SUBCUTANEOUS MYCOSES
By
Dr. Mohammed H. Mushrif
Lecturer of Medical Mycology

Chromoblastomycosis
Causative fungus
Chromoblastomycosis is caused by five fungi which
are:
1- Phialophora verrucosa
2- Cladophialophora carrionii
3- Rhinocladiella aquaspersa
4- Fonsecaea pedrosoi
5- Fonsecaea compacta
All of these fungi reside in soil and vegetation.
All of these fungi are transmitted by traumatic
inoculation.
All of these fungi are dematiaceous fungi.
Dematiaceous fungi are fungi which have
melanin in their cell walls.
All of these fungi in tissues appear the same
producing spherical copper colored cells (4 – 12
µm in diameter) called sclerotic bodies that
divide by transverse septation producing clusters
of four to eight cells.
These fungi are differentiated only according to
the mode of conidiation.
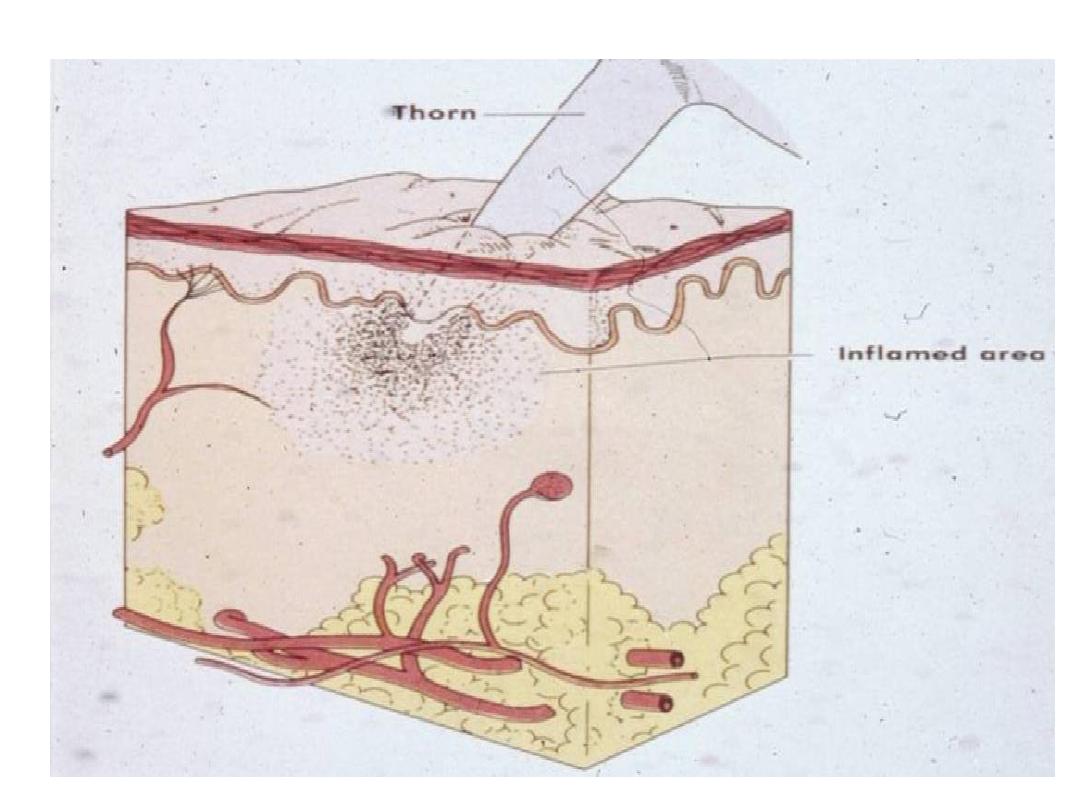
Pathogenesis and clinical picture
Fungi are introduced in the skin by traumatic
inoculation of the exposed areas such as legs or feet.
Infection is slow and will induce hyperplasia of the
epidermal tissues.
Over months to years, the lesion becomes verrucous
with extension along the draining lymphatics.
Then, cauliflower nodules with crusting abscesses
finally cover the lesion.
Dissemination is rare.
Fibrosis of lymphatic channels may occur leading to
lymphatic obstruction and elephantiasis.
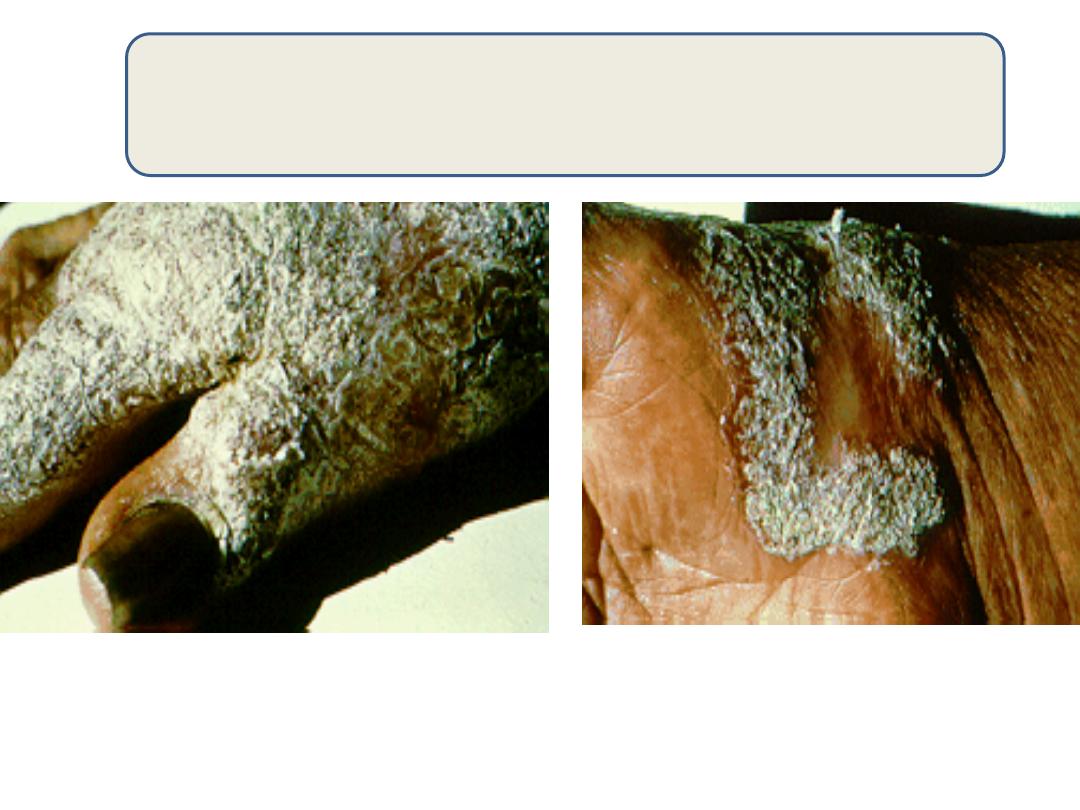
Chronic verrucous chromoblastomycosis
Laboratory diagnosis
Specimen:
scrapings or biopsies from the lesion.
Direct microscopic examination:
Skin scrapings should be examined using KOH 10% and
Parker ink or calcofluor white stains.
Detection of is diagnostic of
chromoblastomycosis regardless of the fungus.
Tissue biopsies should be stained by H&E / PAS / Grocott’s
methenamine silver stains.
Tissue sections reveal AND
sclerotic bodies
granuloma
extensive hyperplasia of the dermal tissue
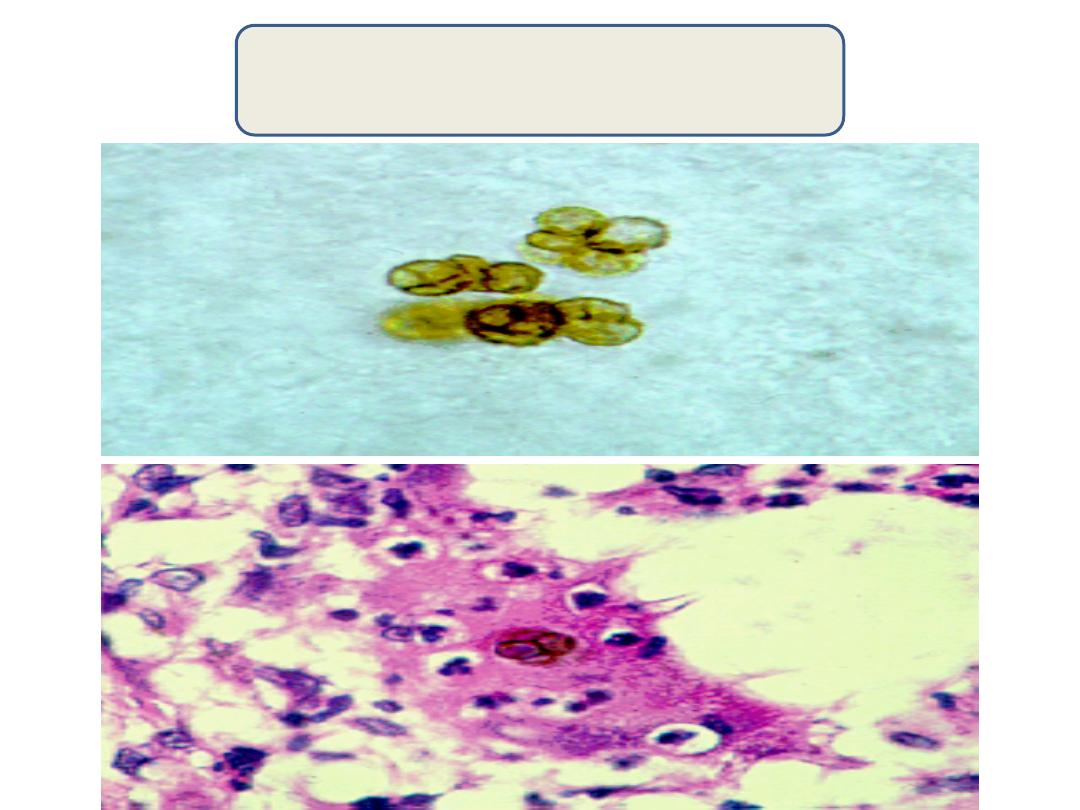
Sclerotic bodies
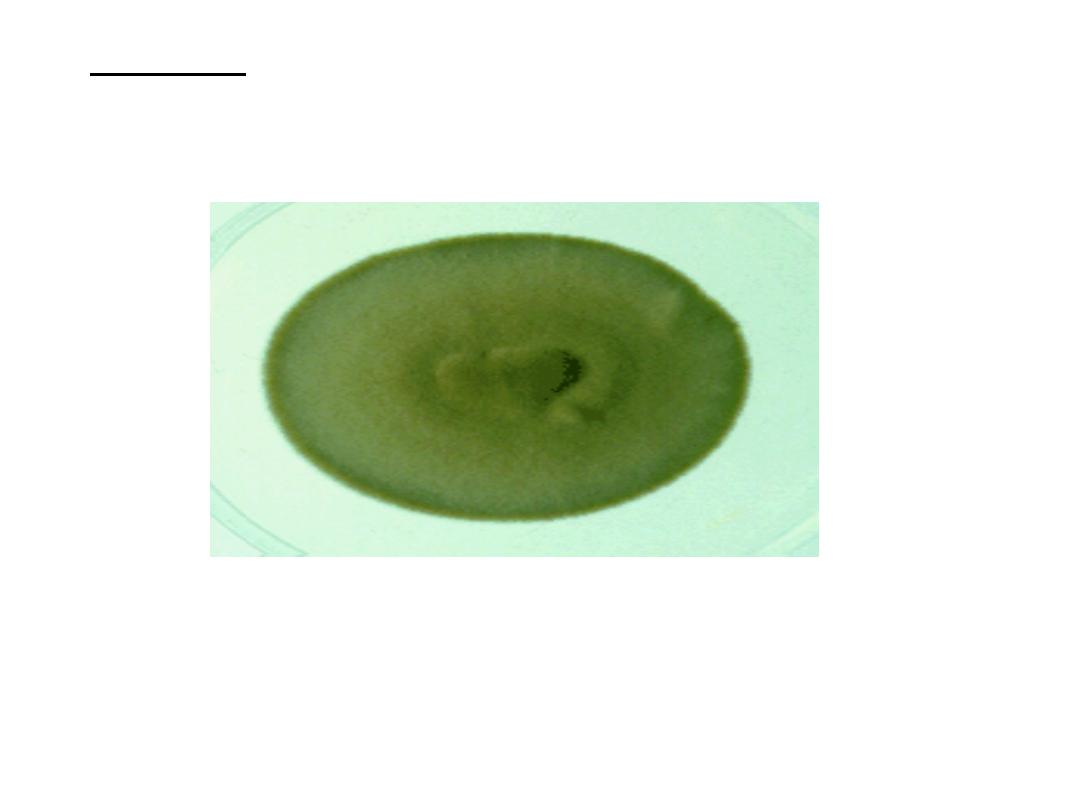
Culture:
Culture is done on SDA with antibiotics at 25 degree
(colonies are olivaceous black with a suede-like surface).
Slide culture is done to identify the fungus based on the
morphology of conidia.

Treatment
• Surgical excision with wide margin is the
therapy for small lesions .
• For larger lesions, we use flucytosine or
itraconazole.
• Relapse is common
Phaehyphomycosis
Phaehyphomycosis is a term applied to
infections characterized by the presence of darkly
pigmented septate hyphae in tissues
(dematiaceous fungi).
Phaehyphomycosis is caused by over 100 species
of dematiaceous fungi.
The clinical forms vary from phaehyphomycotic
cyst in the subcutaneous tissues to sinusitis and
brain abscesses.