Baghdad College of Medicine / 5
th
grade
Student’s Name :
Dr. Yasser Naif Qassim
Lec. 2
Maxillofacial Trauma
Sun. 9 / 10 / 2016
DONE BY : Ali Kareem
مكتب اشور لالستنساخ
2016 – 2017
Maxillofacial Trauma Dr. Yasser N. Qassim
9-10-2016
2
©Ali Kareem 2016-2017
Maxillofacial Trauma
Dr.YASSIR NAIF QASSIM
F.I.B.M.S
(PLASTIC & RECONSTRUCTIVE)
Facial injuries deserve special attention, because of their life and aesthetic significance.Facial
trauma is a life threathing condition because :
1- The face is an area of airway passage (mouth and nose).
2- The face is very vascular area (carotid arteries, vertebral arteries,…etc).
3- It may be associated with other injuries to brain and spine.
A. SOFT TISSUE INJURIES
Soft tissue injuries may include:
Contusion: is a brusing injury caused by blunt trauma, can be associated with underlying
hematoma.
Abrasion: is loss of superficial layers of skin by contact with rough objects.
Puncture wound: is caused by sharp pointed tool, may be associated with injury of an
underlying deep structures.
Accidental (traumatic) tattoo: in which small particles embeding the dermis .
Clear cut injury.
Laceration injury: the most common form of facial injury characterized byirregular
margins and should be repaired in layers.
Avulsion flap: is an undermined laceration that can be one of the most disfiguring of all
soft tissue injueies.
Special region considerations:
1. Cheek and temporal region: high risk of injury to facial nerve and parotid gland and its
duct.
2. Eyelid injuries: required precise alignment of tarsal plate and lid margin.
3. Lip injuries: the whitroll and vermilion border should be aligned first and the muscle
should be repaired.
4. Eyebrow:should never be shaved and must be repaired with precise attention to its shape
and border. Muscles division under brow should alwaysbe repaired to prevent spreading
and depression scar.
5. Nose: once the bony framework is accurately restored, soft tissues need only to be
approximated According to anatomical arrangement.
Maxillofacial Trauma Dr. Yasser N. Qassim
9-10-2016
3
©Ali Kareem 2016-2017
B. SKELETAL INJURIES
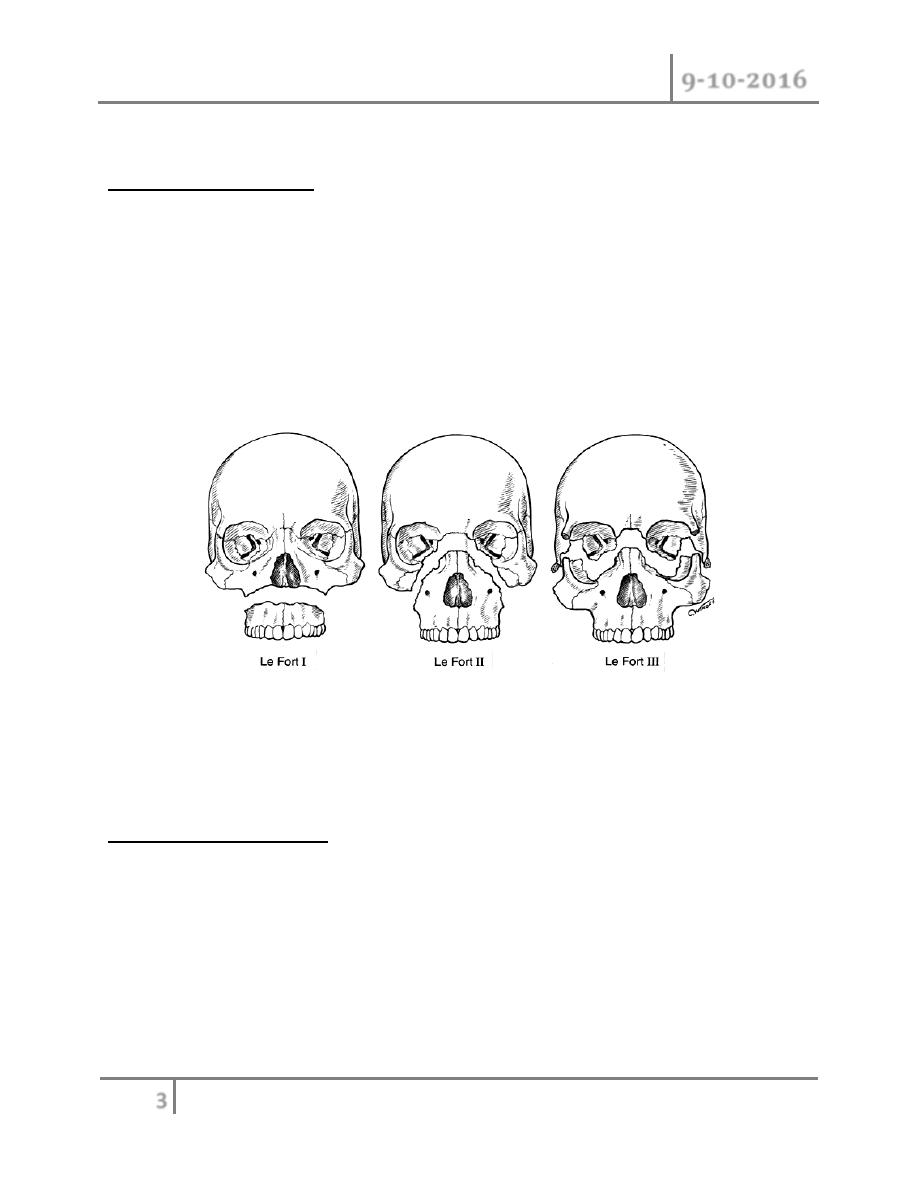
1-Maxillary Fractures:
First described by an anatomist René Le Fort in 1901.
Le Fort I — A transverse fracture involving the maxilla resulting in a floating palate.
Le Fort II — A pyramidal fracture that involve the maxilla & traverses the infraorbital rims and
nasoethmoid region producing midface mobility.
Le Fort III — A fracture through the zygoma, orbital floor and nasal bridge that results in
craniofacial dysjunction.
The Le Fort II fracture is the most common, followed by Le Fort I and III patterns.
The patient is presenting with malocclusion , mobile maxilla , epistaxis and periorbital
ecchymosis(Le Fort II & III) , and battle sign,haemotympanum,&CSF otorrhea(Le Fort III).
2-Mandibular fractures:
Mandibular fracture can be classified according to:
1. Region of mandible: condyle and condylar neck, ramus, coronoid, angle, body,
symphysis.
The neck of condyle is the most common site fallowed by the angle of mandible; the least
common site is the region of canine tooth.
2. Open or closed: depending on whether or not have communication with skin laceration.
3. according to direction: whether oblique, transverse, or comminuted.
Maxillofacial Trauma Dr. Yasser N. Qassim
9-10-2016
4
©Ali Kareem 2016-2017
Usually the patient is presenting with pain, swelling, tenderness and malocclusion. Also
numbness in the distribution of mental nereve,bleeding from laceration or from socket of tooth,
trismus (pain on moving the jaw) is noted.On palpation we can feel crepitus, tenderness and
when the patient is asked to open his or her mouth the jaw deviated toward one side.
3-Zygomatic fractures:
The patient is presenting with malar flattening , Infraorbital nerve parasthesia , tenderness and
brusisng.In case of isolated zygomatic arch fractures there will be limitation of mandibular range
of motion.
4-Bony orbital fractures:
Inferior and medial wall are most frequently involved & usually the patient is presenting with
diplopia due to injury of muscles or nerve, and subconjectival hemorrhage. Enopthalmus due to
pressure from outside or exopthalmus indicating retrorbital hematoma may be the presenting
signs.
5-Nasal bone fractures:
Nasal fractures are either laterally or posteriorly displace.The presenting features include
swelling of the nose & the medial orbital region ,Pain,nasal obstruction.crepitation, nasal
deformity,septum deviation,nasal bleedings (epistaxsis),& mucosal laceration with or without
septal haematoma.
Evaluation and initial management :
1-History: ask about the mechanism of injury and if the patient is unconscious we take the
history from witness which includes the mechanism of injury, history of previous medical or
surgical disease.
2-Clinical examination: the examination should be quick and proper.Begin with overall
inspection noting any facial asymmetries, hemorrhage and ecchymosis.Neurological examination
of 12 cranial nerves and sensory examination.All bony surfaces are palpated to assess areas of
tenderness, crepitation or any bone defect.
3-Investigation: these include general blood examination e.g.Hb,blood group & Rh,bleeding
time & clotting time.The basic biochemical investigations should also be done like blood sugar
and renal function tests in addition to radiological examinations which include:
Maxillofacial Trauma Dr. Yasser N. Qassim
9-10-2016
5
©Ali Kareem 2016-2017
A- Plain film: which have limited role in the radiological evaluation of facial trauma. Include:
o Skull film(lateral and posteroanterior view).
o Panorex radiographs for evaluation of mandible.
o Submentvertex view for zygomatic arch.
o Cerical spine X-ray.
B- maxillofacial computer tomography (CT/SCAN): which is the study of choice for
evaluation of most of facial injuries include axial and coronal planes.
4-Treatment:
1. Maintenance of airway: there are many causes of airway obstruction in facial injuries:
o Bleeding interferes with respiration.
o Displaced facial fractures.
o When there is mandibular fracture, the tongue fall back against the pharynx.
o Fractured or avulsed teeth, vomits, forgien bodies.
o Swelling, edema, hematoma narrowing the airway.
Edema tends to develop within 60-90 mints. Sothe patient initially has good airway but later it
become potentially occluded.
The patient should be placed in prone position, and often be assure that there is no cervical spine
fracture, the neck is extended.The obstruction by foreign bodies and avulse teeth can be cleared
by sweeping fingers deeply into mouth and oropharynx.In some cases intubations may be
needed, & when there is a difficulty in intubations or in patient with significant neck swelling
and fracture of mandible , tracheostomy is indicated.
2. Control hemorrhage: although hemorrhage from facial wound appears alarming, it seldom to
be the sole causes of the shock, except in case of close range shotgun wound.Hemorrhage can be
controlled temporarily by direct pressure.In rare situation of uncontrolled hemorrhage from nose
or nasopharynx angiographic embolization is indicated.
3. Aspiration of blood, saliva or gastric contents frequently accompanies maxillofacial injury. It
is prevented by endotracheal Intubations.
4. Control shock: shock is only occasionally caused by facial injury alone.Extensive facial
injury& penetration ocular injury may cause shock by pain.When patient with facial injury is
found in shock, associated injuries should be suspected.
5. Identification of other injuries: e.g. abdominal ,thoracic injuries, & intracranial injuries.
Cervical spine injuries can be missed, so cautiously move the patient and apply cervical collar.

Maxillofacial Trauma Dr. Yasser N. Qassim
9-10-2016
6
©Ali Kareem 2016-2017
After life threating problems have been resolved,all the devitalized tissues should be
debrided(but be conservatie as much as you can) and the wound is copiously irrigated with
normal saline.Soft tissue injuries are repaired under local or general anesthesia(can be left
without repair for up to 24 hours without compromising final result provided the bleeding has
been controlled and wound is dressed).The fractures are redused to normal position and fixed in
place using wires,or mini plates.
Treatment of nasal fracture:
1. epistaxsis can be arrest by:
o Head up position.
o Cold bandage.
o Pressure on nose externally or internally(nasal packing).
2. Corticosteroids are used to minimize edema and facilitated evaluation of fracture
reduction.
3. Septal hematoma should be drainage surgically because it causes resorption of the
cartilage because of pressure necrosis leading to saddle nose.
4. Management of fracture should be done immediately before a significant edema is
developed or after edema is resolved usually after 5-7 days during this period the patient
should have steroids and antibiotics.
Management of fractures by refracturing the bone and reposition of nasal bone in proper
architecture,internal packs are inserted and nasal cast or splint is used externally to hold the
bone.
Internal packs are removed in day 2-3, while external splint is removed in 10- 12 days.All the
patients should be informed that there is possibility of rhinoplasty after one year.
#END of this Lecture …