
406
CHAPTER 9
supplies the medial third of the dorsum of the hand
tendon, descends over the extensor retinaculum, and
winds around the ulna deep to the flexor carpi ulnaris
posterior cutaneous branch of the ulnar nerve
The
finger.
the ulnar nerve, also supplies the lateral side of the ring
variation. Frequently, a dorsal digital nerve, a branch of
hand and fingers supplied by the radial nerve is subject to
side of the ring finger. The area of skin on the back of the
the thumb, the index and middle fingers, and the lateral
It divides into several dorsal digital nerves that supply
lateral two thirds of the dorsum of the hand (Fig. 9.38).
descends over the extensor retinaculum, and supplies the
around the radius deep to the brachioradialis tendon,
winds
superficial branch of the radial nerve
The
The Upper Limb
(Fig. 9.38). It divides into several dorsal digital nerves
cal muscle on the lateral side (Fig. 9.63).
side and farther distally receives the tendon of the lumbri
insertion of the corresponding interosseous muscle on each
The dorsal extensor expansion receives the tendon of
(Fig. 9.63).
verge to be inserted into the base of the distal phalanx
which con
two lateral parts,
the middle phalanx, and
which is inserted into the base of
central part,
parts: a
phalangeal joint, the extensor expansion splits into three
(Figs. 9.56 and 9.57). Near the proximal inter
expansion
extensor
tendon joins the fascial expansion called the
On the posterior surface of each finger, the extensor
digiti minimi (Fig. 9.55).
joined on its medial side by the two tendons of the extensor
of the extensor indicis, and the tendon to the little finger is
to the index finger is joined on its medial side by the tendon
proximal to the heads of the metacarpal bones. The tendon
connect the tendons to the little, ring, and middle fingers,
of the dorsum of the hand. Strong oblique fibrous bands
which occupies the whole width
subfascial space,
roof of a
embedded in the deep fascia, and together they form the
sum of the hand (Figs. 9.56 and 9.57). The tendons are
under the extensor retinaculum and fan out over the dor
The four tendons of the extensor digitorum emerge from
Insertion of the Long Extensor Tendons
seous spaces.
cates with the deep veins of the palm through the interos
arch, which receives digital veins and freely communi
part of the blood from the whole hand drains into the
medial side, into the basilic vein (Fig. 9.100). The greater
on the lateral side into the cephalic vein and, on the
proximal to the metacarpophalangeal joints and drains
The dorsal venous arch lies in the subcutaneous tissue
Dorsal Venous Arch (or Network)
supply from palmar digital nerves.
remainder of the dorsum of each finger receives its nerve
nerves do not extend far beyond the proximal phalanx. The
The dorsal digital branches of the radial and ulnar
the little fingers.
that supply the medial side of the ring and the sides of
-
-
-
-
-
-
Mallet Finger
flexed when the extensor tendon is taut. The last 20° of active
Avulsion of the insertion of one of the extensor tendons into
the distal phalanges can occur if the distal phalanx is forcibly
extension is lost, resulting in a condition known as mallet
finger
extension of the distal interphalangeal joint. This injury can
to its insertion into the base of the middle phalanx results in
(Fig. 9.71).
Boutonnière Deformity
Avulsion of the central slip of the extensor tendon proximal
a characteristic deformity (Fig. 9.71C). The deformity results
from flexing of the proximal interphalangeal joint and hyper-
result from direct end-on trauma to the finger, direct trauma
over the back of the proximal interphalangeal joint, or lacera-
tion of the dorsum of the finger.
C L I N I C A L N O T E S
The Radial Artery on the Dorsum
ligament of the joint (Fig. 9.65). On reaching the dorsum
longus and extensor pollicis brevis, and lies on the lateral
wrist joint, beneath the tendons of the abductor pollicis
The radial artery winds around the lateral margin of the
of the Hand
of the hand, the artery descends beneath the
n of
tendo
the extensor pollicis longus to reach the
al between
interv
the
two heads of the first dorsal interosseous
re,
muscle; he
the margins of the olecranon fossa of the humerus and
, it is attached above to
Posteriorly
head of the radius.
ulna and to the anular ligament, which surrounds the
and below to the margin of the coronoid process of the
sae and to the front of the medial and lateral epicondyles
along the upper margins of the coronoid and radial fos
, it is attached above to the humerus
Capsule: Anteriorly
Synovial hinge joint
Type:
surfaces are covered with hyaline cartilage.
ulna and the head of the radius (Fig. 9.72). The articular
capitulum of the humerus and the trochlear notch of the
This occurs between the trochlea and
Articulation:
and the shoulder joint are fully described on pages 362
The sternoclavicular joint, the acromioclavicular joint,
(Fig. 9.65).
Dorsal digital arteries pass to the thumb and index finger
take part in the anastomosis around the wrist joint.
Branches of the radial artery on the dorsum of the
(see page 403).
the artery turns forward to enter the palm of the hand
hand
Joints of the Upper Limb
and 364.
Elbow Joint
■
■
■
■
■
■
-
Basic Anatomy
407
A
extensor expansion
extensor digitorum
lumbrical
interosseous
B
C
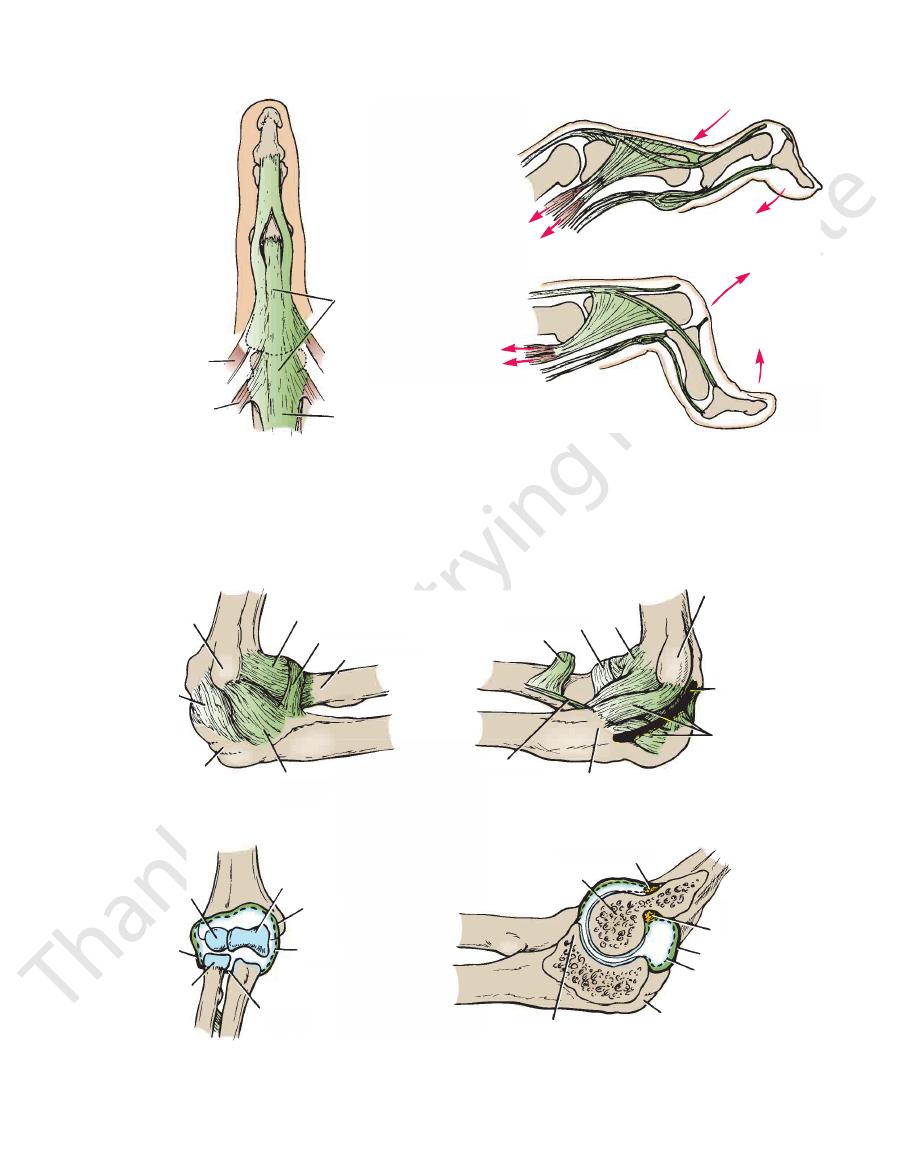
FIGURE 9.71
A.
indicate the direction of the pull of the muscles and the deformity.
Boutonnière deformity. The insertion of the extensor expansion into the base of the middle phalanx is ruptured. The arrows
expansion into the base of the distal phalanx ruptured; sometimes, a flake of bone on the base of the phalanx is pulled off.
Mallet or baseball finger. The insertion of the extensor
which converge to be inserted into the base of the distal phalanx.
geal joint splits into three parts: a central part, which is inserted into the base of the middle phalanx, and two lateral parts,
Posterior view of normal dorsal extensor expansion. The extensor expansion near the proximal interphalan-
B.
C.
lateral
epicondyle
capsule
olecranon
process
lateral collateral
ligament
neck of radius
annular ligament
capsule
annular ligament
biceps
oblique cord
coronoid
process
medial
collateral
ligament
ulnar nerve
medial epicondyle
capitulum
annular
ligament
head of
radius
quadrate
ligament
fat in coronoid fossa
trochlea
olecranon
process
synovial
membrane
capsule
fat in
olecranon
fossa
A
B
C
D
capsule
synovial
membrane
capsule
trochlea
coronoid
process
e
ecranon
ocess
lateral collateral
ligament
neck of radius
annular ligament
capsule
annular ligament
biceps
oblique cord
coronoid
process
me
col
liga
ul
media
um
of
s
quadrate
ligament
fat in coronoid fossa
trochlea
olecranon
process
synovi
memb
capsule
fat
ole
fos
B
capsule
synovial
membrane
caps
trochlea
coronoid
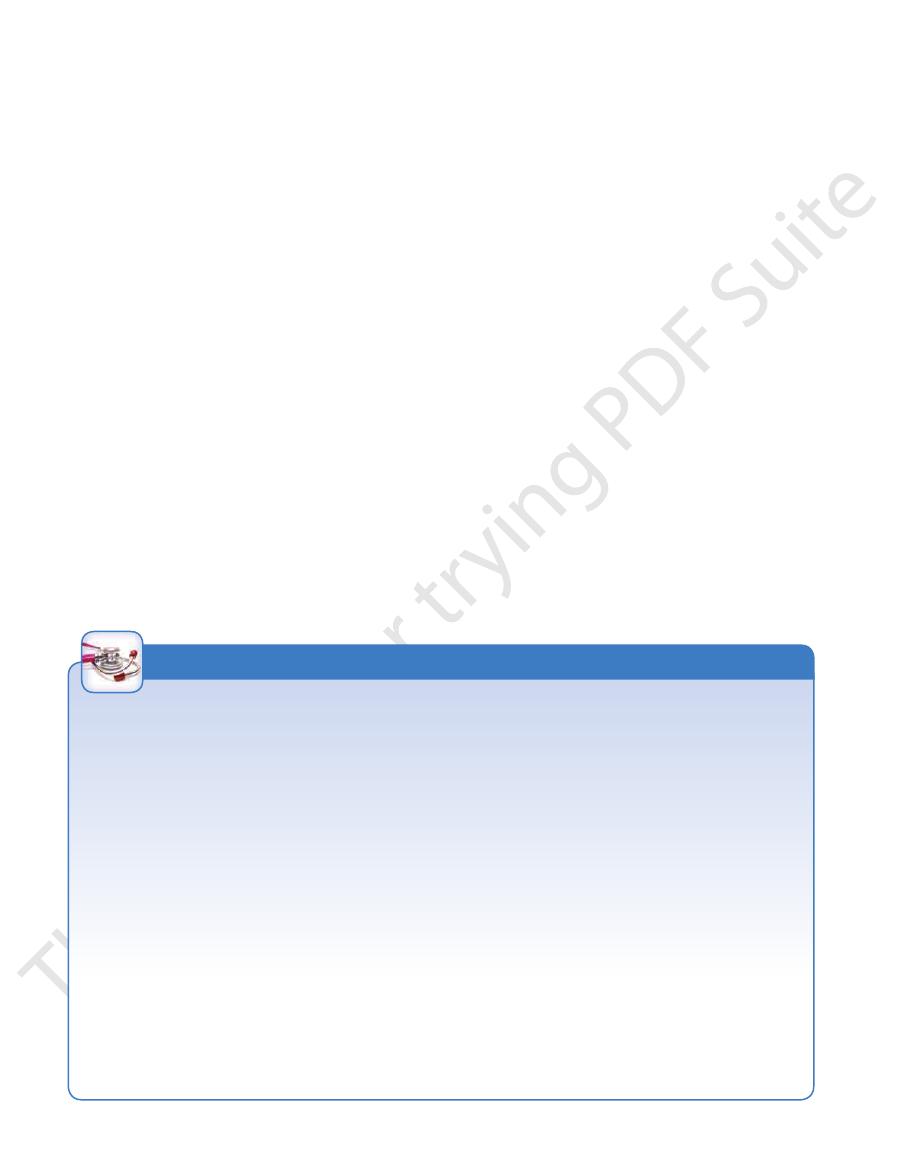
FIGURE 9.72
Right elbow joint.
Sagittal section.
Anterior view of the interior of the joint.
Medial view.
Lateral view.
A.
B.
C.
D.
408
CHAPTER 9
The triceps muscle, a small bursa
Posteriorly:
median nerve, and the brachial artery
The brachialis, the tendon of the biceps, the
Anteriorly:
Important Relations
angle disappears when the elbow joint is fully flexed.
and is about 170° in the male and 167° in the female. The
carrying angle
angle, which opens laterally, is called the
forearm lies at an angle to the long axis of the arm. This
It should be noted that the long axis of the extended
triceps and anconeus muscles.
and pronator teres muscles. Extension is performed by the
performed by the brachialis, biceps brachii, brachioradialis,
the anterior ligament and the brachialis muscle. Flexion is
is checked by the tension of
Extension
coming into contact.
is limited by the anterior surfaces of the forearm and arm
Flexion
The elbow joint is capable of flexion and extension.
Movements
locutaneous, and radial nerves
Branches from the median, ulnar, muscu
Nerve supply:
membrane of the proximal radioulnar joint.
ranon fossae; it is continuous below with the synovial
fatty pads in the floors of the coronoid, radial, and olec
This lines the capsule and covers
Synovial membrane:
ulnar attachments of the two preceding bands.
non; and the transverse band, which passes between the
condyle of the humerus to the medial side of the olecra
the posterior band, which passes from the medial epi
humerus to the medial margin of the coronoid process;
band, which passes from the medial epicondyle of the
consists principally of three strong bands: the anterior
is also triangular and
medial ligament
lar ligament. The
humerus and by its base to the upper margin of the anu
and is attached by its apex to the lateral epicondyle of the
(Fig. 9.72) is triangular
lateral ligament
The
Ligaments:
process of the ulna and to the anular ligament.
below to the upper margin and sides of the olecranon
The Upper Limb
■
■
-
-
-
■
■
-
■
■
-
■
■
■
■
intervening
of the elbow joint. Below it is attached to the inferior
This is continuous above with that
Synovial membrane:
elbow joint. It is not attached to the radius.
(Fig. 9.73). It is continuous above with the capsule of the
ulna and forms a collar around the head of the radius
rior and posterior margins of the radial notch on the
is attached to the ante
anular ligament
The
Ligament:
ous with that of the elbow joint.
The capsule encloses the joint and is continu
Capsule:
Synovial pivot joint
Type:
on the ulna (Figs. 9.72 and 9.73)
the radius and the anular ligament and the radial notch
Between the circumference of the head of
Articulation:
supinator.
The common extensor tendon and the
Laterally:
joint.
epicondyle and crosses the medial ligament of the
ulnar nerve passes behind the medial
The
Medially:
■
■
■
■
Proximal Radioulnar Joint
■
■
■
■
■
■
-
■
■
-
■
■
Stability of Elbow Joint
tomic position, is directed medially and posteriorly and faces in
the physician should see that the medial epicondyle, in the ana
condyle is also common in childhood because then the medial
because the parts of the bones that stabilize the joint are incom
Posterior dislocation usually follows falling on the outstretched
Elbow dislocations are common, and most are posterior.
lar surface of the olecranon and the pulley-shaped trochlea of
The elbow joint is stable because of the wrench-shaped articu-
the humerus; it also has strong medial and lateral ligaments.
When examining the elbow joint, the physician must remember
the normal relations of the bony points. In extension, the medial
and lateral epicondyles and the top of the olecranon process are
in a straight line; in flexion, the bony points form the boundaries
of an equilateral triangle.
Dislocations of the Elbow Joint
hand. Posterior dislocations of the joint are common in children
-
pletely developed. Avulsion of the epiphysis of the medial epi-
ligament is much stronger than the bond of union between the
epiphysis and the diaphysis.
Arthrocentesis of the Elbow Joint
The anterior and posterior walls of the capsule are weak, and
when the joint is distended with fluid, the posterior aspect of the
joint becomes swollen. Aspiration of joint fluid can easily be per-
formed through the back of the joint on either side of the olecra-
non process.
Damage to the Ulnar Nerve with Elbow Joint Injuries
The close relationship of the ulnar nerve to the medial side of
the joint often results in its becoming damaged in dislocations
of the joint or in fracture dislocations in this region. The nerve
lesion can occur at the time of injury or weeks, months, or years
later. The nerve can be involved in scar tissue formation or can
become stretched owing to lateral deviation of the forearm in a
badly reduced supracondylar fracture of the humerus. During
movements of the elbow joint, the continued friction between
the medial epicondyle and the stretched ulnar nerve eventually
results in ulnar palsy.
Radiology of the Elbow Region after Injury
In examining lateral radiographs of the elbow region, it is impor-
tant to remember that the lower end of the humerus is normally
angulated forward 45° on the shaft; when examining a patient,
-
the same direction as the head of the humerus.
C L I N I C A L N O T E S

Basic Anatomy
to the anatomic position and the palm faces anteriorly.
supination is a reversal of this process so that the hand returns
riorly and the thumb lies on the medial side. The movement of
medially in such a manner that the palm comes to face poste
The movement of pronation results in the hand rotating
supination and pronation.
movement of the hand during the repetitive movements of
ment such as a screwdriver because it prevents side-to-side
movement of the ulna is important when using an instru
with the upper limb and is not displaced medially. This
of the ulna moves laterally so that the hand remains in line
the head of the ulna (Fig. 9.75). In addition, the distal end
notch of the radius moving around the circumference of
of the radius with the hand moves bodily forward, the ulnar
rotates within the anular ligament, whereas the distal end
In the movement of pronation, the head of the radius
the apex of the triangular articular disc below.
through the head of the radius above and the attachment of
the proximal and distal radioulnar joints. The axis passes
arm involve a rotary movement around a vertical axis at
The movements of pronation and supination of the fore
Movements
branch of the radial nerve
Anterior interosseous nerve and the deep
Nerve supply:
the edge of one articular surface to that of the other.
This lines the capsule passing from
Synovial membrane:
from the wrist and strongly unites the radius to the ulna.
9.73 and 9.74). It shuts off the distal radioulnar joint
to the lower border of the ulnar notch of the radius (Figs.
the base of the styloid process of the ulna and by its base
cartilage. It is attached by its apex to the lateral side of
This is triangular and composed of fibro
Articular disc:
strengthen the capsule.
ligaments
posterior
anterior
Weak
Ligaments:
superiorly.
The capsule encloses the joint but is deficient
Capsule:
Synovial pivot joint
Type:
the ulnar notch on the radius (Fig. 9.73)
Between the rounded head of the ulna and
Articulation:
sor tendon
Supinator muscle and the common exten
Posteriorly:
Supinator muscle and the radial nerve
Anteriorly:
Important Relations
Pronation and supination of the forearm (see below)
Movements
locutaneous, and radial nerves
Branches of the median, ulnar, muscu
Nerve supply:
lower margin of the radial notch of the ulna.
margin of the articular surface of the radius and the
409
■
■
-
■
■
■
■
-
Distal Radioulnar Joint
■
■
■
■
■
■
■
■
and
■
■
-
■
■
■
■
-
-
-
radial notch of ulna
lateral collateral ligament
annular ligament
olecranon process of ulna
coronoid process of ulna
interosseous membrane
ulna
synovial membrane
triangular
cartilaginous
ligament
styloid process
medial ligament
pisiform
triquetral
joint cavity
interosseous metacarpal
ligaments
interosseous intercarpal ligaments
trapezoid
trapezium
scaphoid
lateral ligament
styloid process
lunate
palmar ligament
collateral ligaments
radius
FIGURE 9.73
Ligaments of the proximal and distal radioulnar joints, wrist joint, carpal joints, and joints of the fingers.
410
CHAPTER 9
The tendon of extensor digiti minimi
Posteriorly:
The tendons of flexor digitorum profundus
Anteriorly:
Important Relations
of supination in right-handed people.
screw and corkscrews are driven inward by the movement
threads and the spiral of corkscrews are made so that the
Because supination is the more powerful movement, screw
movements because of the strength of the biceps muscle.
supinator. Supination is the more powerful of the two
is performed by the biceps brachii and the
Supination
pronator quadratus.
is performed by the pronator teres and the
Pronation
The Upper Limb
■
■
■
■
proximal phalanx
of ring finger
metacarpal
of little finger
fourth dorsal
interosseous
medial ligament
of wrist joint
styloid process of ulna
head of ulna
triquetral
dorsal extensor expansion
extensor digitorum (cut)
extensor indicis (cut)
third metacarpal
extensor pollicis
longus (cut)
first dorsal
interosseous
trapezoid
capitate
hamate
lateral ligament of
wrist joint
styloid process of radius
scaphoid
lunate
shaft of
radius
shaft of ulna
interosseous
membrane
triangular cartilaginous
ligament of wrist joint
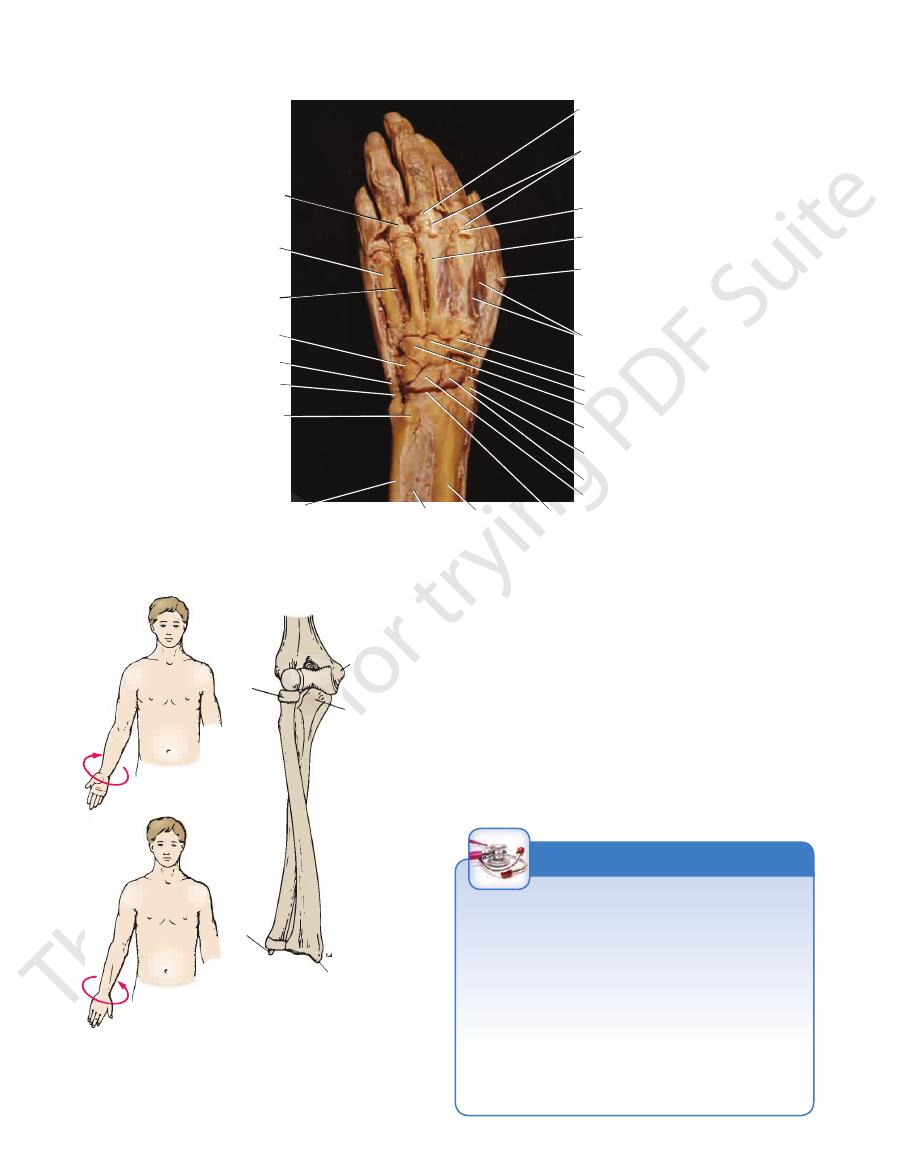
FIGURE 9.74
Dissection of the dorsal surface of the left hand and distal end of the forearm. Note the carpal bones and the
intercarpal joints; note also the wrist (radiocarpal) joint.
A
supination
of forearm
pronation of
forearm
medial
epicondyle
of humerus
coronoid
process
of ulna
styloid
process
of radius
head of
radius
styloid
process
of ulna
B
C
A
supination
of forearm
pronation of
forearm
sty
pro
of r
head of
radius
styloid
process
of ulna
C
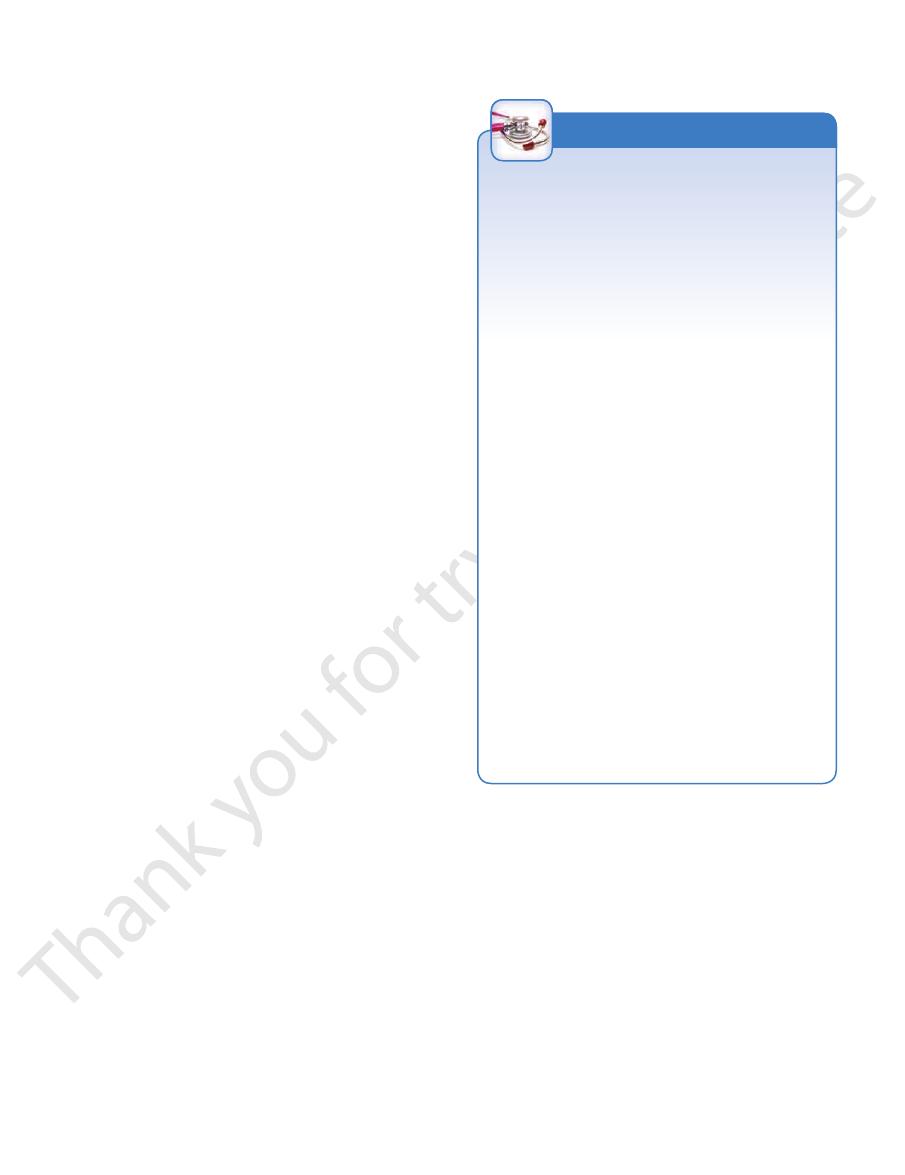
FIGURE 9.75
Movements of supination (
ulna when the forearm is fully pronated.
Relative positions of the radius and the
) of the forearm that take place at the proximal and distal
A) and pronation
(B
radioulnar joints. C.
Radioulnar Joint Disease
infection of the elbow joint invariably involves the proxi
The proximal radioulnar joint communicates with the elbow
joint, whereas the distal radioulnar joint does not communi-
cate with the wrist joint. In practical terms, this means that
-
mal radioulnar joint. The strength of the proximal radioulnar
joint depends on the integrity of the strong anular ligament.
Rupture of this ligament occurs in cases of anterior disloca-
tion of the head of the radius on the capitulum of the humerus.
In young children, in whom the head of the radius is still small
and undeveloped, a sudden jerk on the arm can pull the radial
head down through the anular ligament.
C L I N I C A L N O T E S
Basic Anatomy
Synovial membrane:
interosseous ligaments.
posterior,
anterior,
The bones are united by strong
Ligaments:
The capsule surrounds each joint.
Capsule:
Synovial plane joints
Type:
bones (Figs. 9.73 and 9.74)
joint, between the proximal and distal rows of carpal
the distal row of the carpus; and finally, the midcarpal
imal row of the carpus; between the individual bones of
Between the individual bones of the prox
Articulation:
Intercarpal Joints
The radial artery
Laterally:
nerve
The posterior cutaneous branch of the ulnar
Medially:
abductor pollicis longus
brevis, the extensor pollicis longus and brevis, and the
extensor indicis, the extensor carpi radialis longus and
the extensor digiti minimi, the extensor digitorum, the
The tendons of the extensor carpi ulnaris,
Posteriorly:
median and ulnar nerves
flexor carpi radialis, the flexor carpi ulnaris, and the
fundus and superficialis, the flexor pollicis longus, the
The tendons of the flexor digitorum pro
Anteriorly:
Important Relations
ulnaris.
is performed by the flexor and extensor carpi
Adduction
pollicis longus and brevis.
are assisted by the abductor pollicis longus and extensor
the extensor carpi radialis longus and brevis. These muscles
is performed by the flexor carpi radialis and
Abduction
and the extensor pollicis longus.
digitorum, the extensor indicis, the extensor digiti minimi,
carpi ulnaris. These muscles are assisted by the extensor
longus, the extensor carpi radialis brevis, and the extensor
is performed by the extensor carpi radialis
Extension
digitorum profundus, and the flexor pollicis longus.
are assisted by the flexor digitorum superficialis, the flexor
flexor carpi ulnaris, and the palmaris longus. These muscles
is performed by the flexor carpi radialis, the
Flexion
of pronation and supination of the forearm.
The lack of rotation is compensated for by the movements
possible because the articular surfaces are ellipsoid shaped.
abduction, adduction, and circumduction. Rotation is
The following movements are possible: flexion, extension,
Movements
branch of the radial nerve
Anterior interosseous nerve and the deep
Nerve supply:
pal joints.
radioulnar joint or with the joint cavities of the intercar
joint cavity does not communicate with that of the distal
attached to the margins of the articular surfaces. The
This lines the capsule and is
Synovial membrane:
scaphoid bone (Figs. 9.73 and 9.74).
attached to the styloid process of the radius and to the
lateral ligament
tral bone (Figs. 9.73 and 9.74). The
to the styloid process of the ulna and to the trique
is attached
medial ligament
strengthen the capsule. The
posterior ligaments
Ligaments: Anterior
to the proximal row of carpal bones.
above to the distal ends of the radius and ulna and below
The capsule encloses the joint and is attached
Capsule:
Synovial ellipsoid joint
Type:
surface.
surface, which is adapted to the distal ellipsoid convex
proximal articular surface forms an ellipsoid concave
and triquetral bones below (Figs. 9.73 and 9.74). The
and the articular disc above and the scaphoid, lunate,
Between the distal end of the radius
Articulation:
Wrist Joint (Radiocarpal Joint)
411
■
■
■
■
■
■
■
■
and
-
is
■
■
-
■
■
not
■
■
-
■
■
■
■
■
■
Joints of the Hand and Fingers
■
■
-
■
■
■
■
■
■
and
■
■
joint cavity of the midcarpal joint extends not only
attached to the margins of the articular surfaces. The
This lines the capsule and is
C L I N I C A L N O T E S
Wrist Joint Injuries
tured about 1 in. (2.5 cm) proximal to the wrist joint (Colles’
distal radial epiphysis; in the teenager the clavicle might
for example, there may be a posterior displacement of the
area affected seems to be related to age. In a young child,
ferent parts of the upper limb give way under the strain. The
and finally, to the sternum. If the forces are excessive, dif
scapula to the coracoclavicular ligament and the clavicle;
ulna to the humerus; thence, through the glenoid fossa of the
across the interosseous membrane to the ulna, and from the
the scaphoid to the distal end of the radius, from the radius
In falls on the outstretched hand, forces are transmitted from
tured scaphoid or dislocation of the lunate bone, which are
joint pain, and limitation of movement. These symptoms and
ligament of the wrist joint, producing synovial effusion,
A fall on the outstretched hand can strain the anterior
joint. The joint is stabilized by the strong medial and lateral
which separates the wrist joint from the distal radioulnar
bones by the strong triangular fibrocartilaginous ligament,
bones. The head of the ulna is separated from the carpal
distal end of the radius and the proximal row of carpal
The wrist joint is essentially a synovial joint between the
ligaments.
Because the styloid process of the radius is longer than
that of the ulna, abduction of the wrist joint is less extensive
than adduction. In flexion–extension movements, the hand
can be flexed about 80° but extended to only about 45°. The
range of flexion is increased by movement at the midcarpal
joint.
signs must not be confused with those produced by a frac-
similar.
Falls on the Outstretched Hand
-
fracture; in the young adult the scaphoid is commonly frac-
tured; and in the elderly the distal end of the radius is frac-
fracture) (Fig. 9.50).
C L I N I C A L N O T E S
412
CHAPTER 9
and brevis. The movements of abduction and adduction
is performed by the extensor pollicis longus
extension
is performed by the flexor pollicis longus and brevis and
flexion
of the metacarpophalangeal joint of the thumb,
finger is performed by the palmar interossei. In the case
Movement toward the midline of the third
Adduction:
third finger is performed by the dorsal interossei.
Movement away from the midline of the
Abduction:
extensor digiti minimi
Extensor digitorum, extensor indicis, and
Extension:
the flexor digitorum superficialis and profundus
The lumbricals and the interossei, assisted by
Flexion:
The following movements are possible:
Movements
attached to the margins of the articular surfaces.
This lines the capsule and is
Synovial membrane:
when the joint is in extension.
ligaments are taut when the joint is in flexion and lax
acarpal bone to the base of the phalanx. The collateral
passes downward and forward from the head of the met
bands present on each side of the joints (Fig. 9.73). Each
are cord-like
collateral ligaments
bones together. The
which hold the heads of the metacarpal
pal ligaments,
deep transverse metacar
fifth joints are united by the
The palmar ligaments of the second, third, fourth, and
phalanx but less so to the metacarpal bone (Fig. 9.73).
tain some fibrocartilage. They are firmly attached to the
are strong and con
palmar ligaments
The
Ligaments:
The capsule surrounds the joint.
Capsule:
Synovial condyloid joints
Type:
and the bases of the proximal phalanges (Fig. 9.73)
Between the heads of the metacarpal bones
Articulation:
Metacarpophalangeal Joints
by the opponens pollicis.
The thumb is rotated medially
Rotation (opposition):
Adductor pollicis
Adduction:
Abductor pollicis longus and brevis
Abduction:
Extensor pollicis longus and brevis
Extension:
Flexor pollicis brevis and opponens pollicis
Flexion:
The following movements are possible:
Movements
separate joint cavity.
This lines the capsule and forms a
Synovial membrane:
The capsule surrounds the joint.
Capsule:
Synovial saddle-shaped joint
Type:
shaped base of the first metacarpal bone (Fig. 9.73).
Between the trapezium and the saddle-
Articulation:
Carpometacarpal Joint of the Thumb
(Figs. 9.73 and 9.74).
A small amount of gliding movement is possible
interosseous ligaments. They have a common joint cavity.
synovial plane joints possessing anterior, posterior, and
The carpometacarpal and intermetacarpal joints are
Carpometacarpal and Intermetacarpal Joints
A small amount of gliding movement is possible.
Movements
ulnar nerve
branch of the radial nerve, and deep branch of the
Anterior interosseous nerve, deep
Nerve supply:
and downward between the bones of the distal row.
between the individual bones forming the proximal row
between the two rows of carpal bones but also upward
The Upper Limb
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
■
-
-
-
■
■
■
■
■
■
■
■
■
■
in the anatomic position.
The following movements are described with the hand
index finger are in contact.
with that of the index finger, and the pulp of the thumb and
such a manner that the plane of the thumbnail lies parallel
the others. The metacarpal bone of the thumb is rotated in
partially flexed, the index finger being flexed as much as
(more so than in the position of rest), and the fingers are
semiprone position, the wrist joint is partially extended
thumb and index finger (Fig. 9.76). The forearm is in the
the hand when it is about to grasp an object between the
is the posture adopted by
position of function
The
nail lies at a right angle to the plane of the other fingernails.
flexed as much as the others; and the plane of the thumb
fingers are partially flexed, although the index finger is not
joint is slightly extended; the second, third, fourth, and fifth
9.76). The forearm is in the semiprone position; the wrist
when the fingers are at rest and the hand is relaxed (Fig.
is the posture adopted by the hand
position of rest
The
the movements of the fingers.
fixator action on the wrist joint, ensuring a stable base for
the flexors and extensors of the carpus can exert a balanced
ing to their best mechanical advantage; at the same time,
long flexor and extensor tendons of the fingers are work
ous membrane is lax. With the wrist partially extended, the
taut; in other positions of the forearm bones, the interosse
midprone position, when the interosseous membrane is
esting to note that the forearm bones are most stable in the
position and the wrist joint is partially extended. It is inter
watch repairing, the forearm is placed in the semiprone
such as those used in the holding of small instruments in
For the hand to be able to perform delicate movements,
Position of the Hand
or her own hand.
is strongly advised to closely observe the movements in his
movements of the hand described in this section, the reader
To comprehend fully the important positioning and
as important as all the remaining fingers combined.
of the first metacarpal bone makes the thumb functionally
between the thumb and index finger. The extreme mobility
action of the thumb, which enables one to grasp objects
Much of the importance of the hand depends on the pincer
upper limb is the important prehensile organ—the hand.
the trunk at the shoulder joint. At the distal end of the
The upper limb is a multijointed lever freely movable on
(Fig. 9.73).
structure similar to that of the metacarpophalangeal joints
Interphalangeal joints are synovial hinge joints that have a
Interphalangeal Joints
are performed at the carpometacarpal joint.
The Hand as a Functional Unit
-
-
-
-
Basic Anatomy
pal bone; a small amount of movement takes place at the
place mainly between the trapezium and the 1st metacar
other nails (Figs. 9.76 and 9.78A). The movement takes
thumbnail being kept at right angles to the plane of the
oposterior plane away from the palm, the plane of the
is the movement of the thumb in an anter
Abduction
are the extensor pollicis longus and brevis.
phalangeal joints. The muscles producing the movement
metacarpal bone, at the metacarpophalangeal and inter
movement takes place between the trapezium and the 1st
plane of the other fingernails (Figs. 9.76 and 9.77A). The
maintain the plane of the thumbnail at right angles to the
coronal plane away from the palm in such a manner as to
is the movement of the thumb in a lateral or
Extension
the flexor pollicis longus and brevis and the opponens pollicis.
phalangeal joints. The muscles producing the movement are
1st metacarpal bone, at the metacarpophalangeal and inter
The movement takes place between the trapezium and the
right angles to the plane of the other fingernails (Fig. 9.76).
such a manner as to maintain the plane of the thumbnail at
is the movement of the thumb across the palm in
Flexion
Movements of the Thumb
413
-
-
-
-
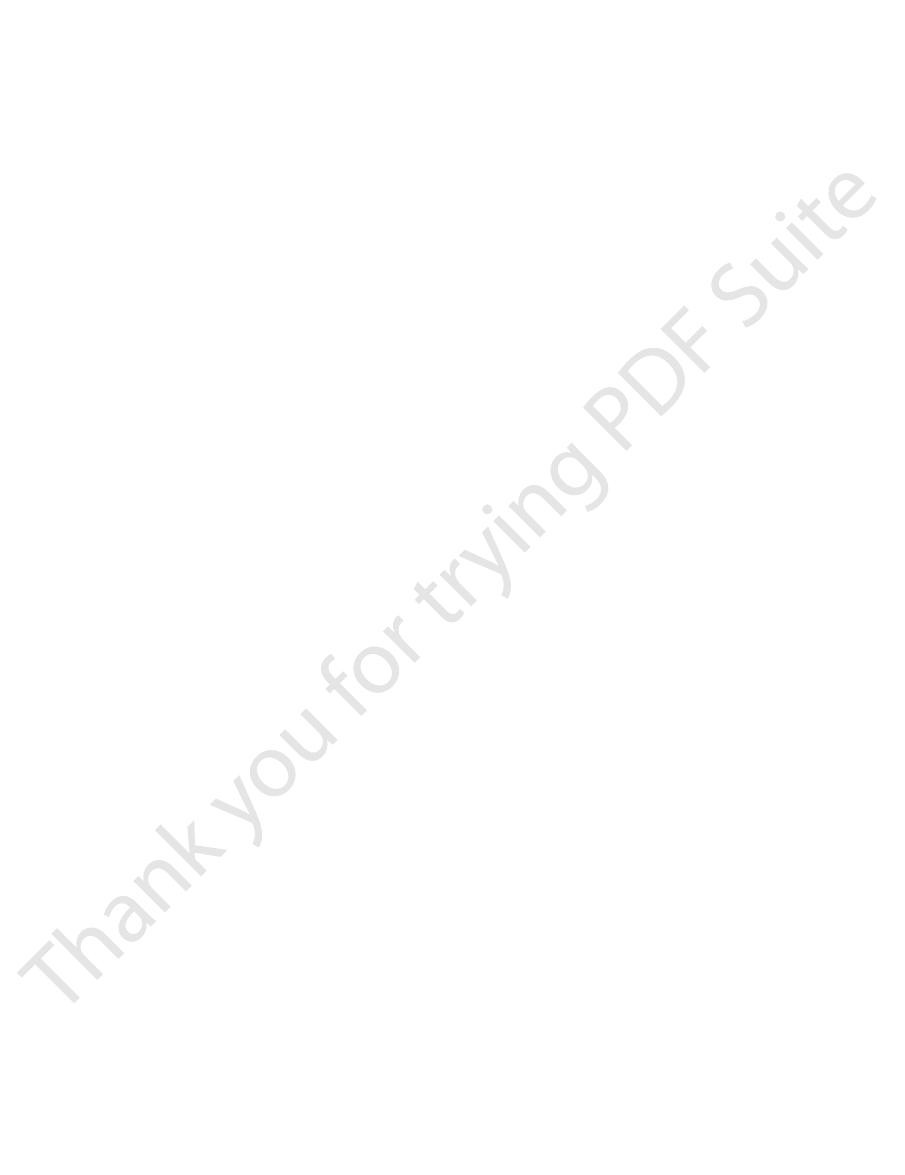
position of rest
position of function
flexion of thumb
abduction of thumb
extension of thumb
adduction of thumb
opposition of thumb
FIGURE 9.76
Various positions of the hand and movements of the thumb.

414
CHAPTER 9
anteroposterior plane. The movement takes place at the
is the movement forward of the finger in an
Flexion
Little Fingers
Movements of the Index, Middle, Ring, and
ducing the movement is the opponens pollicis.
the plane of the nail of the opposed finger. The muscle pro
zium. The plane of the thumbnail comes to lie parallel with
metacarpal bone and the attached phalanges on the trape
ment is accomplished by the medial rotation of the 1st
any of the other fingers (Figs. 9.76 and 9.77C). The move
comes into contact with the anterior surface of the tip of
palm in such a manner that the anterior surface of the tip
is the movement of the thumb across the
Opposition
pollicis.
The muscle producing the movement is the adductor
place between the trapezium and the 1st metacarpal bone.
fingernails (Figs. 9.76 and 9.78B). The movement takes
nail being kept at right angles to the plane of the other
oposterior plane toward the palm, the plane of the thumb
is the movement of the thumb in an anter
Adduction
movement are the abductor pollicis longus and brevis.
metacarpophalangeal joint. The muscles producing the
The Upper Limb
-
-
-
-
-
interphalangeal and metacarpophalangeal joints. The distal
placed in a partially opposed position and is also slightly
a deep concavity. To achieve this, the thumb is abducted and
In the cupped position, the palm of the hand is formed into
the metacarpal head, and the collateral ligaments are slack.
base of the phalanx is in contact with the rounded part of
the extended position of the metacarpophalangeal joint, the
by the collateral ligaments, which are taut in this position. In
the metacarpal bone. The two bones are held in close contact
in contact with the flattened anterior surface of the head of
the articular surface of the base of the proximal phalanx lies
in the extended position. In the flexed position of the finger,
Abduction and adduction of the fingers are possible only
producing the movement are the palmar interossei.
takes place at the metacarpophalangeal joint. The muscles
midline of the middle finger (Fig. 9.77B). The movement
is the movement of the fingers toward the
Adduction
tor digiti minimi abducts the little finger.
ducing the movement are the dorsal interossei; the abduc
place at the metacarpophalangeal joint. The muscles pro
middle finger (Figs. 9.69 and 9.77A). The movement takes
the middle finger) away from the imaginary midline of the
is the movement of the fingers (including
Abduction
digiti minimi for the little finger).
by the extensor indicis for the index finger and the extensor
proximal phalanx by the extensor digitorum (in addition,
middle phalanx by the lumbricals and interossei, and the
phalanx is extended by the lumbricals and interossei, the
interphalangeal and metacarpophalangeal joints. The distal
an anteroposterior plane. The movements take place at the
is the movement backward of the finger in
Extension
the proximal phalanx by the lumbricals and the interossei.
middle phalanx by the flexor digitorum superficialis, and
phalanx is flexed by the flexor digitorum profundus, the
-
-
Cupping the Hand
A
B
C
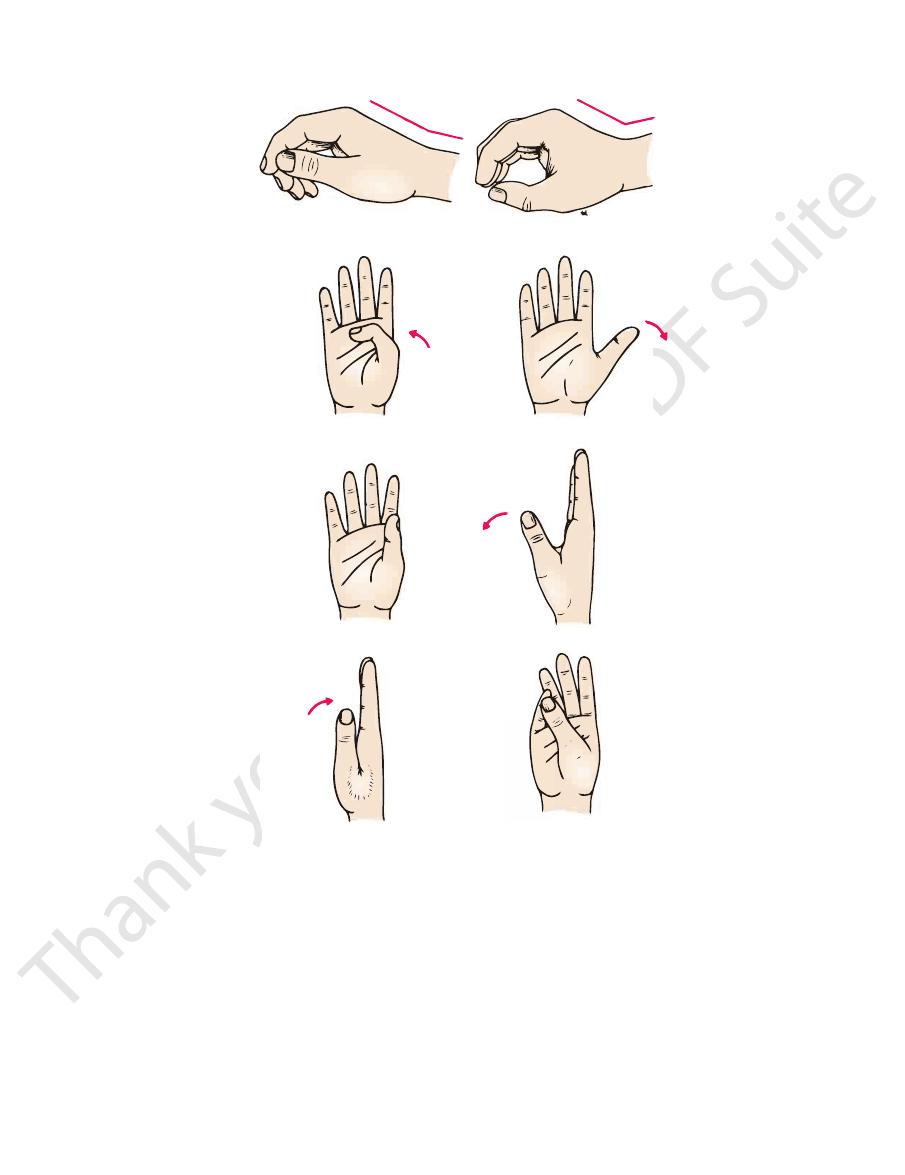
FIGURE 9.77
Left hand with the fingers abducted and the
thumb extended (A), with the fingers adducted and the
thumb adducted (B), and with the thumb in the position of
opposition (C).
A
B
FIGURE 9.78
Left hand with the thumb about to move the
and with the thumb about to move the pencil in the direc
pencil away from the palm to demonstrate abduction (A)
-
tion of the palm to demonstrate adduction (B).
Basic Anatomy
very difficult.)
(Try to make a “strong fist” with the wrist joint flexed—it is
carpi ulnaris muscles must occur to extend the wrist joint.
the extensor carpi radialis longus and brevis and the extensor
ment to be carried out efficiently, a synergic contraction of
long flexor muscles of the fingers and thumb. For this move
fingers and thumb. It is performed by the contraction of the
pophalangeal joints and the interphalangeal joints of the
Making a fist is accomplished by flexing the metacar
joints to increase the general concavity of the cupped hand.
the fingers are also rotated slightly at the metacarpophalangeal
The index, middle, ring, and little fingers are partially flexed;
which improves the gripping ability of the palm.
the hypothenar eminence medially; it also puckers the skin,
palmaris brevis muscle contracts and pulls the skin over
effect of drawing the hypothenar eminence forward. The
slightly rotated at the carpometacarpal joints. This has the
The 4th and 5th metacarpal bones are flexed and
forward.
flexed. This has the effect of drawing the thenar eminence
415
Making a Fist
-
-
Diseases of the Hand and Preservation of Function
ing the thumb) is normally flexed into the palm, it points to the
From the clinical standpoint, the hand is one of the most impor-
tant organs of the body. Without a normally functioning hand, the
patient’s livelihood is often in jeopardy. To students who doubt
this statement, I would suggest that they place their right (or
left) hand in a pocket for 24 hours. They will be astonished at the
number of times they would like to use it if they could.
From the purely mechanical point of view, the hand can be
regarded as a pincer-like mechanism between the thumb and
fingers, situated at the end of a multijointed lever. The most
important part of the hand is the thumb, and it is the physician’s
responsibility to preserve the thumb, or as much of it as possible,
so that the pincer-like mechanism can be maintained. The pin-
cer-like action of the thumb largely depends on its unique ability
to be drawn across the palm and opposed to the other fingers.
This movement alone, although important, is insufficient for the
mechanism to work effectively. The opposing skin surfaces must
have tactile sensation—and this explains why median nerve
palsy is so much more disabling than ulnar nerve palsy.
If the hand requires immobilization for the treatment of dis-
ease of any part of the upper limb, it should be immobilized (if
possible) in the position of function. This means that if loss of
movement occurs at the wrist joint, or at the joints of the hand or
fingers, the patient will at least have a hand that is in a position of
mechanical advantage, and one that can serve a useful purpose.
Physicians should also remember that when a finger (exclud-
tubercle of the scaphoid; individual fingers requiring immobili-
zation in flexion, on a splint or within a cast, should therefore
always be placed in this position.
Always refer to the patient’s fingers by name: thumb, index,
middle, ring, and little finger. Numbering the fingers is confusing
(is the thumb a finger?) and has led to such disastrous results as
amputating the wrong finger.
C L I N I C A L N O T E S
Development of the Upper Limb
may occur. A defective limb may possess a rudimen
that migrate within each limb. As a consequence of these two
terior groups, and the nerve trunks entering the base of each
whereas the mesenchyme of the postaxial border becomes asso
associated and innervated with the lower five cervical nerves,
The mesenchyme situated along the preaxial border becomes
opposite the bases of the limb buds start to grow into the limbs.
limb buds elongate, the anterior rami of the spinal nerves situated
As the
and upper two thoracic segments. The flattened limb buds have
before the leg buds and lie at the level of the lower six cervical
two pairs of flattened paddles (Fig. 9.79). The arm buds develop
This causes the overlying ectoderm to bulge from the trunk as
result of a localized proliferation of somatopleuric mesenchyme.
The limb buds appear during the sixth week of development as the
a cephalic preaxial border and a caudal postaxial border.
-
ciated with the 8th cervical and 1st thoracic nerves.
Later, the mesenchymal masses divide into anterior and pos-
limb also divide into anterior and posterior divisions. The mes-
enchyme within the limbs differentiates into individual muscles
factors, the anterior rami of the spinal nerves become arranged
in complicated plexuses that are found near the base of each
limb so that the brachial plexus is formed.
Amelia
Absence of one or more limbs (amelia) or partial absence (ectro-
melia)
-
tary hand at the extremity of the limb or a well-developed hand
E M B R Y O L O G I C N O T E S
(continued)