1
Fifth stage
Gynecology
Lec-2
Dr.Asmaa
5/10/2015
Genital tract malformation
The student at the end of this lecture should be able to :
• Describe the types of uterine anomalies and theirclinical presentations.
• Exclude cryptomenorrhoea from a primary amenorrhoea case with normal secondary
sexual characteristics and cyclical abdominal pain.
Anomalies of the paramesonephric duct
• anomalies of the fallopian tubes, uterus, cervix and vagina are not uncommon.
• The exact aetiology is unknown ,the mostly accepted three theories are:
teratogenesis , genetic inheritance and multifactorial expression.
• DES exposure can cause T shaped narrow endometrial cavity,and fallopian tube
anomalies without affecting the urinary tract,
• Variation and combination of anomalies occur :
lack of development(agenesis),
incomplete development (hypoplasia),
incomplete canalization (atresia)
complete separate development.
Uterine anomalies
Absence of the uterus :
uterus is absent or rudimentary and incapable of function, due
to complete mullerian agenesis
There are two conditions present with absent uterus .

2
1. Mayer Rokitansky Kuster Hauser syndrome (MRKH):
-absent uterus and vagina.
-46XX.
-normal ovarian function.
-presents as primary amenorrhoea .
It can be associated with important anomalies of the urinary system ,as hoarse shoe kidney
or pelvic kidney
2. A state of androgen insensitivity syndrome
- absent uterus
- blind end of the lower vagina
- XY
- absent axillary and pubic hair
- gonads are testis(histology) found in the abdomen or the groin require removal
because of long term malignancy.
No treatment is available for such uterine anomalies (uterine transplantation)
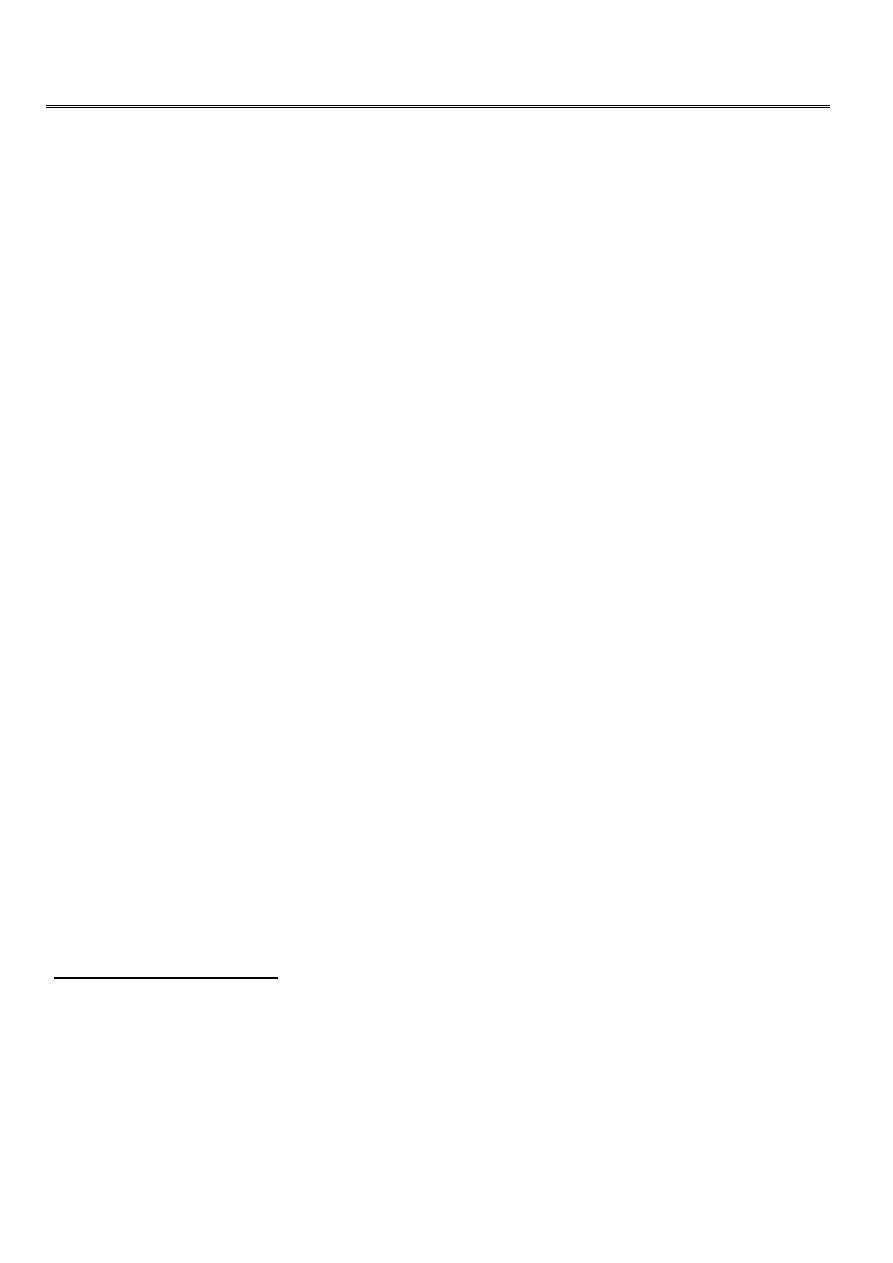
Uterine fusion anomalies:
these are not uncommon and the lesser degrees of defect are quite common.
a.Uterus didelphys : complete lack of fusion of the mullerian ducts with double uterus and
double vagina.
b.Uterus bicornis bicollis : the two horn of the uterus have separate cavities with fused
muscular wall with or without vaginal septum.Lack of complete fusion
c.Uterus bicornis unicollis: the uterine body is bifid and the horns are unequal in size with
normal cervix.
d.Uterus unicornis :when one mullerian canal develops into fallopian tube, uterus and
cervix while the second duct is in rudimentary horn which its canal may not be connected
with the uterus causing hemihaematometra with dysmenorrhoea.its due to failure of
formation.
e.Uterus septus: when the ducts fused and the cavity is separated by a median septum
either partial or complete. There may be vaginal sep. this is due to lack of complete
dissolution of midline paramesonephric system.
3
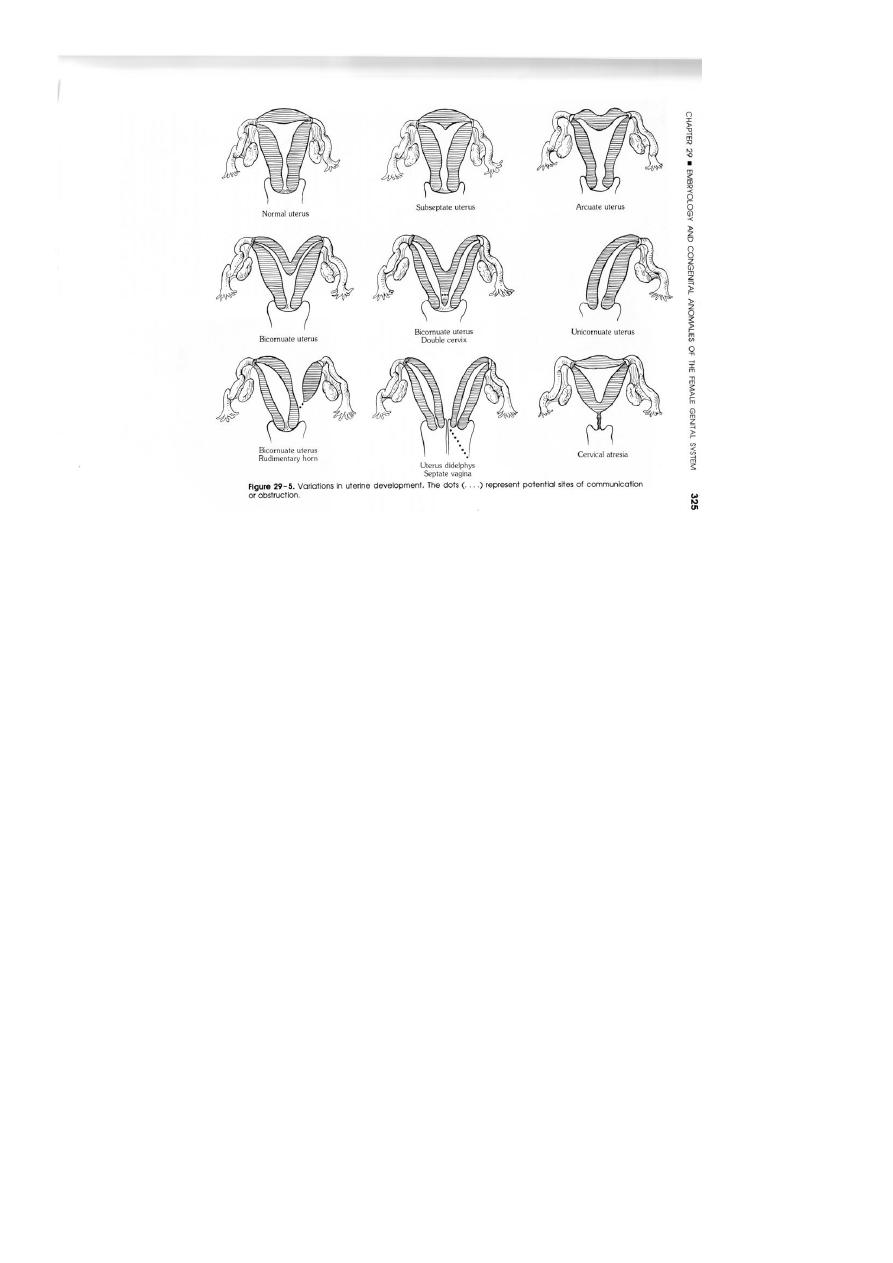
Presentation of uterine anomalies
-symptomless discovered during HSG or during operation.
-infertility.
-dysmenorrhoea(rudimentary horn)
-dyspareunia.
-recurrent pregnancy loss and preterm labour.
-malpresentation
-difficult labour.
- Trapped blood in rudimentary horn or closed vagina.
-rare presentation is ectopic pregnancy in a rudimentary horn .
-Rare uterine arteriovenous malformation result into life threatening haemorrhage
.
4
Vaginal anomalies :(absent,atresia,septum)
absent vagina :
less common type, usually occur with absent uterus in MRKH syndrome (
rarely occur with the presence of the uterus), there is normal secondary sexual characteristics
presents between the age of twelve and sixten years as primary amenorrhoea which suggest
an anatomical abnormality.
Vulval and abdominal examination
ultrasound required to exclude any retained blood inside the upper part of the genital tract,
karyotype is required to exclude androgen insensitivity syndrome (XY ).
5
If the patient abnormality discovered after marriage at attempt of intercoarse operation to
create a new vagina (william operation: edge of the posterior parts of the labia majora are
sutured in the midline result into a perineal puoch) is often satisfactory.
More extensive operation is MacIndoe operation (aspace is dissected between therectum and
the bladder and urethra and this cavity is lined with a skin graft from the thigh applied on
amold which is held to the introitus by stitches. )
If there is a functioning uterus early operation is required and the upper end of the vaginal
epithelium is dissected down to the introitus. Always urinary tract abnormalities should be
excluded.
Canalization defects of vagina
:the more common anomalies of the vagina inluding :
imperforated hymen.
longitudinal and transverse vaginal septum.
partial development(Vaginal atresia).
double vagina.
Imperforforated hymen:
represent the milder form of these canalization defect ,it
occurs at the site where the vaginal plate contacts the urogenital sinus,usually at the
vestibule,similar anomaly ,the transverse vaginal septum,is usualy present at the junction
of the upper and middle third of vagina, Both are associated with normal development of
the upper reproductive tract
Atransverse vaginal septum at sometimes will have asinus tract or perforation that allows
menstruation to escape. less commonly,vaginal atresia represents a more substanial lack
of canalizationof considerable length of the vagina at the caudal or cranial end of the
vaginal plate,if cranially placed there may be associated with absent cervix and upper
vagina. as the uterus is often normal ,the menstrual blood after puberty will be retained
inside, a condition known as cryptomenorrhoea.
The vagina become distended with blood (haematocolpos) the blood become thick and
chocklate after slow absorption of fluid .
Leaking of the fluid into the peritoneal cavity may cause obstruction of the fimbiria or
endometriosis.
The presentation is a female between 14-16 years .
primary amenorrhoea ,
cyclical discomfort then abdominal pain ,
6
mass may be large and felt above the pubic symphysis ,
retention of urine may occur even peritonitis.
Vulval inspection : a bulging membrane may be seen and appear purple or red (thin or
thick).
Rectal examination reveal a mass at the vagina. Hydrocolpos is similar but its distention of
the vagina by the retained mucoid secretion of the cervix present in the neonatal period.
Diagnosis needs US, laproscopy or even laparotomy. Diagnosis is often obvious ,but
difficult in case of obstruction at higher level or in obstruction in one of double system
(normal menses at the patent side).
Treatment : satisfactory drainage best is by excision of the membrane.
There is high risk of infection need antibiotic cover 24 hr. before and 5 days after,
meticulous surgery ,don’t use cotton swab for mopping only suction .
Prognosis is good if the distention only involve the vagina not the uterus nor the tubes.
There is risk of obstruction of the fimbria, endometriosis and infertility.There may be
vaginal stenosis and dyspareunia later on .
Vaginal septum:
there is longitudinal anteroposterior septum due to mullerian fusion anomalies.One of
them may be larger or both have equal size. May obstruct labour when it can be divided
easily if not give away .
Fallopian tubes anomalies
-malformed or absent tube congenital diverticula or accessory ostia have no linical
significance
Gonadal anomalies (gonadal dysgenesis)
Cervical anomalies :
congenital elongation of he cervix to reach the introitus causing discomfort and may require
excision . Malfusion in form of didelphys cervix,or septate cervix.

7
Cyst of the broad ligament:
• Reminant of the wolffian duct
-hydatid of morgagni (pedinculated at the outer end)
-koblet’s tubules (pronephric in origin)
-epoophoron and the paraphoron (proximal) ,both are of mesodermal origin .
Reminant of ovary (fimbrial cyst)