted into the cavity.The schematic depicts the laterally condensed
gutta percha point and the spreader.The cross-section schematic shows the third
accessory gutta percha point (pink) following
lateral condensation.
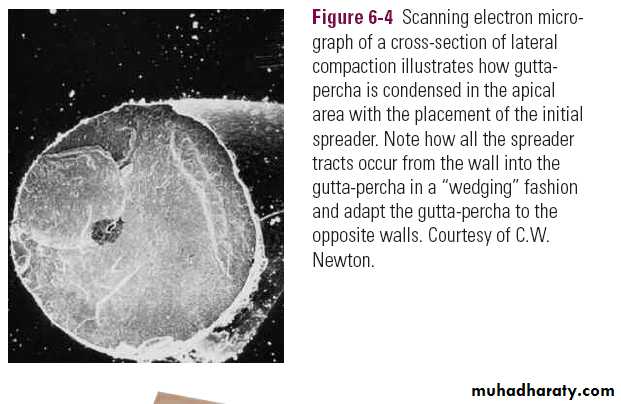
Condensation of the individual gutta percha
points leads to a homogeneous mass, whosepercentage composition of sealer is less than
5%.
Following radiographic evaluation of the master point, the point is coated with sealer and inserted into the canal with up and down movements.
Following radiographic evaluation of the master point, the point is coated with sealer and inserted into the canal with up and down movements.
Following radiographic evaluation of the master point, the point is coated with sealer and inserted into the canal with up and down movements.
With a size 30 finger spreader, the gutta percha points are condensed onto/into each other.
The tip of each additional gutta percha point
is dipped into sealer and then inserted intothe canal.
Condensation of the gutta percha continues until the spreader can only be inserted into the middle third of the root canal.
Following removal of the excess gutta percha
using a heated spatula, the remaining materialis vertically condensed.