1
Fifth stage
Surgery
(orthopedics)
Lec-4
د.هشام القطان
16/10/2016
Upper Limbs
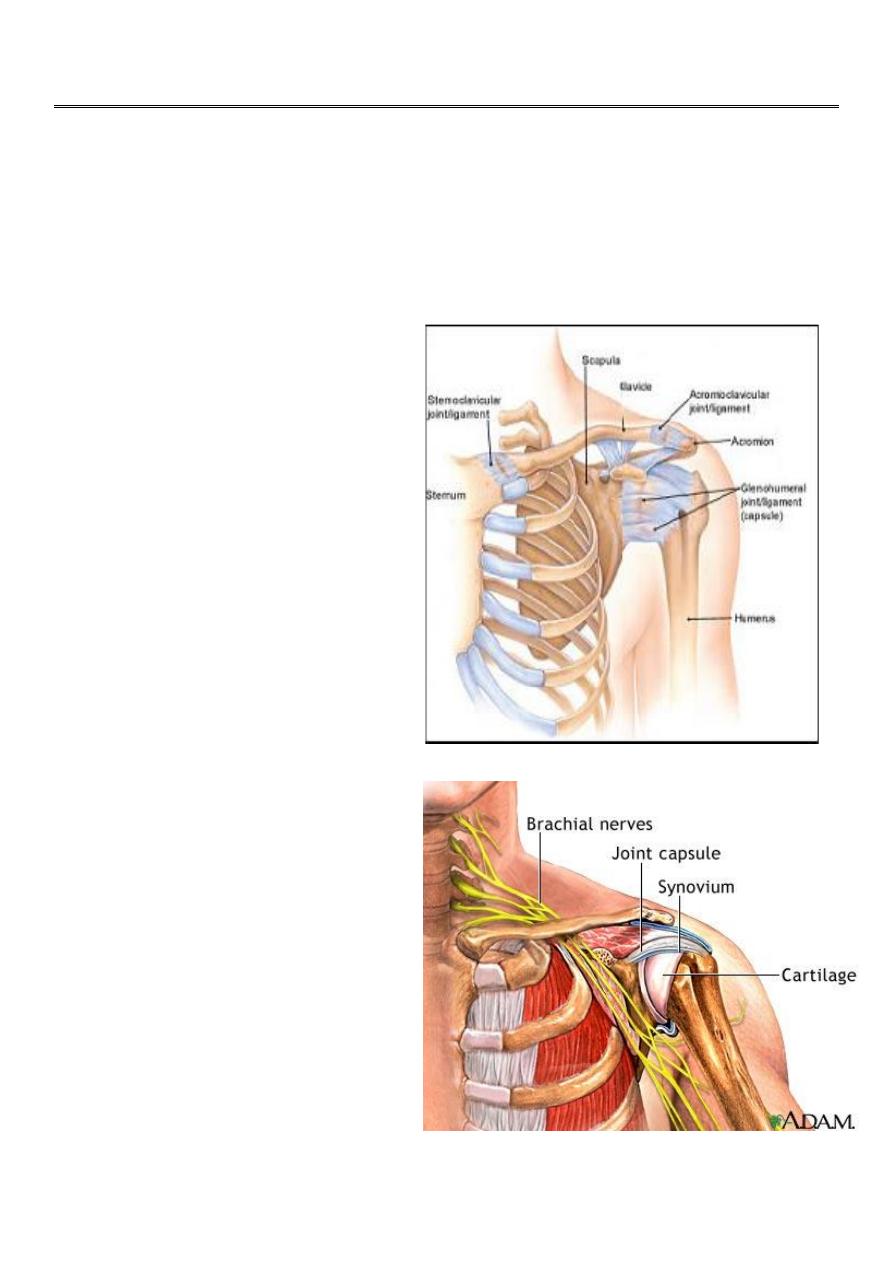
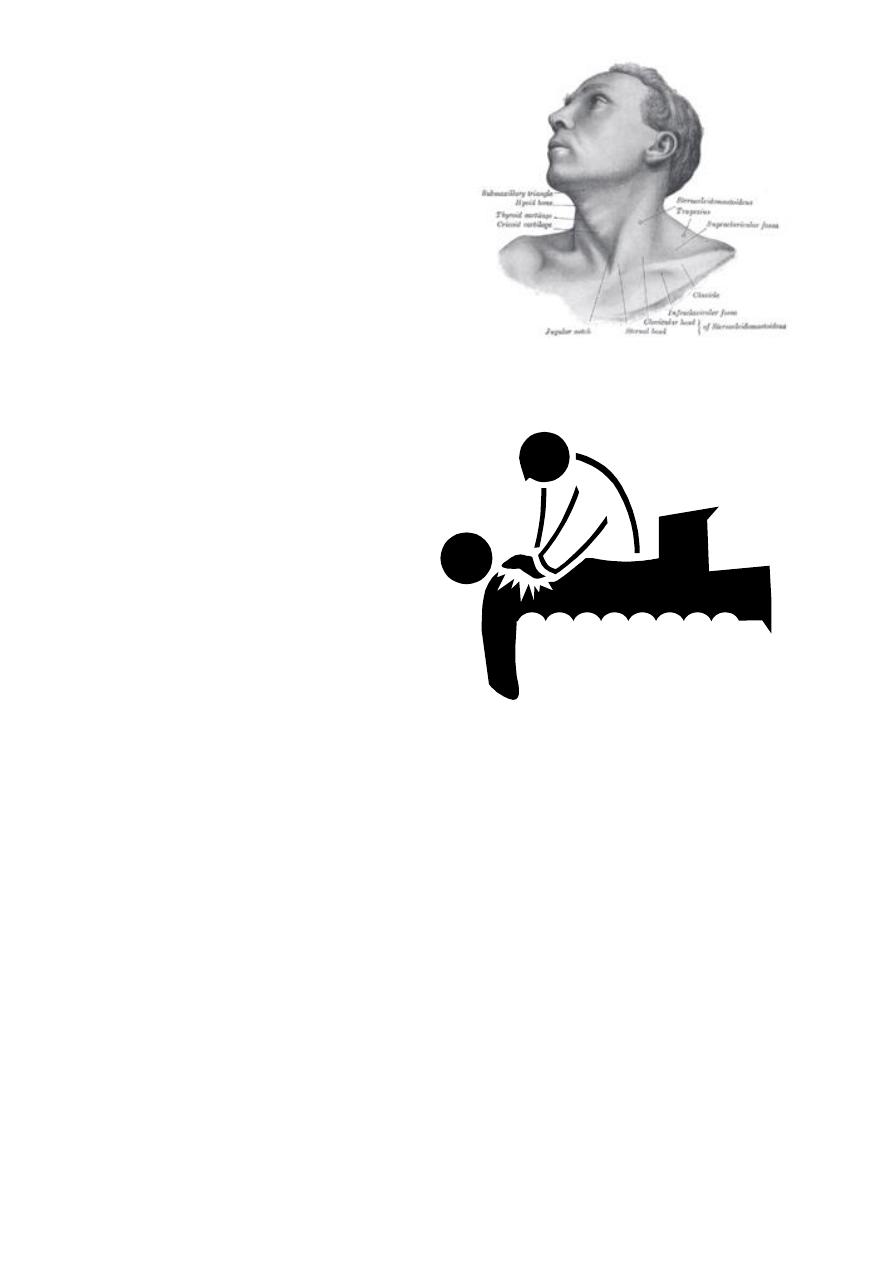
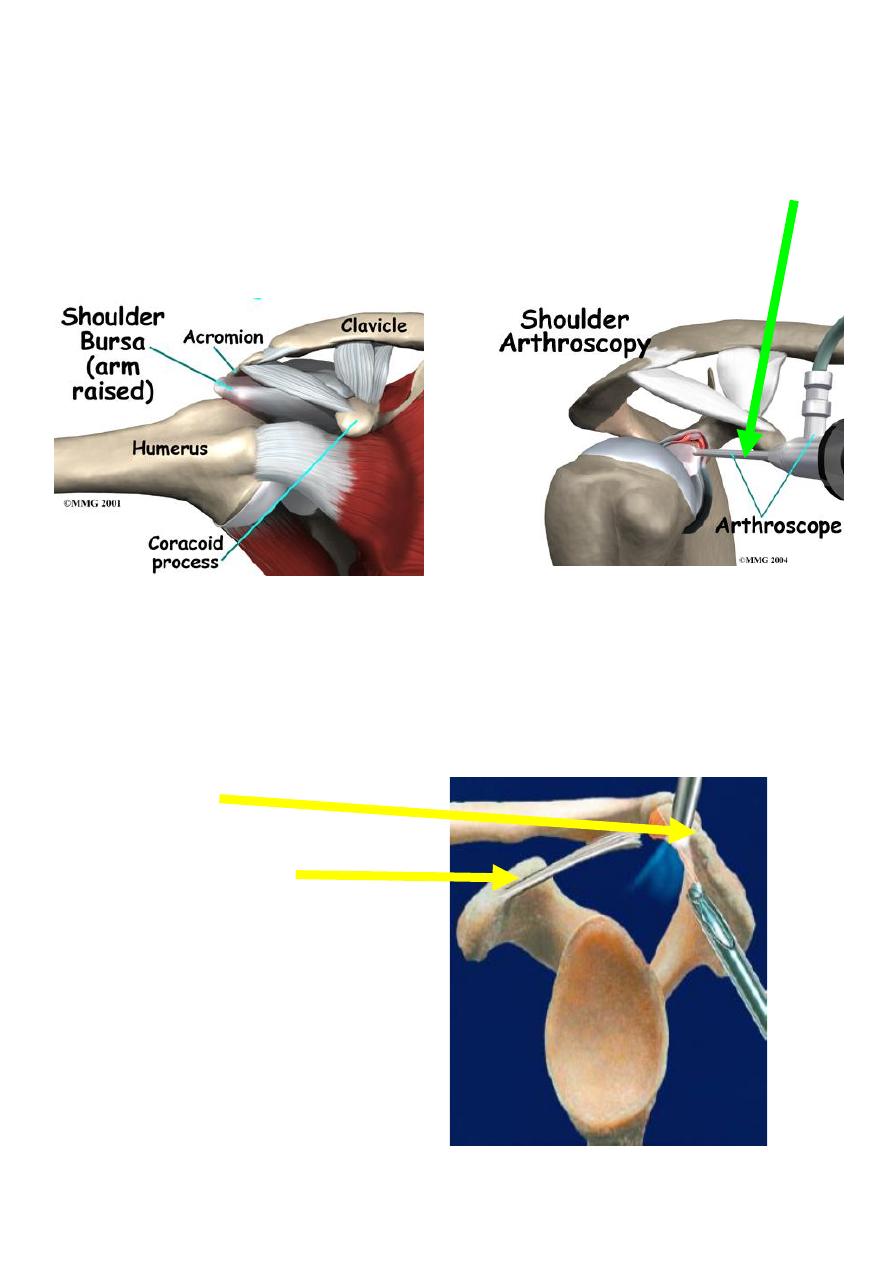
Review Anatomy of the Shoulder
The shoulder consists of four joints:
Glenohumeral.
Acromioclavicular
Sternoclavicular
Scapulothoracic
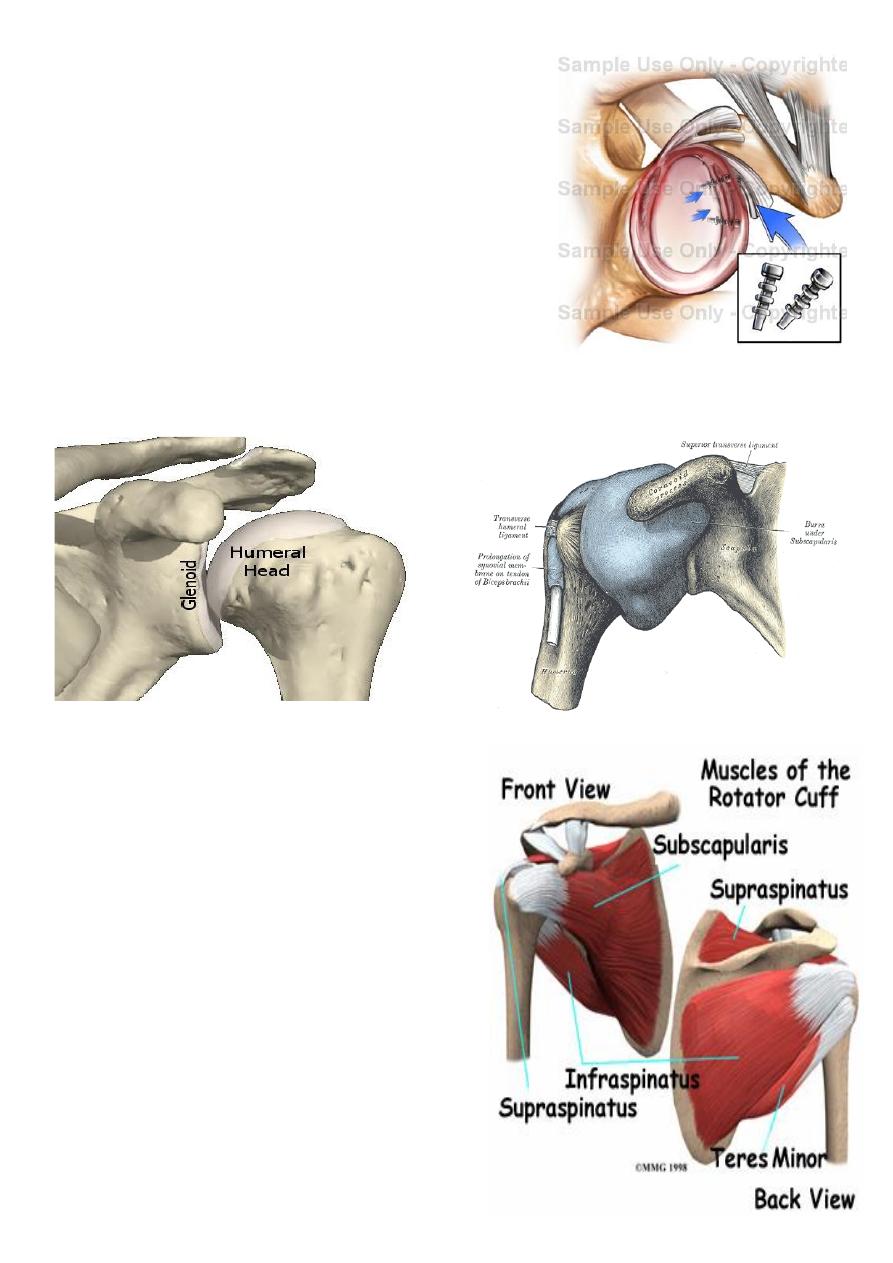
Cup and saucer joint
2
Labrum around edge of
saucer Capsule and capsular ligaments
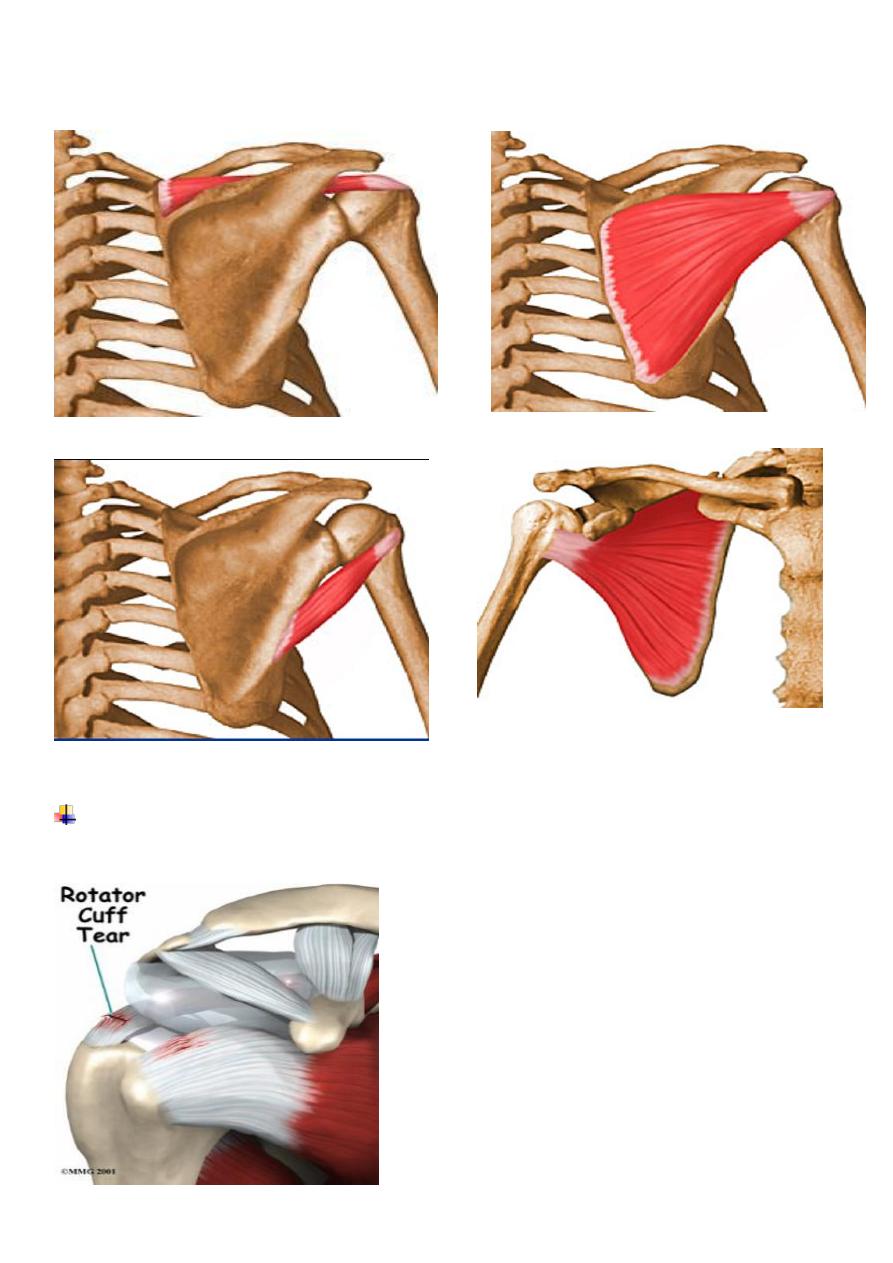
Dynamic “cuff” of muscles
Subscapularis anterior
Supraspinatus superior
Infraspinatus posteriorsuperior
Teres minor posterior
Long head of biceps intra-articula
3
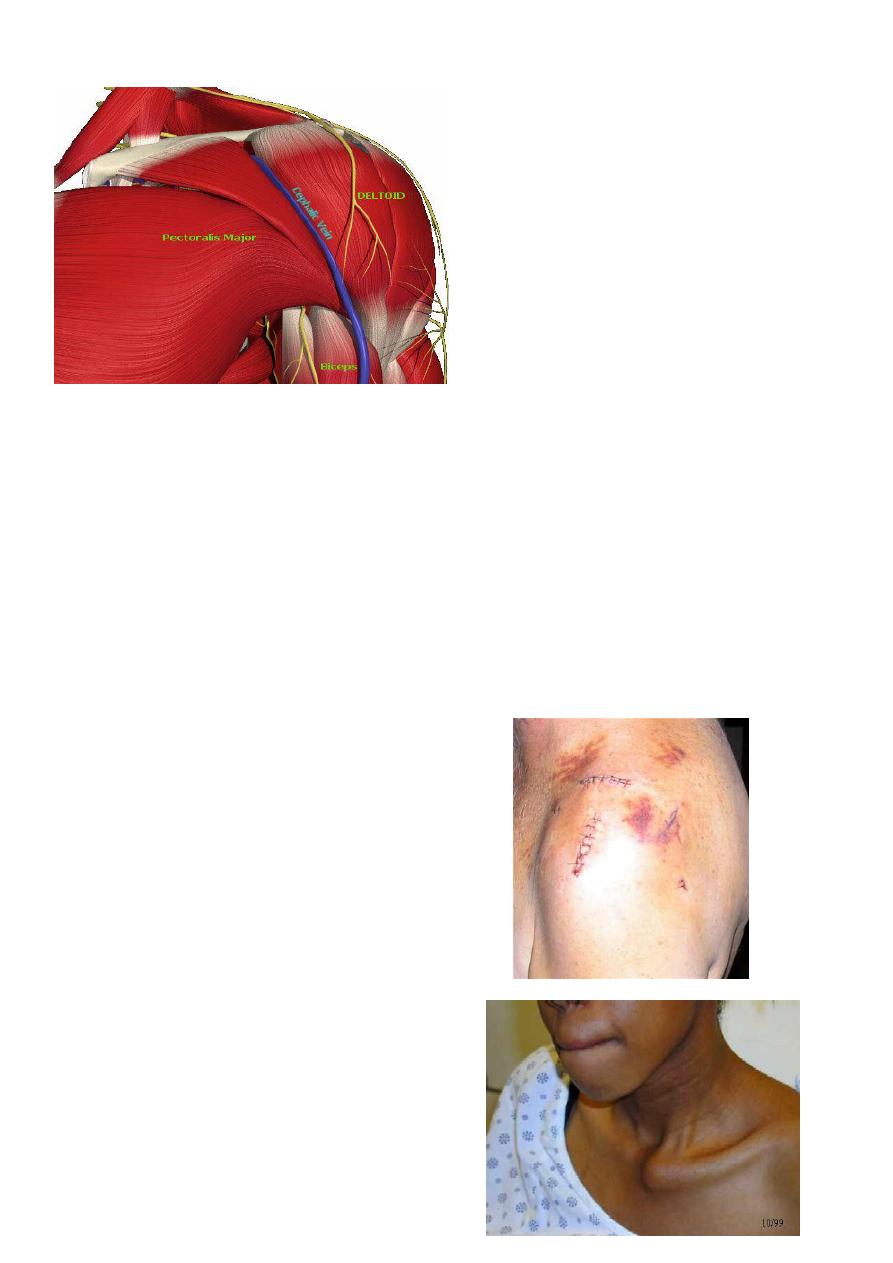
Examination
The patient should always be examined from the front and from the behind.
Both upper and the chest must be visible.
Examination of the shoulder must include a full examination of the neck and vice versa.
Basic Examination;
1. Inspection
General:
Swelling
Erythema
Joint Deformity
Muscle wasting
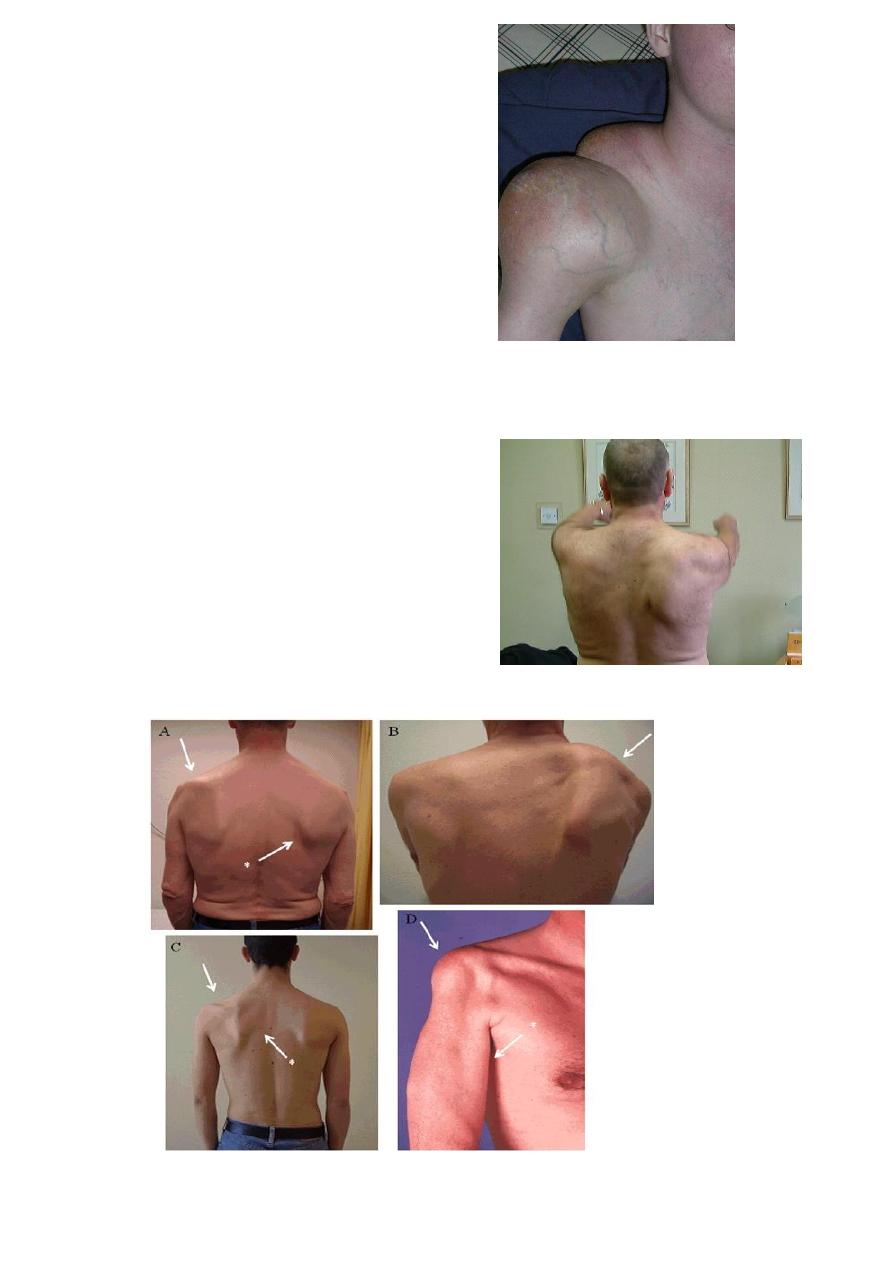
Front:
Sternoclavicular Joint prominence
Clavicle deformity
Acromioclavicular joint prominence
4
Side:
Swelling
Behind:
Scapula shape and situation
Webbing of the skin
Winging
5
Above:
Clavicle
Supraclavicular fossa
Swelling
2. Palpation
Heat
Crepitations
Bony tenderness
Humeral head and shaft
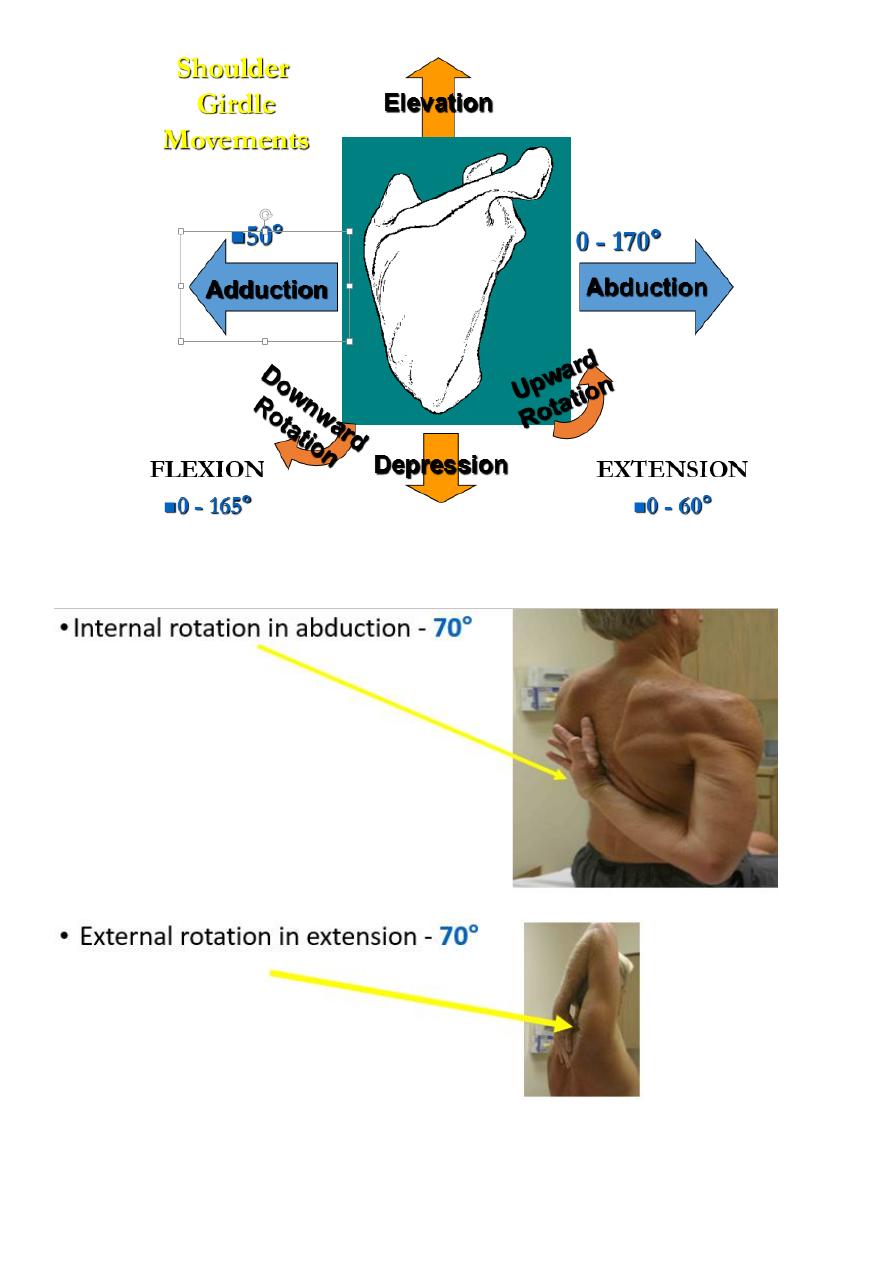
3. Movement
Active before passive
6
7
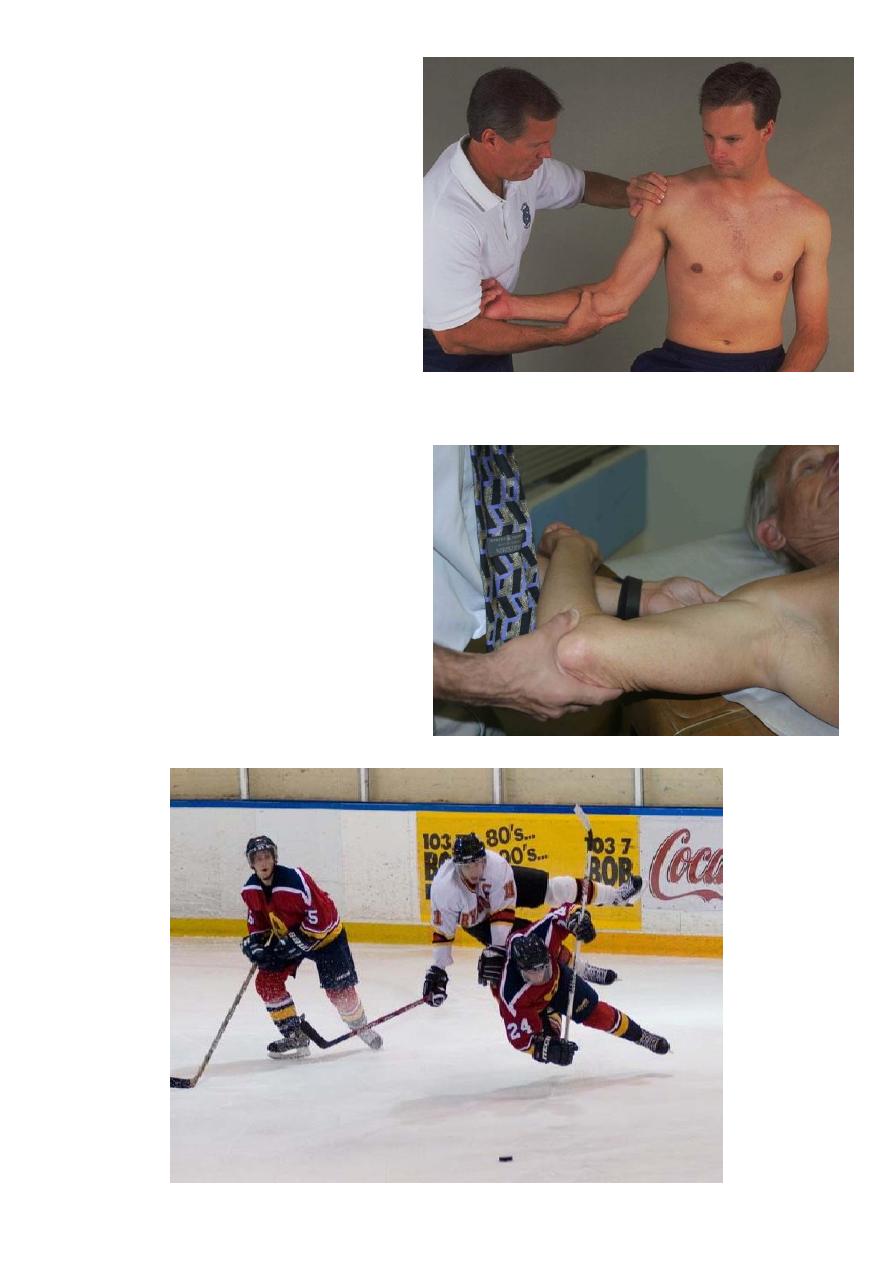
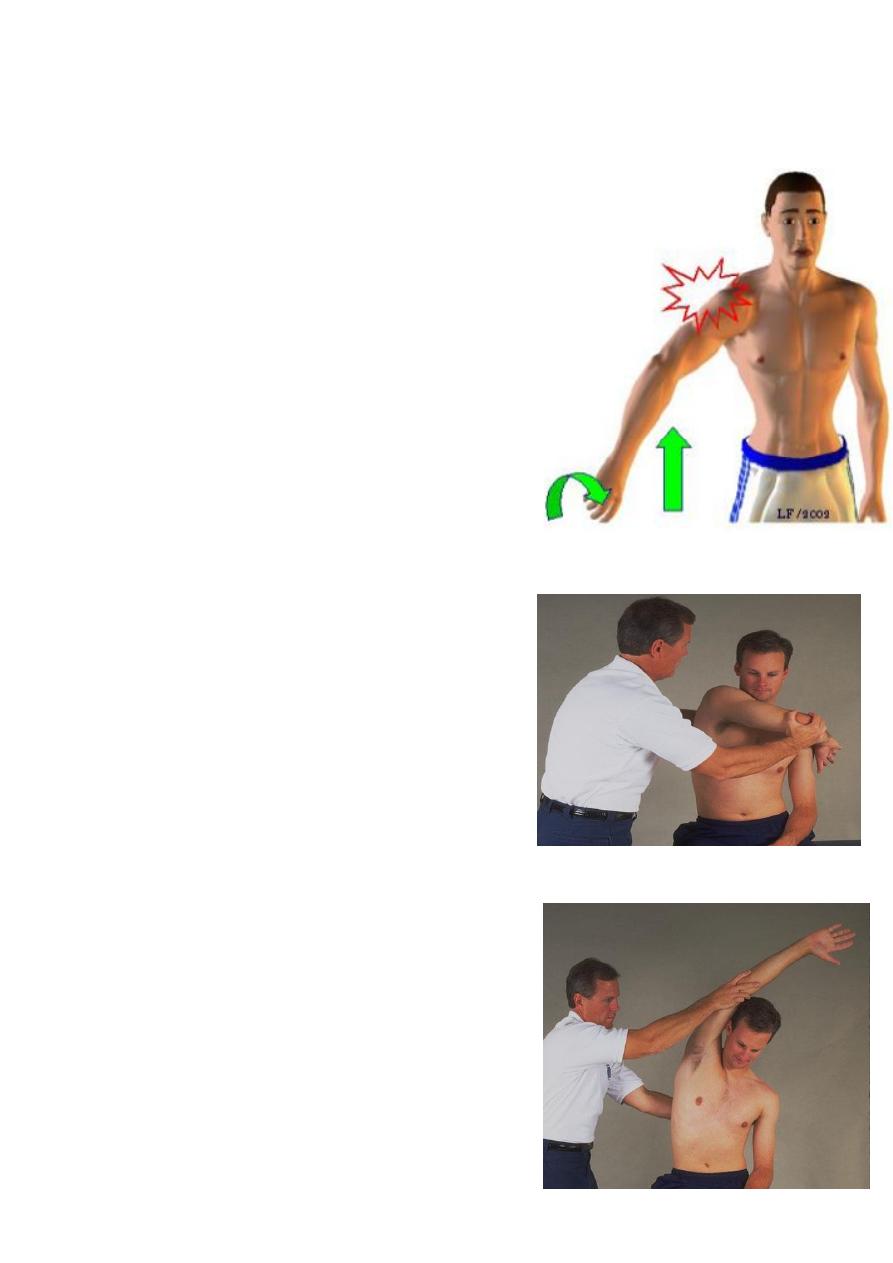
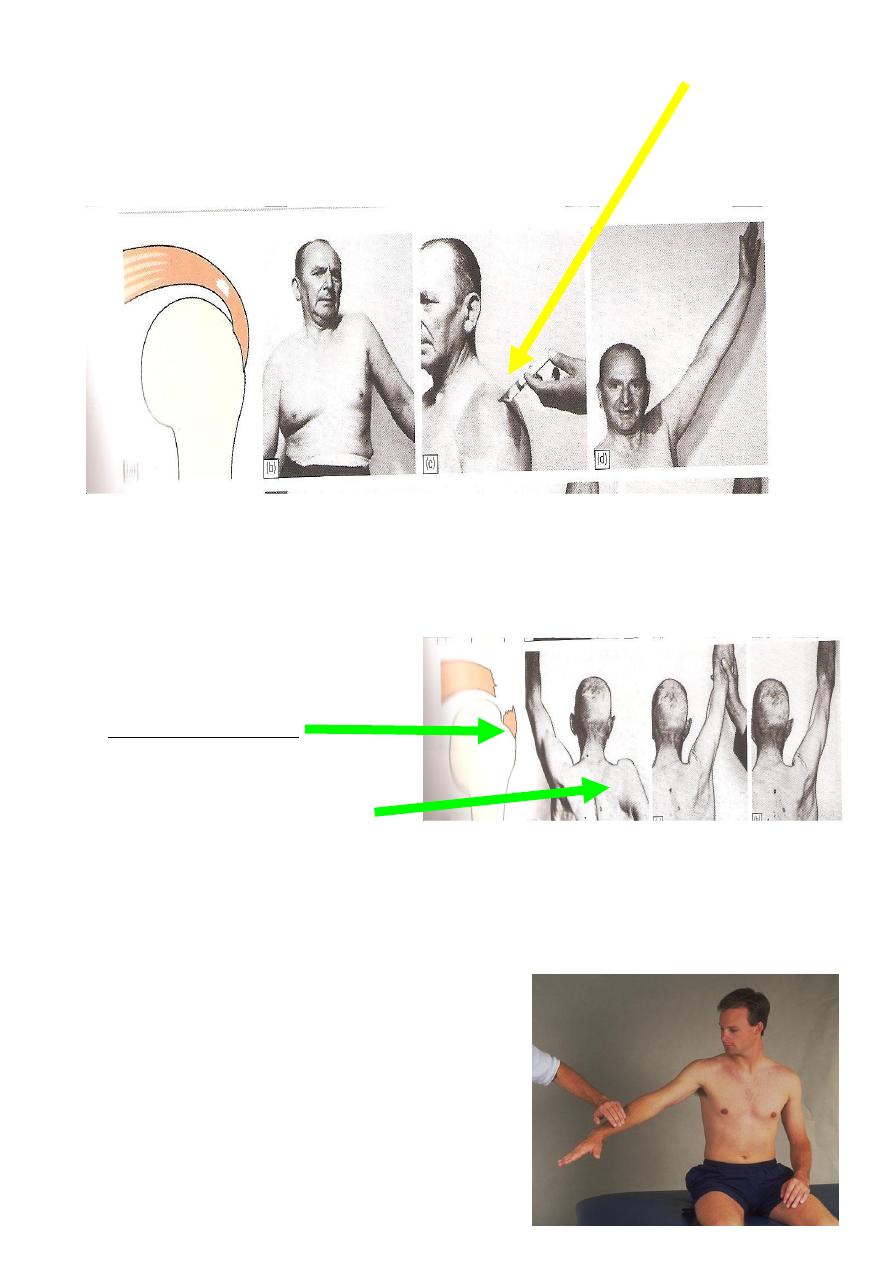
Supraspinatus Weakness
Drop Arm Test.
8
Bicep Tendon Irritation
Speed’s Test.
Apprehension tests

9
Investigations
X-ray
WBC
ESR
Blood Culture
Aspiration of the Joint
CAT
MRI
Arthroscopy
Arthography
Examination under anesthetic
Shoulder
Disorder of the rotator cuff
Acute tendinitis.
Chronic tendinitis (Impingement Syndrome).
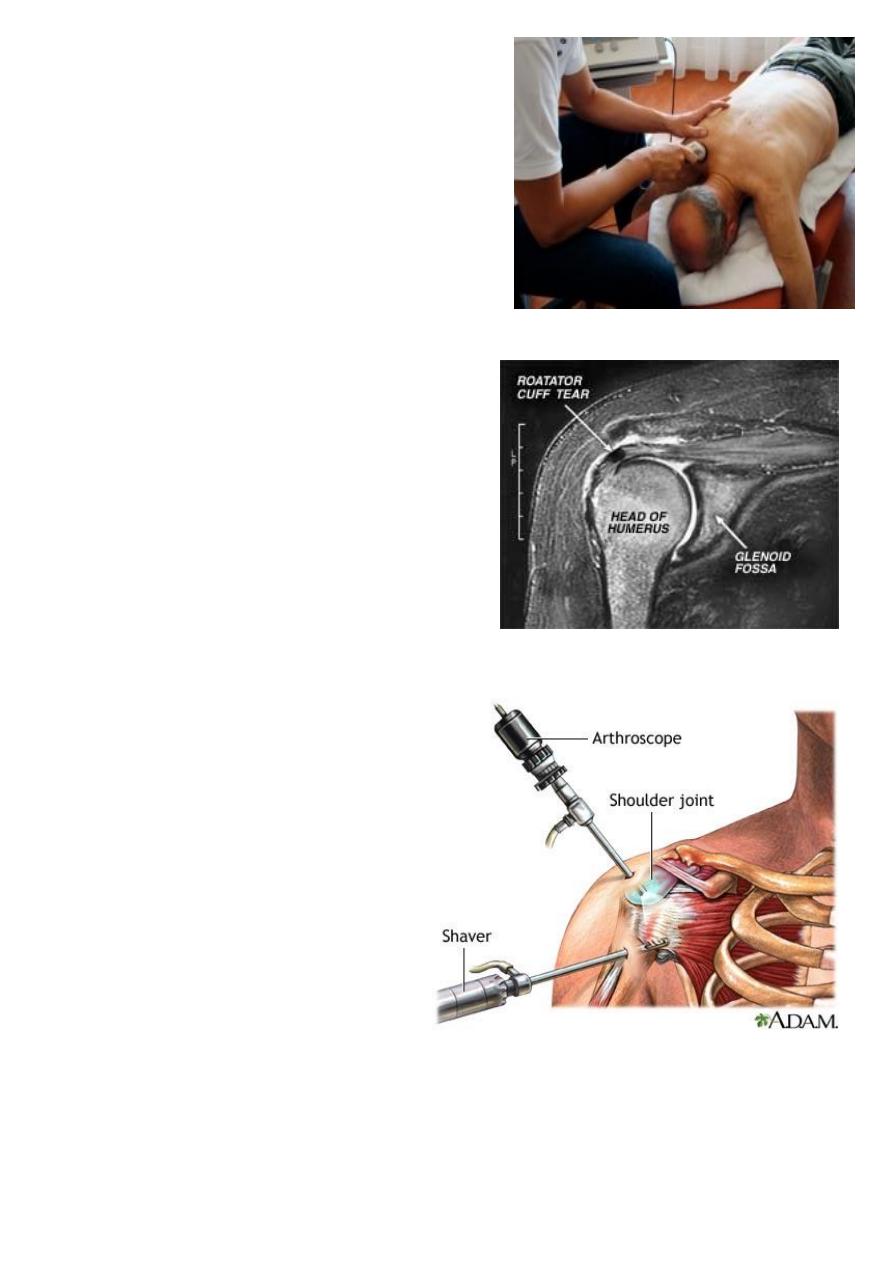
Rotator Cuff Tears.
Frozen Shoulder
.
**Supraspinatus Tendinitis acute calcific tendinitis**
Pain is caused by inflammation of the tendon and subacromial bursa.
Age of onset is
43
Men being more commonly affected
.
11
Clinical features
Rapid onset without Warning. Disturbance of sleep.
Severe pain.
Apprehension to move the arm.
Acute localised tenderness.
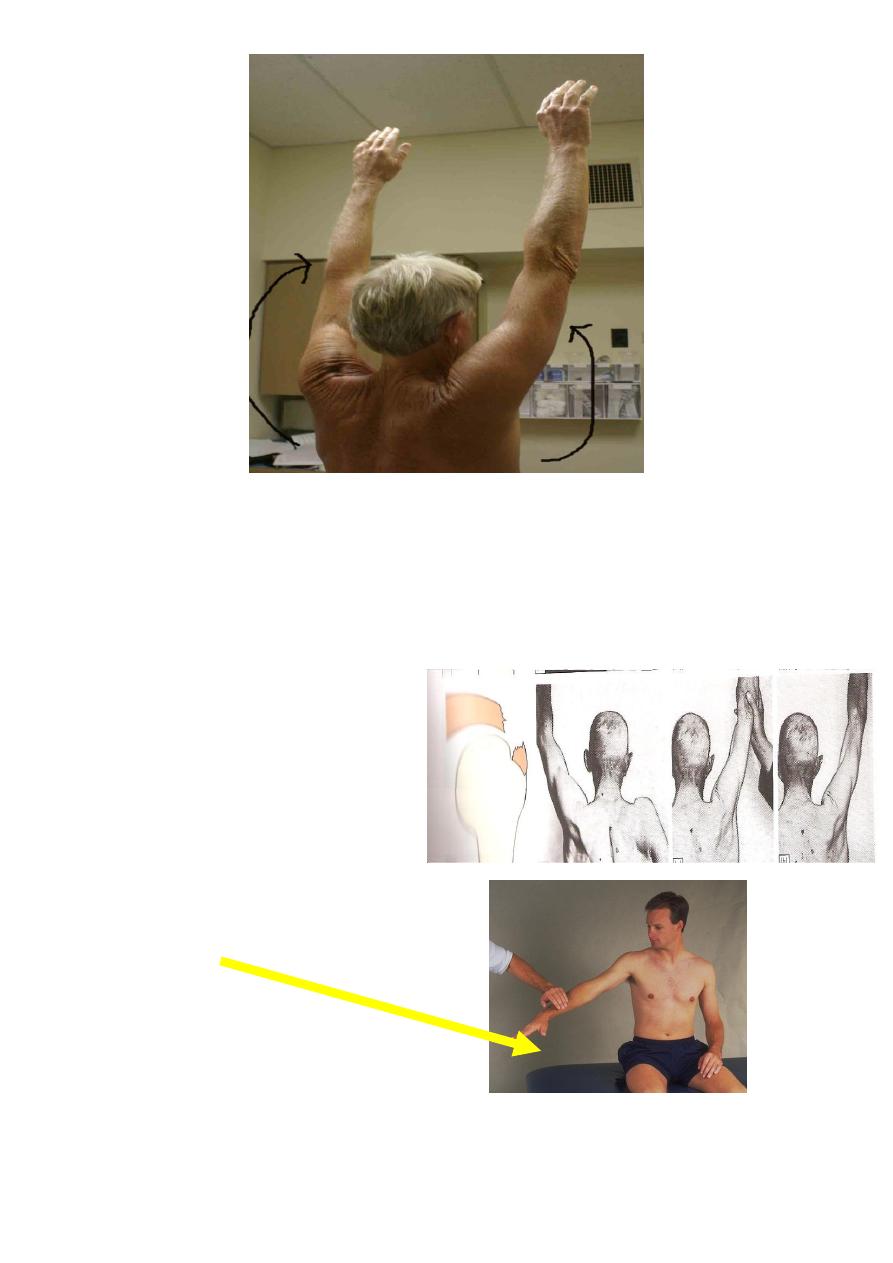
Shoulder Impingement Tests
Hawkins-Kennedy Test.
Neer’s Test
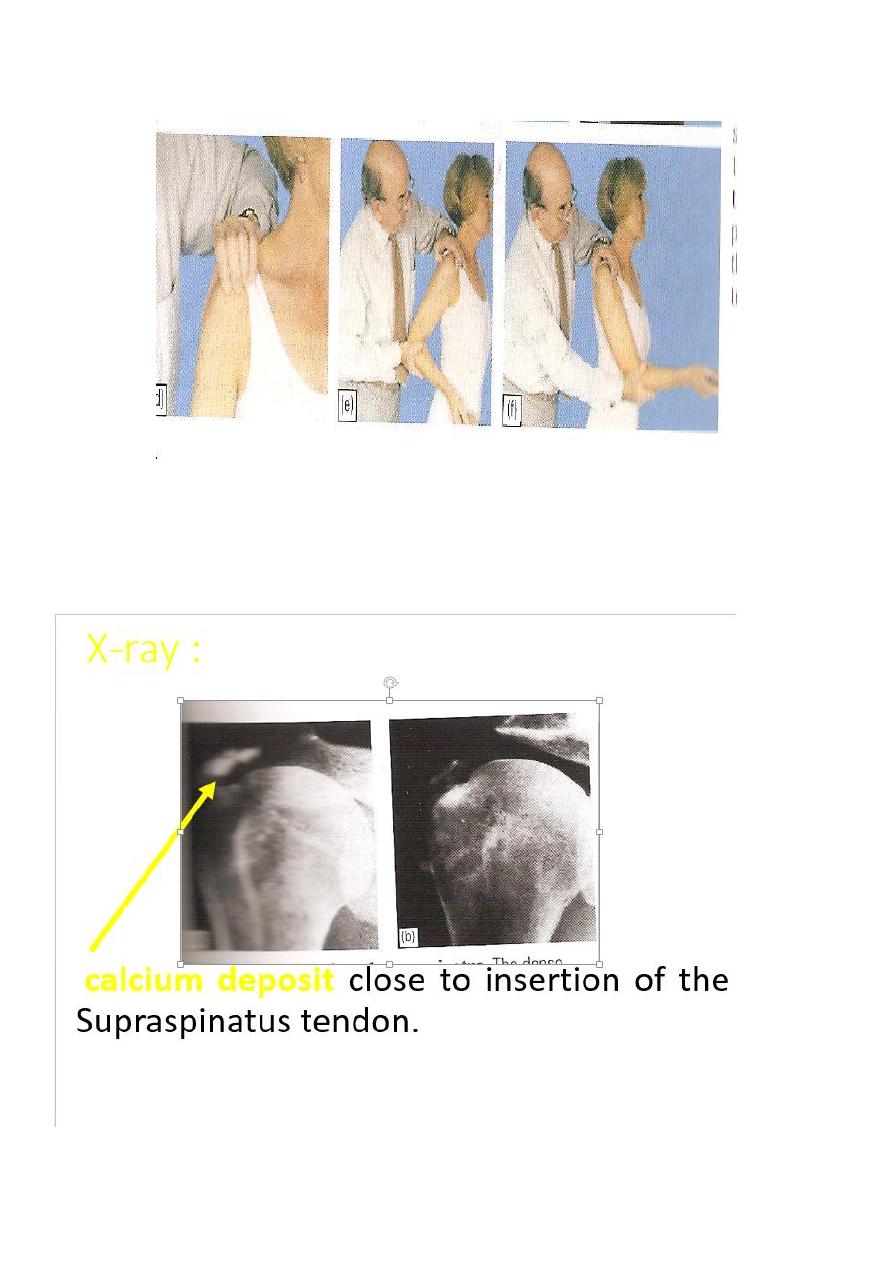
11
X-Ray
12
Treatment
mild cases :
Rest with sling.
Anti-inflammatories
Severe cases :
1. long acting steroid injections (methylprednisolone 40-80 mg).
With local anaesthetic (lignocaine 1%).
2. If symptom not relieved surgery for removal calcific material.
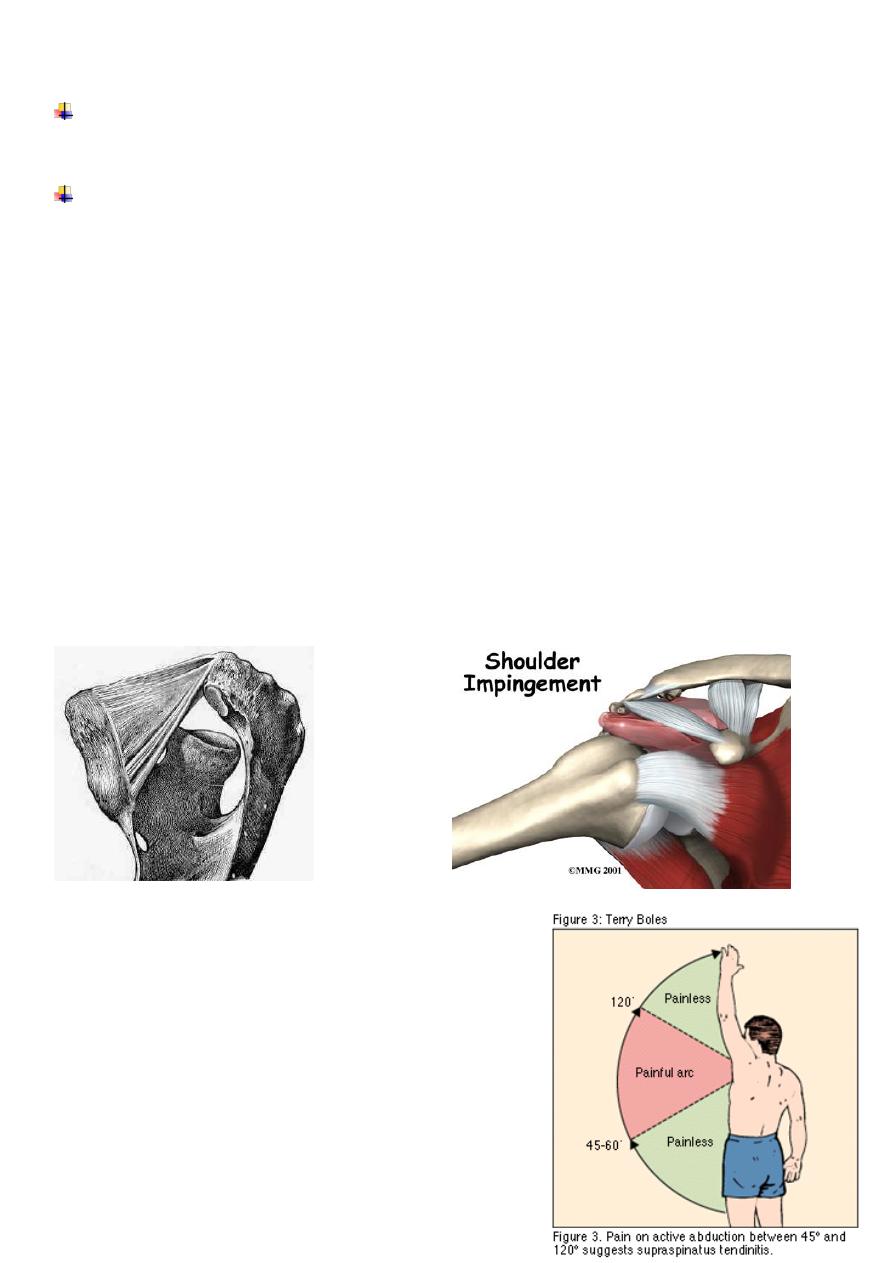
Impingement Syndrome
The pain is due to irritation of the Supraspinatus tendon.
Commonly caused by repeated overhead movements which cause pinching of the
tendon
.
The clinical features
Patient age
40-60
years.
Onset usually
insidious.
But can be sudden after overuse.
Painful lateral aspect of upper arm( over the deltoid
muscle).
Worse at night.
13
cannot lie on affected arm.
The shoulder looks normal.
Pain on overhead and behind the back movements.
Repeating the movement with the arm in full external rotation may be easier and
painless
(pathognomonic of Supraspinatus tendinitis)
Crepitus or clicking during movement.
In long standing cases wasting of the muscles
Loss of power
Movement especially abduction and external rotation are restricted
.
Treatment
Rest in the younger patient, modification of activity (i.e. not playing golf/ racket
sports).
14
In chronic cases
Physiotherapy.
Analgesics and sometimes steroid and local anaesthetic injections become necessary.
If symptoms keep recurring, operation is advisable by decompressing the
coracoacromial ligament (now a day done by arthroscopy)
Operative
Acromioplasty
Coracoacromial ligament
release
15
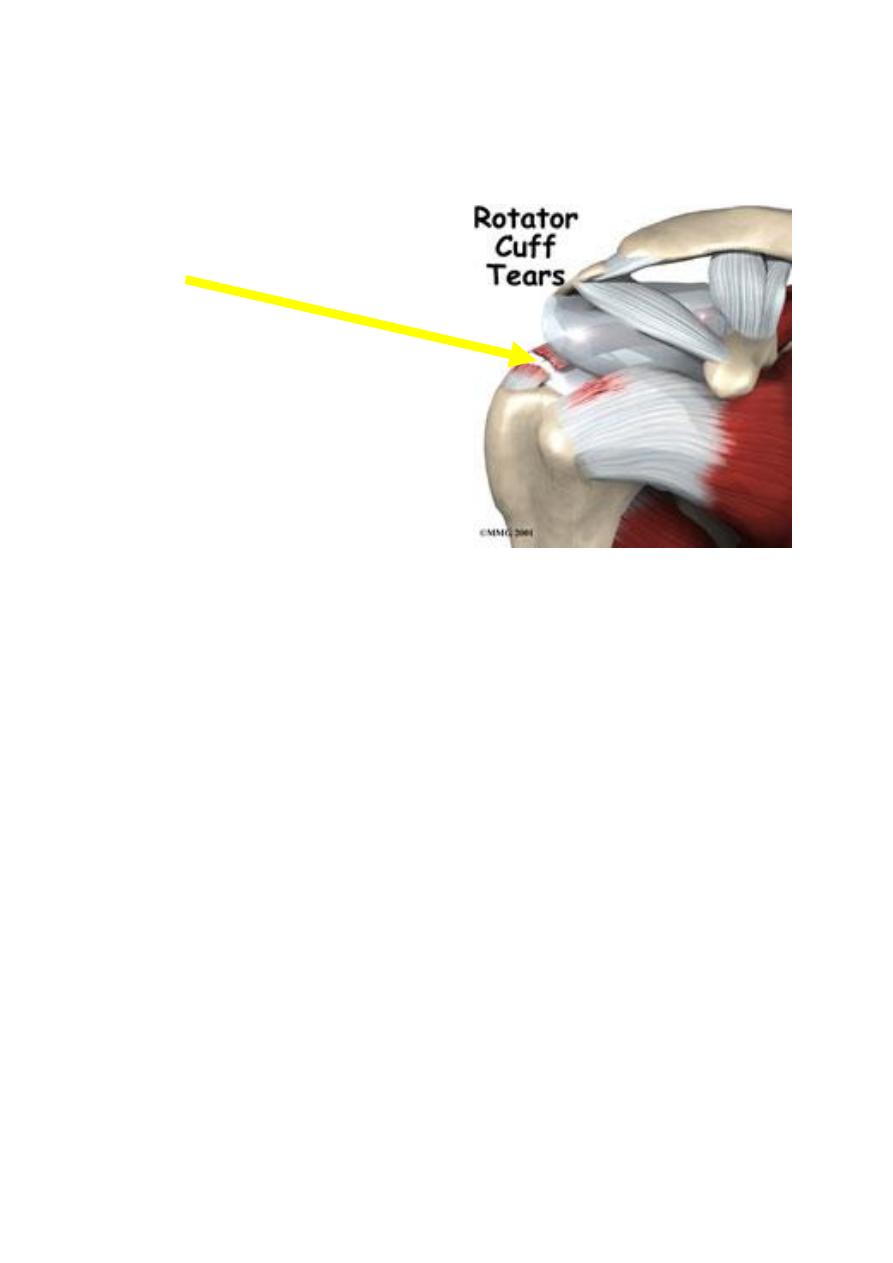
Rotator Cuff Tear
Minor
In minor tears the Supraspinatus muscle is still able to function
.
16
Major
In a major tear there is no activity of the Supraspinatus muscle.
Clinical features
The patient is usually aged 45-75.
While lifting a weight or protecting himself from falling, he 'sprains' his shoulder.
Pain is felt immediately.
Unable to lift his arm sideways.
The appearance is usually normal.
but in longstanding cases there is Supraspinatus wasting.
Tenderness may be diffuse or may be localized to just below the tip of the acromion
process.
With a recent injury, active abduction is grossly limited and painful.
17
To distinguish between partial and complete tears, pain is abolished by injecting a
local anesthetic.
if active abduction is now possible, the tear must be only partial
.
Weeks later
Two types are easily differentiated.
With a complete tear.
Pain has by then subsided.
Active abduction is impossible
.
Passive abduction is full and once the arm has been lifted above a right angle, the
patient can keep it up by deltoid (the abduction paradox).
When he lowers it sideways it suddenly drops (the drop-arm sign).
With a partial tear.
Abduction slowly recovers
.
18
Investigations
The diagnosis may be confirmed by
Ultrasonography.
M R I
Arthroscopy
A.L.Y