1
Fifth stage
ORTHO
Part-2
د.هشام القطان
16/10/2016
Frozen shoulder
The term frozen shoulder should he reserved for a well-defined disorder characterized by
progressive pain and stiffness which usually resolves spontaneously after about 18 months.
The patient age 40-60 .
May give a history of trauma, often trivial.
Pain gradually increases in severity and Prevents sleeping on the affected side.
After several months it begins to subside But as it does so, stiffness becomes more
and more of a problem
Untreated stiffness persists for another 6-12 months. Gradually movement is
regained, but may not return to normal .
Usually there is nothing to see except slight wasting .
There may also be some tenderness .
But movements are always limited and in a severe case the shoulder is extremely
stiff.
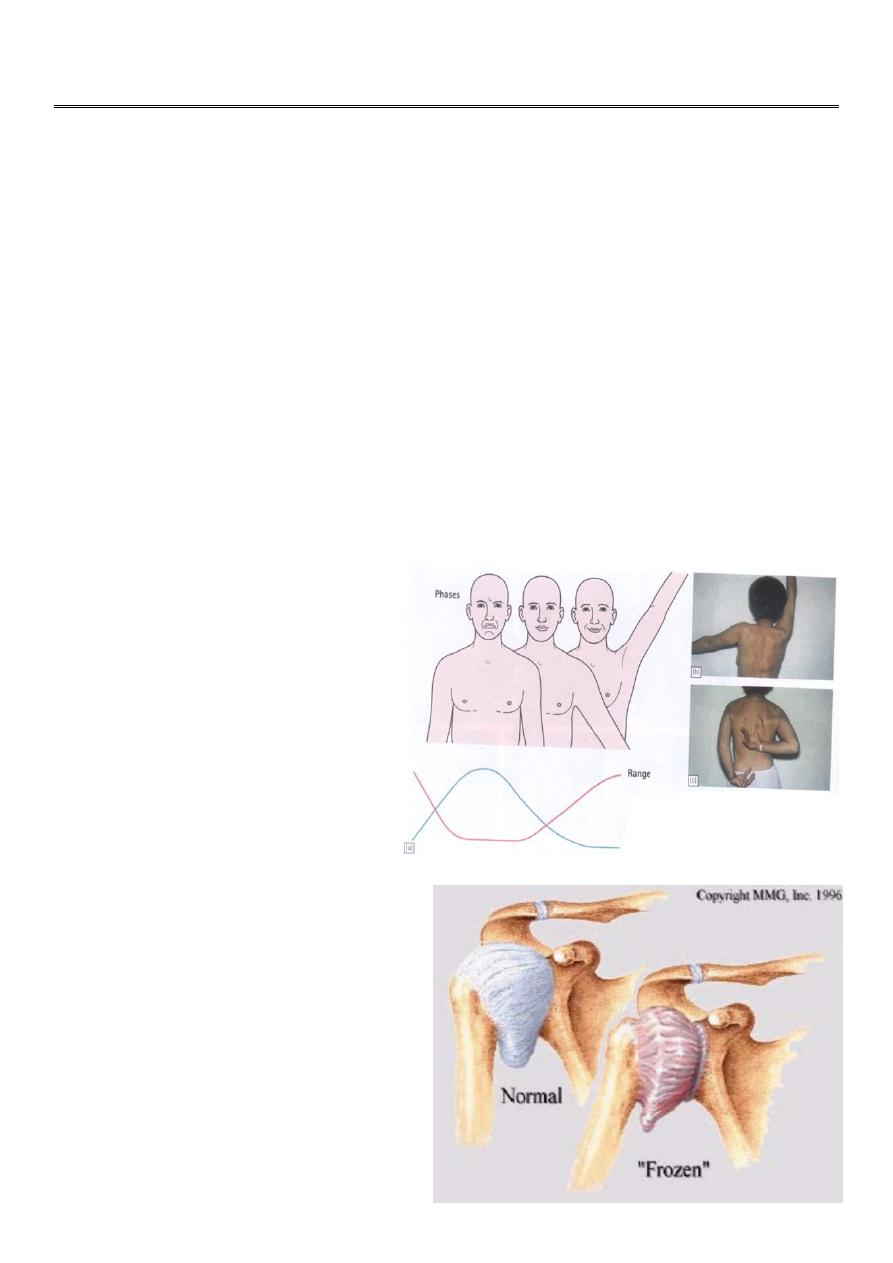
Stages :-
Freezing: Moderate diffuse
pain, normal but painful motion.
Frozen: Pain subsides, leaving
stiffness and severe decrease in
function.
Thawing: Return to normal
function gradually.
X-ray :-
Show decreased bone density in the
humerus.
Arthrography shows a contracted joint .
2
Treatment :-
1- Freezing: Try to abort in the inflammatory stage, local heat ,
NSAIDs, cortisone injection locally sometimes help ,
physiotherapy.
))= شنو موقع هالصورة معرف
2- Frozen or Thawing: Manipulation under GA if no progress with physio
*Arthroscopic release for resistant cases
-----------------------------------------------------------------------------------------------
Elbow
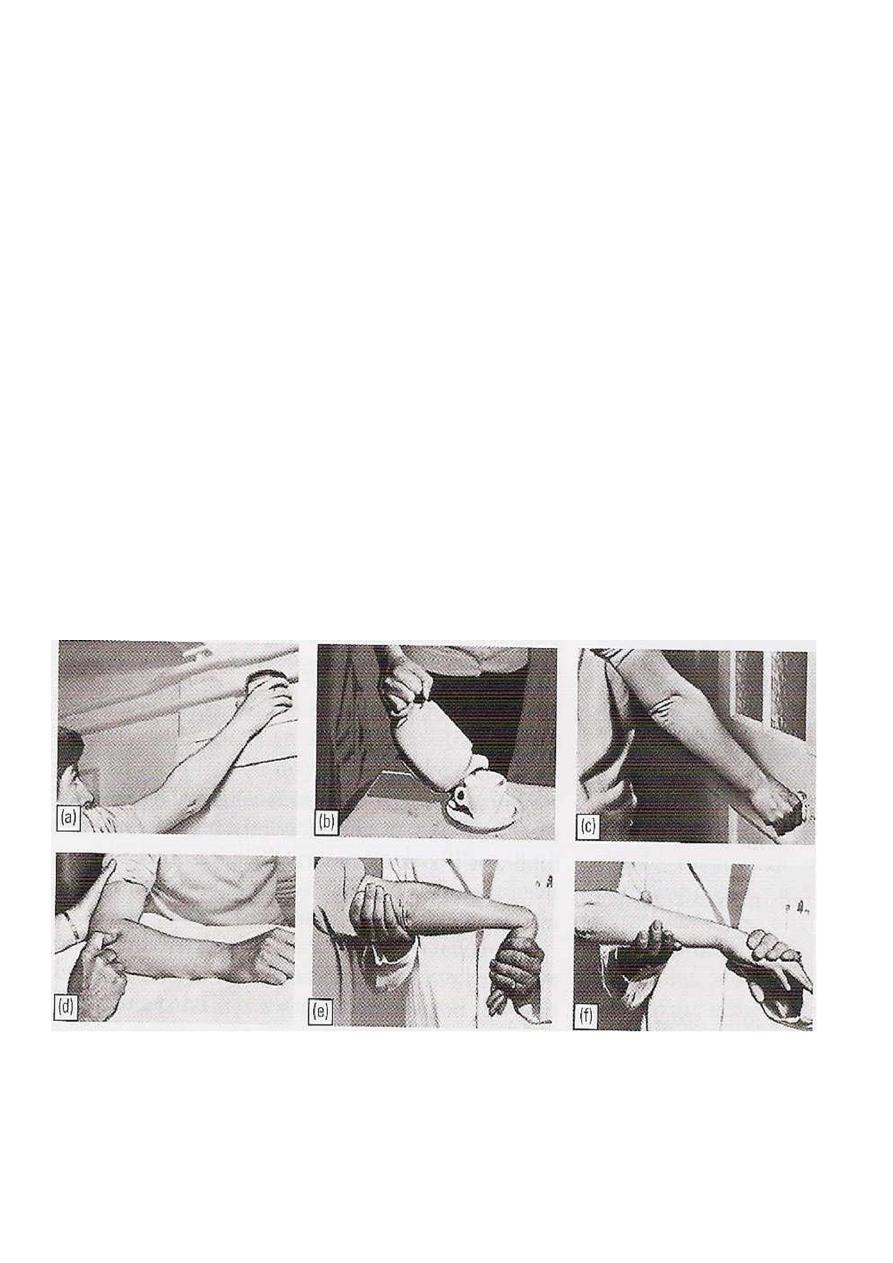
Examination :-
Both upper limbs must be complete exposed
and it is essential to look for the back as well
the front.
The neck ,shoulder and hands should also be
examined.
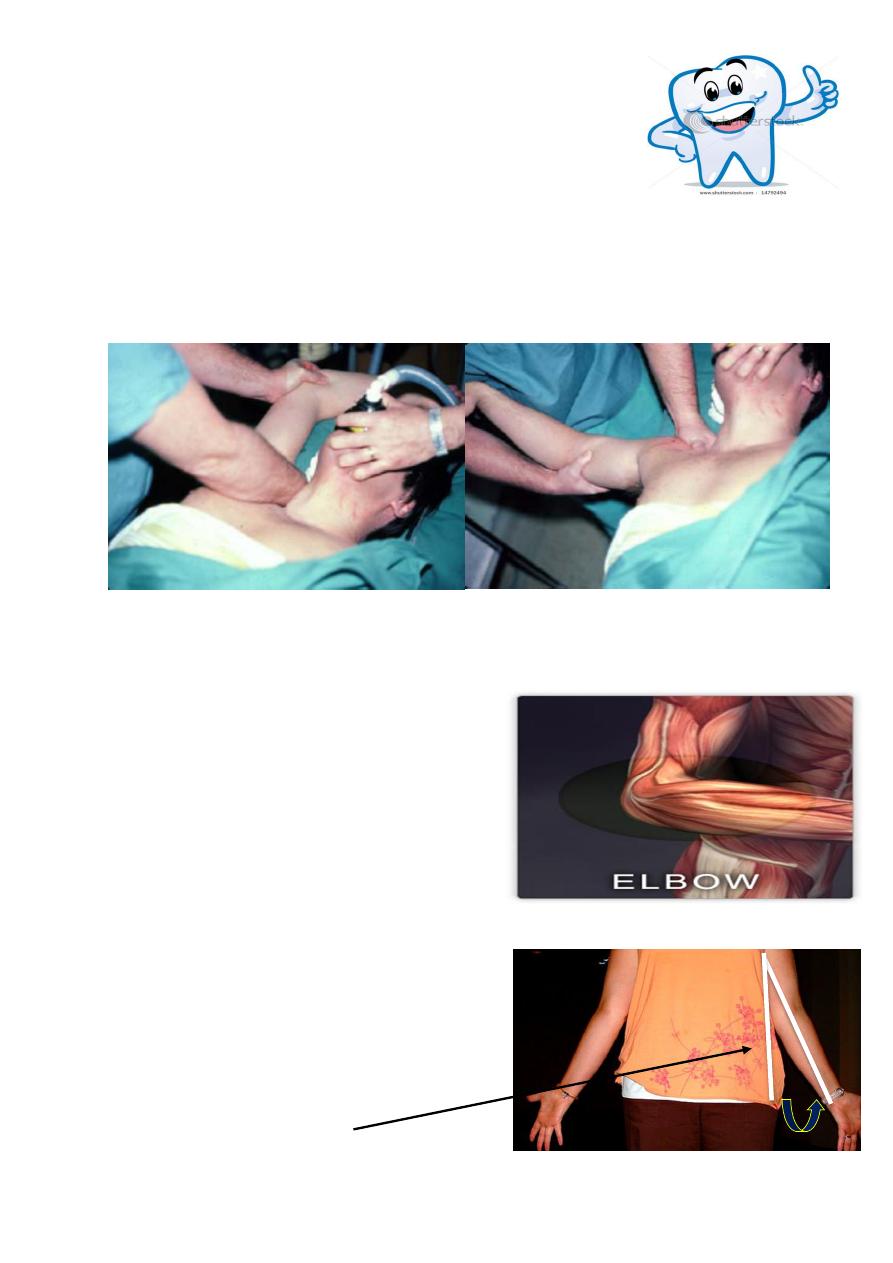
Look :-
Looking at the patient from the front with his or her
arms outstretched alongside the body and the palms
facing forward
the elbows are seen to be held in 5-10 degrees of
valgus ;
this is the normal 'carrying angle'.
Anything more, especially if unilateral, is regarded as a vaLgus deformity .
Varus deformity is less obvious.
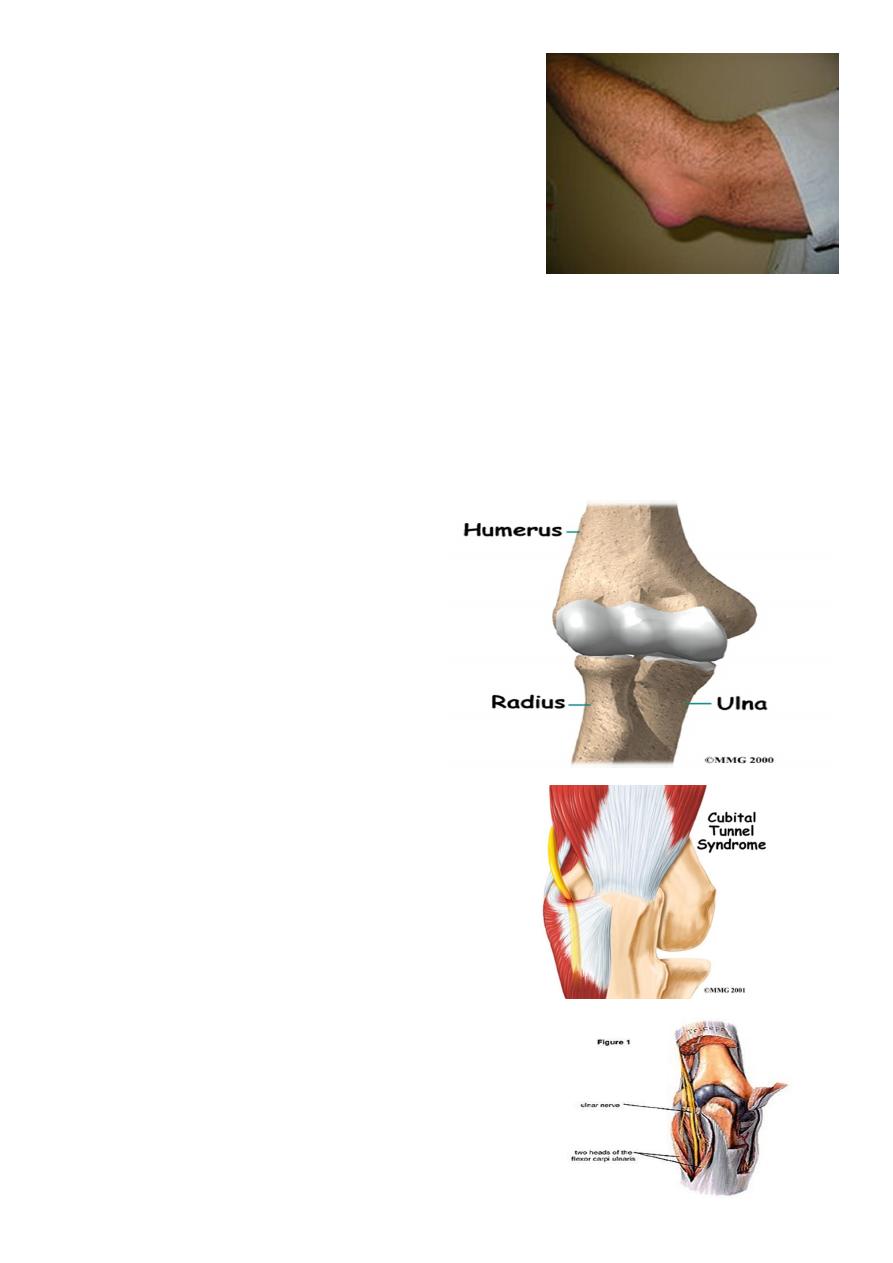
3
The most common swelling is in the olecranon bursa
at the back of the elbow
Feel :-
Important bony landmarks are the medial and lateral condyle ,and the tip of the
olecranon .
These are palpated to determine whether the joint is correctly positioned.
Superficial structures are examined for warmth and subcutaneous nodules.
The joint line (including the radioulnar joint
depression ) is located and palpated for
synovial thickening .
Tenderness can usually be localized to a
particular structure
The ulnar nerve is fairly superficial behind the medial
condyle and here it can be tolled under
4
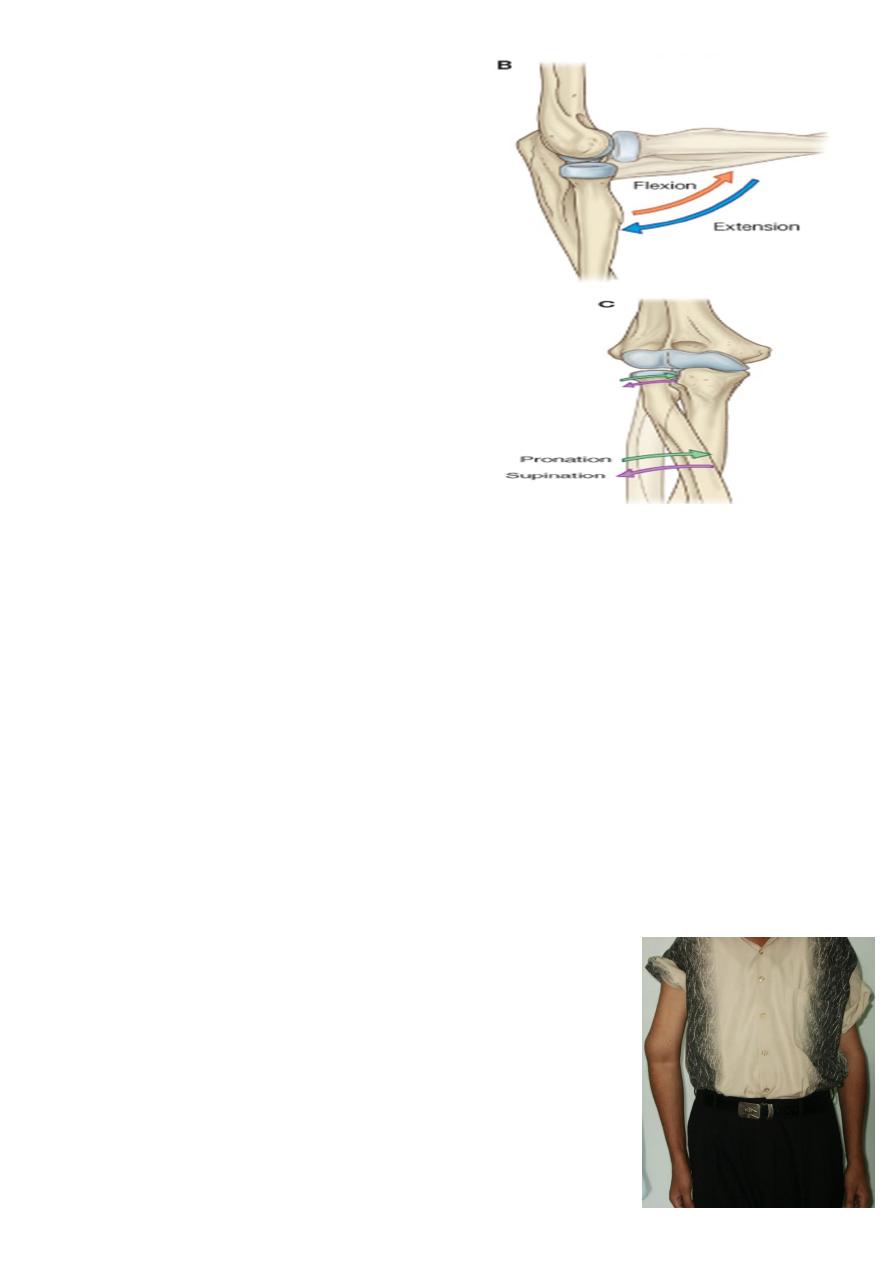
Movement :-
Flexion and extension are compared on the
two sides.
the radioulnar joints are : pronation and
supination
General examination :-
symptoms and signs do not point clearly to a local disorder ,
other parts are examined:
the neck (for cervical disc lesions)
the shoulder (for cuff lesions)
the hand (for nerve lesions)
Radiological examination:-
position of each bone is noted then the joint line and space .
Next, the individual bones are inspected for evidence of old injury or bone destruction.
Finally, loose bodies .
Elbow deformities
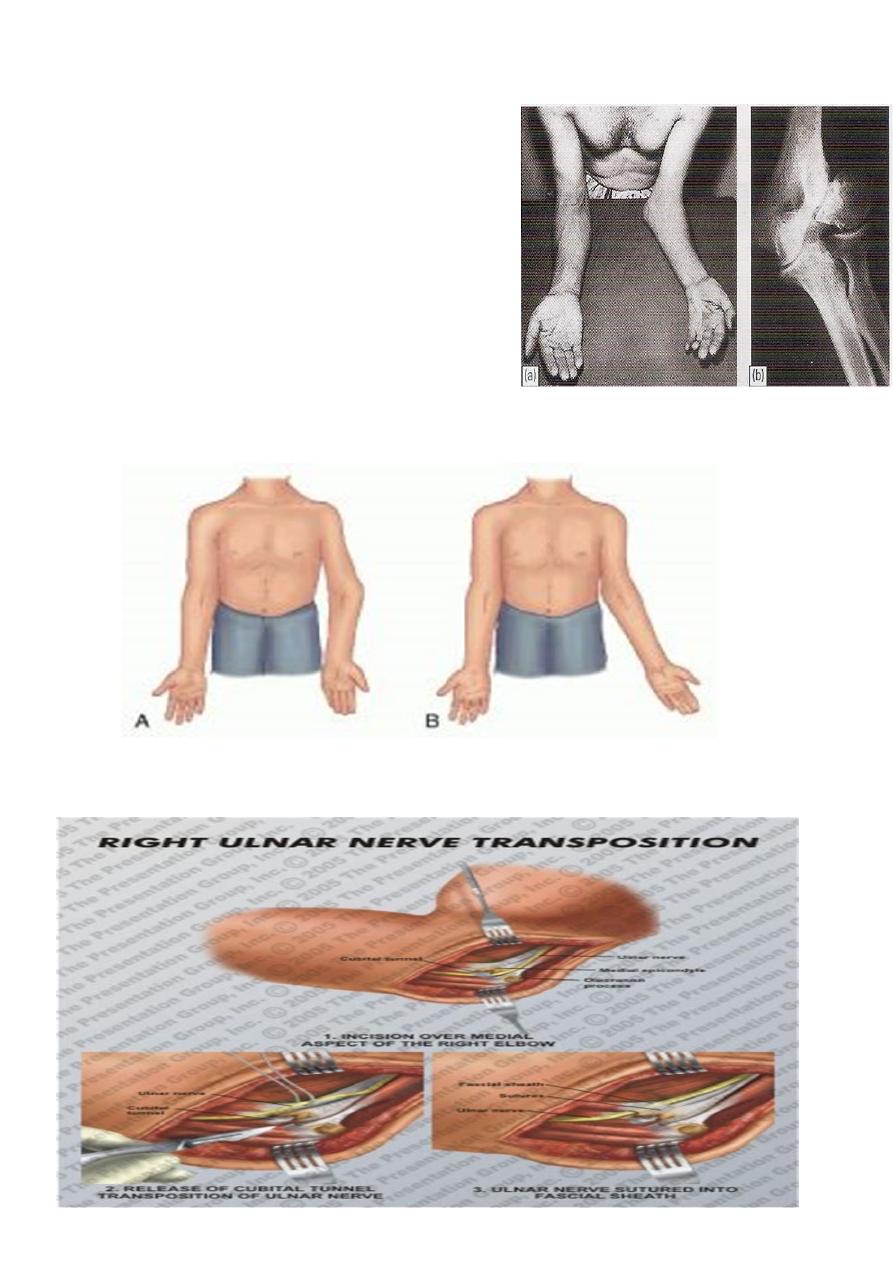
CUBITUS VARUS (or 'gun-stock') deformity :-
is most obvious when the elbows are extended and the arms are
elevated .
The most common cause is malunion of a supracondylar
fracture .
The deformity can be corrected by a wedge Osteotomy of
the lower humerus
5
CUBITUS VALGUS :-
The most common cause is non-union of a
fractured lateral condyle; this may give gross
deformity and a bony knob on the inner side of
the joint .
The importance of valgus deformity is the
liability for delayed ulnar palsy to develop;
years after the causal injury,
the patient notices weakness of the hand with
numbness and tingling of the ulnar fingers .
The deformity itself needs no treatment .
but for delayed ulnar palsy the nerve should be
transposed to the front of the elbow
A. Cubitus varus B. Cubitus valgus
6
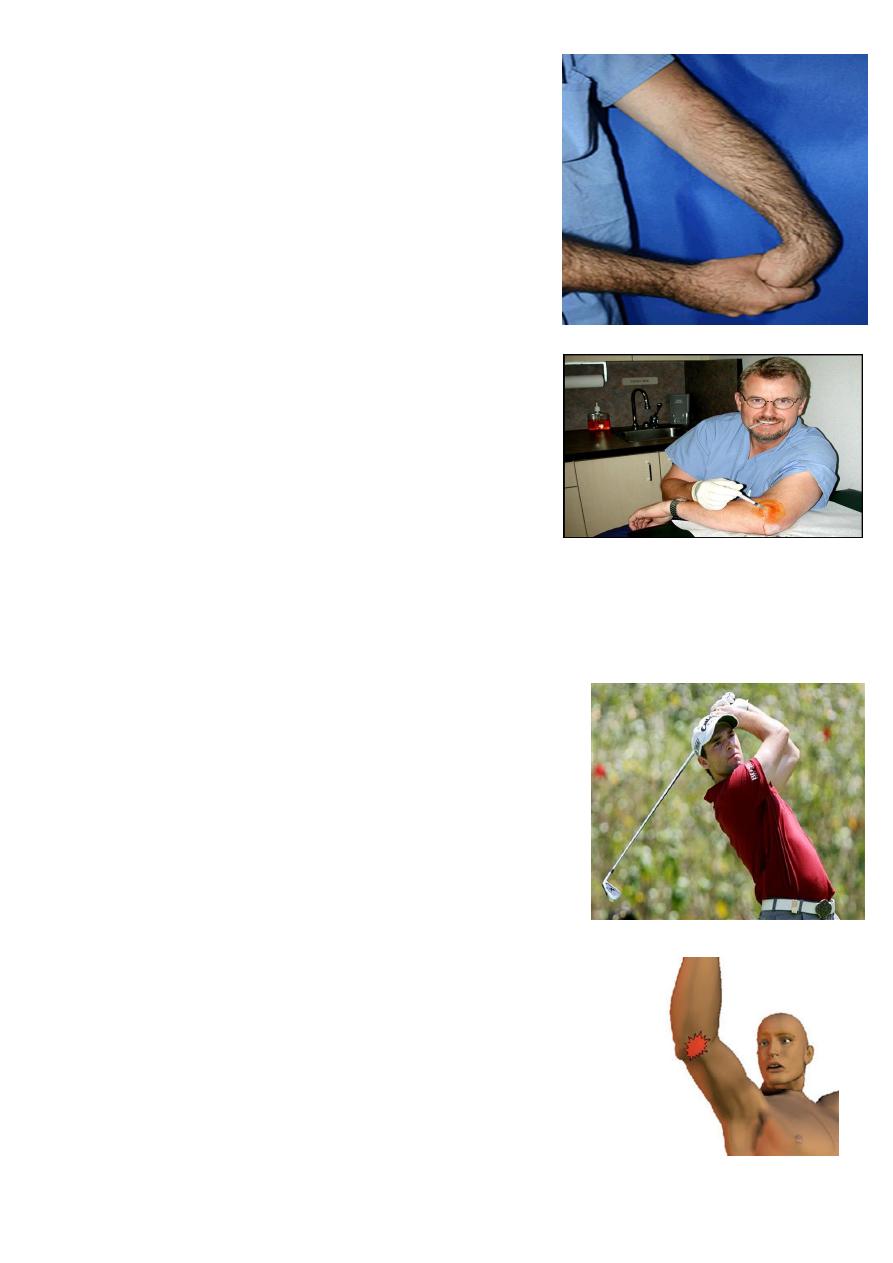
'TENNIS ELBOW'
The cause of these common disorders is unknown. Most cases follow minor trauma or
repetitive strain on the tendon aponeuroses attached to the lateral .
Pain is probably due to a vascular repair process similar to that of rotator cuff
tendinitis around the shoulder.
Often there is a history of occupational stress or unaccustomed activity.
o such as house painting,
o carpentry or
o other activities that involve strenuous wrist movements and forearm muscle
contraction
Clinical features :-
pain is felt over the outer side of the elbow .
in severe cases it may radiate widely.
It is initiated or aggravated by movements such as pouring out tea .
o turning a stiff door-handle.
o shaking hands or .
o lifting with the forearm.
The elbow looks normal and flexion and extension are full and painless .
Tenderness is localized to a spot just below the lateral epicondyle, and pain is reproduced
by getting the patient to extend the wrist against resistance.
7
Or simply by passively flexing the wrist so as to stretch
the common extensors.
Treatment :-
1- Rest and analgesia .
2- If pain is severe. the area of maximum tenderness is
injected with a mixture of corticosteroid and local
anaesthetized
.
3- Persistent pain :surgery with detachment origin at
the humeral epicondyle
'GOLFER'S ELBOW
Similar symptoms occur around the medial epicondyle and
owing to involvement of the common tendon of origin of the
wrist flexors.
pain is reproduced by passive extension of the wrist.
Treatment :-
Rest, or avoiding the precipitating activity, allow the
lesion to heal .
If pain is severe, the area 0f maximum tenderness is injected
with a mixture corticosteroid and local anaesthetic.
Persistent pain which fails to respond conservative measures
may call for operative treatment .
(((The affected common tendon on the medial side of the elbow is
detached from its origin at the humeral epicondyle))).
8
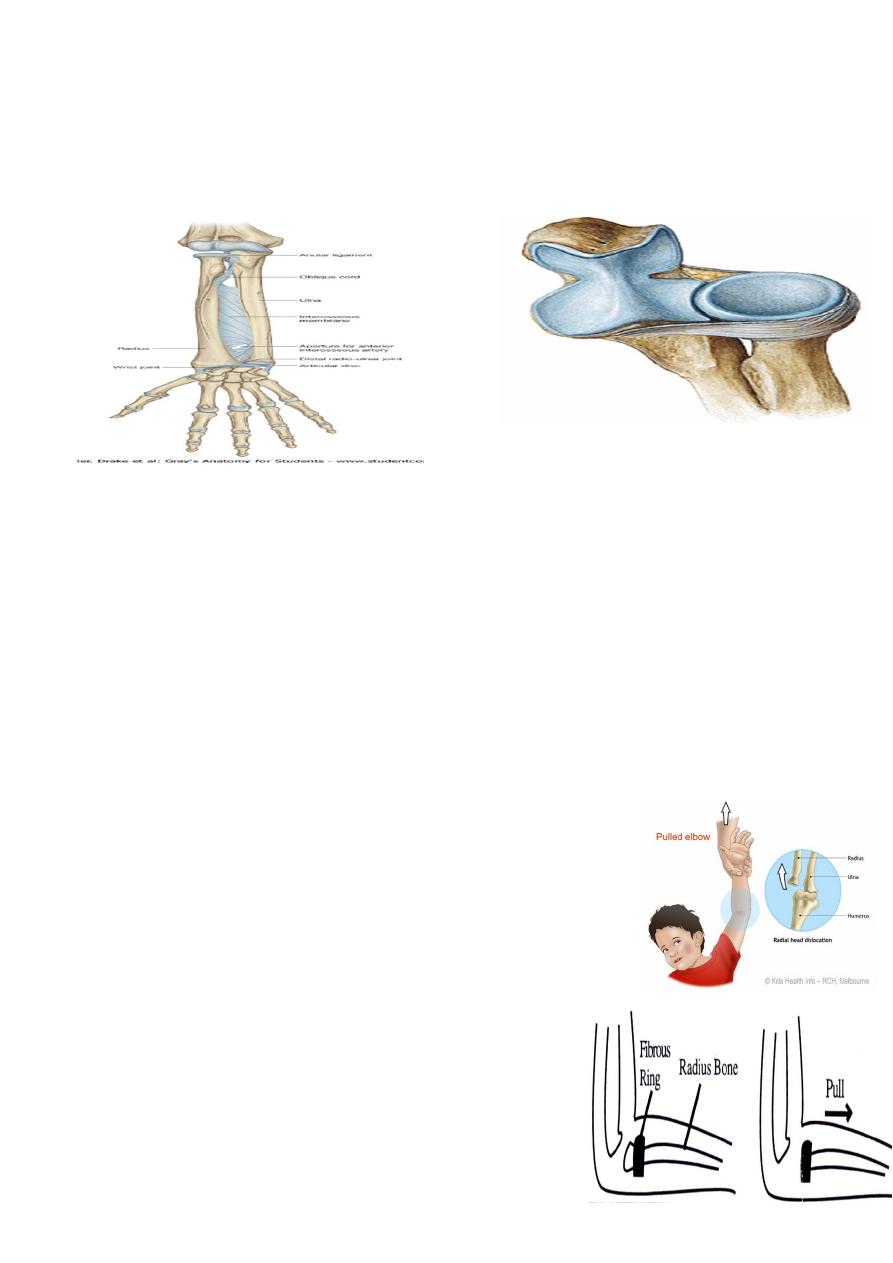
PULLED ELBOW
Nursemaids Elbow”
Anatomy :-
A pulled elbow is due to the radial head stretching the ligament and slipping out from under
its cover.
It occurs in children in the 2-6 age group ,
and is a common in young children between 1 and 4 years of age.
It is rare beyond the age of 6 years
condition that young children often get from being swung around while being held by
the lower arms It.
is most obvious when the elbows are extended and the arms are elevated.
The most common cause is malunion of a supracondylar fracture.
The deformity can be corrected by a wedge Osteotomy of the lower humerus.
commonly occurs when being grabbed suddenly by the wrist,
e.g. to prevent a child running into the road, or when a child
falls while his hand is being held.
jerky pressure on the elbow joint can pop the radial head out
from under the ligament.
This is not a considered a dislocation of the elbow, which
is extremely rare in young children.
A child will begin to cry right after the injury, and cannot
move the affected forearm because of the pain.

9
The arm is slightly bent at the elbow, and the
forearm is usually held in front of the stomach.
The patient’s history and distinct posture of the
affected forearm make the diagnosis .
An X-ray is not usually required.
Investigation :-
X rays are unnecessary if there is a typical history and no
visible swelling or deformity .
If the child has a pulled elbow the X ray is normal .
The child may have normal use of the arm on return from radiology since positioning by the
radiographer may solve the problem.
Management :-
A pulled elbow is corrected by a specific manipulation, which
is uncomfortable for a moment, a click is often felt as the
radial head pops back under the ligament .
The child will start using the arm soon afterwards.
If the elbow is not corrected with manipulation ,
the arm is rested in a sling as spontaneous correction usually
occurs within 48 hours.
You may wish to give your child pain relief.
HOW TO PREVENT THIS FROM HAPPENING
AGAIN ?
Avoid lifting or pulling a child by the hands, wrist or forearms.
Avoid swinging a child around by their wrists or forearms.
Use upper arms or arm-pits to lift the child
10
OLECRANON BURSITIS
The olecranon bursa sometimes becomes enlarged as a result of pressure or friction. When it
is also painful, the Cause is more likely to be infection , gout or
. rheumatoid arthritis.
Treatment :-
The underlying disorder must be treated .
Septic bursitis may need local drainage .
Occasionally a chronically enlarged bursa has to be excised
Your feeling when you are reading the lecture
SH.J