Basic Anatomy
335
Skin 380
Fascial Compartments of the
Forearm 382
The Region of the Wrist 394
Structures on the Anterior Aspect of
the Wrist 394
Structures on the Posterior Aspect of
the Wrist 396
The Palm of the Hand 397
Skin 397
Deep Fascia 398
The Palmar Aponeurosis 398
The Carpal Tunnel 398
Fibrous Flexor Sheaths 398
Synovial Flexor Sheaths 399
Insertion of the Long Flexor
Tendons 400
Small Muscles of the Hand 400
Short Muscles of the Thumb 400
Short Muscles of the Little Finger 400
Arteries of the Palm 402
Veins of the Palm 403
Lymph Drainage of the Palm 403
Nerves of the Palm 404
Fascial Spaces of the Palm 404
Pulp Space of the Fingers 405
The Dorsum of the Hand 405
Skin 405
Dorsal Venous Arch (or Network) 406
Insertion of the Long Extensor
Tendons 406
The Radial Artery on the Dorsum of the
Hand 406
Joints of the Upper Limb 406
Elbow Joint 406
Proximal Radioulnar Joint 408
Distal Radioulnar Joint 409
Wrist Joint (Radiocarpal Joint) 410
Joints of the Hand and Fingers 411
The Hand as a Functional Unit 412
Radiographic Anatomy 418
Radiographic Appearances of the Upper
Limb 418
Surface Anatomy 418
Anterior Surface of the Chest 418
Suprasternal Notch 418
Sternal Angle (Angle of Louis) 418
Xiphisternal Joint 418
Costal Margin 418
Clavicle 418
Ribs 419
Deltopectoral Triangle 419
Axillary Folds 419
Axilla 419
Posterior Surface of the Chest 425
Spinous Processes of Cervical and
Thoracic Vertebrae 425
Scapula 425
The Breast 425
The Elbow Region 426
The Wrist and Hand 426
Important Structures Lying in Front of
the Wrist 426
Important Structures Lying on the
Lateral Side of the Wrist 426
Important Structures Lying on the Back
of the Wrist 428
Important Structures Lying in the
Palm 428
Important Structures Lying on the
Dorsum of the Hand 428
C H A P T E R
nant cells along the lymph vessels to the lymph nodes in the
importance because of the frequent development of cancer in
The basic anatomy of the breast is of considerable clinical
index finger and the unique ability of the thumb to be drawn across
much function as possible. The pincer action of the thumb and
deserve particular attention because the goal is to preserve as
are commonly seen by the physician. Wrist and hand injuries
Pain, fractures, dislocations, and nerve injuries of the upper limb
O B J E C T I V E S
■
■
the palm to the other fingers must be preserved at all costs.
■
■
A physician must be familiar with the nerves, bones, joints,
tendons, and blood and lymphatic vessels and their anatomic
relationships.
■
■
the glands and the subsequent dissemination of the malig-
armpit.
■
■
The primary concern of this chapter is to present to the student
the basic anatomy of the upper limb so that as a practicing
medical professional he or she will be able to make an accurate
diagnosis and initiate prompt treatment.
C H A P T E R O U T L I N E
(continued)
natomy
asic
B
a
The upper limb is a multijointed lever that is freely
secrete milk (Fig. 9.1). They are present in both sexes. In
The breasts are specialized accessory glands of the skin that
Location and Description
be overemphasized.
is largely into the armpit. Their clinical importance cannot
ral region and their blood supply and lymphatic drainage
cally part of the upper limb; they are situated in the pecto
The breasts, although strictly speaking, are not anatomi
of the trunk with the arm), arm, elbow, forearm, wrist, and
The upper limb is divided into the shoulder (junction
finger.
one to grasp objects between the thumb and index
on the pincer-like action of the thumb, which enables
the hand. Much of the importance of the hand depends
distal end of the upper limb is the important organ,
movable on the trunk at the shoulder joint. At the
hand.
The Pectoral Region and the Axilla
The Breasts
-
-

336
CHAPTER 9
increase in length and branching in the duct system
In the early months of pregnancy, there is a rapid
Early
Pregnancy
The Upper Limb
(Fig. 9.2). The secretory alveoli develop at the ends of the
axillary tail
the superficial fascia. A small part, called the
the midaxillary line. The greater part of the gland lies in
to 6th rib and from the lateral margin of the sternum to
sition of fat. The base of the breast extends from the 2nd
the increased size of the glands is mainly from the depo
the ovarian hormones (Fig. 9.1). The ducts elongate, but
assume their hemispherical shape under the influence of
At puberty in females, the breasts gradually enlarge and
Puberty
extend beyond the margin of the areola.
tem of ducts embedded in connective tissue that does not
The breast tissue consists of a sys
areola.
skin called the
are small and surrounded by a colored area of
nipples
The
males and immature females, they are similar in structure.
of ovarian estrogens and progesterone.
lous. The atrophy after menopause is caused by the absence
The breasts tend to shrink in size and become more pendu
The amount of adipose tissue may increase or decrease.
of the secretory alveoli disappear, leaving behind the ducts.
After the menopause, the breast atrophies (Fig. 9.2). Most
Postmenopause
color.
areola fades, but the area never lightens to its original
nearly to their original size. The pigmentation of the
thickens. The breasts and the nipples shrink and return
of them disappear. The interlobular connective tissue
milk is absorbed, the secretory alveoli shrink, and most
the breasts return to their inactive state. The remaining
Once the baby has been weaned,
Postweaning
colostrum.
with the fluid secretion called
mostly because of the distention of the secretory alveoli
process slows. The breasts, however, continue to enlarge,
During the second half of pregnancy, the growth
Late
active.
epidermis. The areolar glands enlarge and become more
a result of increased deposits of melanin pigment in the
and the areola becomes darker and more extensive as
nourishment for the developing gland. The nipple enlarges,
of the connective tissue also increases to provide adequate
expanding and budding secretory alveoli. The vascularity
smaller ducts, and the connective tissue becomes filled with
-
-
-
(Fig. 9.1), extends upward and laterally, pierces the deep
from a circular base.
In young women, the breasts tend to protrude forward
Young Women
(Fig. 9.1).
retromammary space
breasts is a space filled by loose connective tissue called the
(Fig. 9.1). Behind the
suspensory ligaments
that serve as
The lobes of the gland are separated by fibrous septa
areolar glands.
tubercles on the areola are produced by the underlying
(Fig. 9.1). Tiny
areola
the nipple is surrounded by the
just before its termination. The base of
ampulla
dilated
separately on the summit of the nipple and possesses a
out from the nipple. The main duct from each lobe opens
which radiate
lobes,
Each breast consists of 15 to 20
and enters the axilla.
fascia at the lower border of the pectoralis major muscle,
lactiferous ducts
ampulla
nipple
areola
tubercles
lobes
fibrous septa
adipose tissue
clavicle
rib
pectoralis minor
pectoralis major
retromammary space
filled with loose
areolar tissue
skin
fibrous septa-
suspensory ligaments
adipose tissue
areola
nipple
ampulla
lactiferous duct
of lobe of
mammary gland
axillary tail
A
B
C
FIGURE 9.1
Mature breast in the female.
The axillary tail, which pierces the deep fascia and extends into the axilla.
Sagittal
Anterior view with skin partially removed to show internal structure.
A.
B.
section. C.
Basic Anatomy
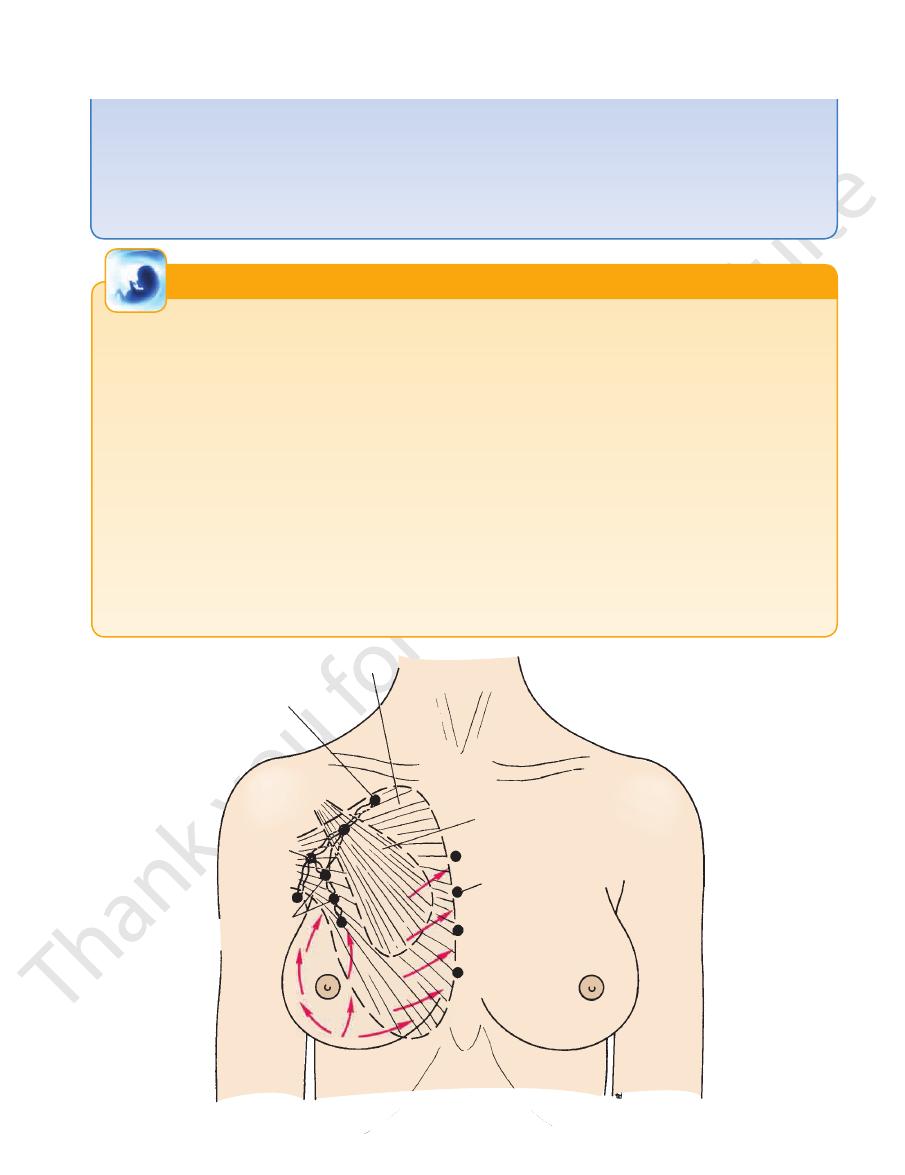
uated along the course of the posterior intercostal arter
drain posteriorly into the posterior intercostal nodes (sit
lymph vessels follow the posterior intercostal arteries and
ity along the course of the internal thoracic artery). A few
thoracic group of nodes (situated within the thoracic cav
that pierce the intercostal spaces and enter the internal
muscle). The medial quadrants drain by means of vessels
just posterior to the lower border of the pectoralis major
rior axillary or pectoral group of nodes (Fig. 9.3) (situated
The lateral quadrants of the breast drain into the ante
nodes.
of the malignant cells along the lymph vessels to the lymph
of cancer in the gland and the subsequent dissemination
clinical importance because of the frequent development
The lymph drainage of the mammary gland is of great
Lymph Drainage
The veins correspond to the arteries.
Veins
lateral thoracic and thoracoacromial branches.
arteries. The axillary artery also supplies the gland via its
branches of the internal thoracic artery and the intercostal
The branches to the breasts include the perforating
Arteries
337
Blood Supply
-
-
-
-
ies); some vessels communicate with the lymph vessels
abdominal wall.
of the opposite breast and with those of the anterior
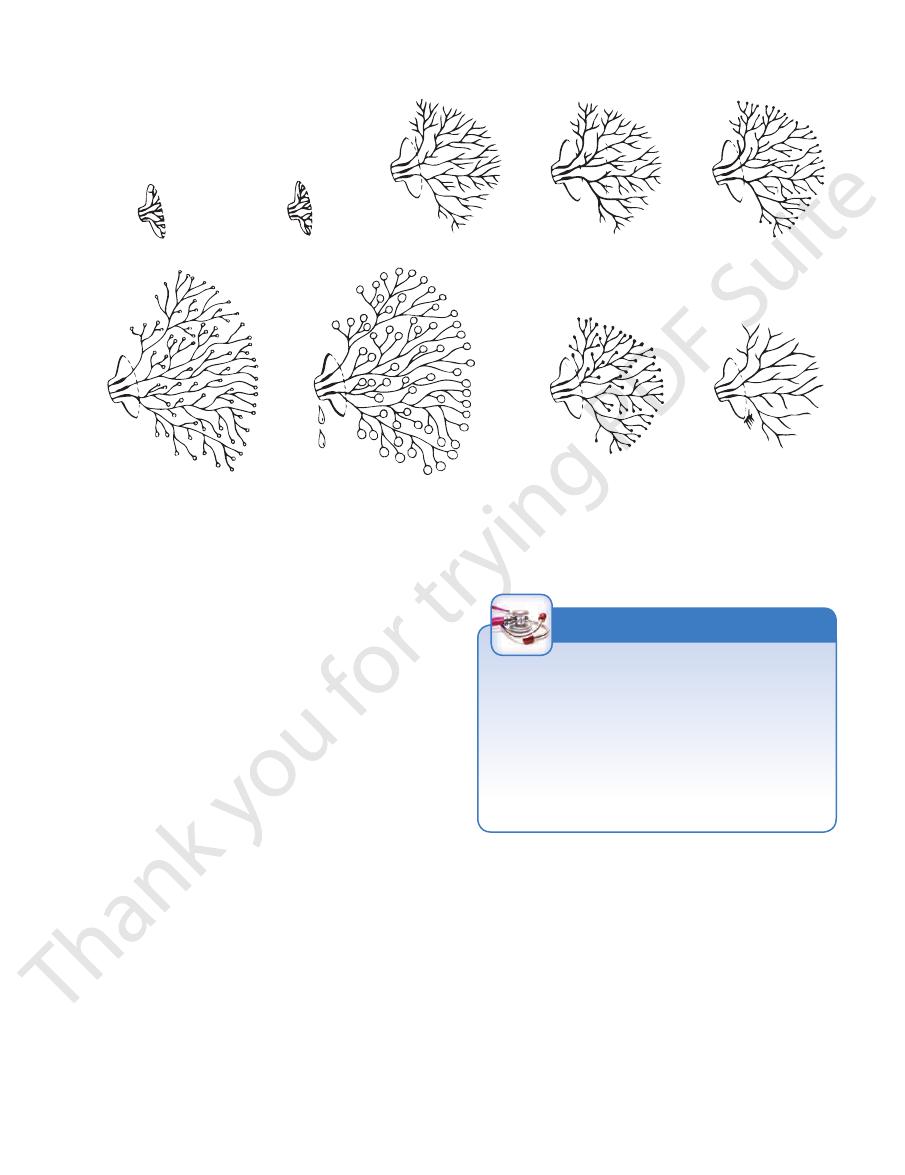
female before puberty
female at puberty
young and adult male
female, first half
of menstrual cycle
female, second half
of menstrual cycle
pregnant female
lactating female
female after cessation
of lactation
female after menopause
FIGURE 9.2
eoli in the breasts in both sexes at different stages of
Extent of the development of the ducts and secretory alv
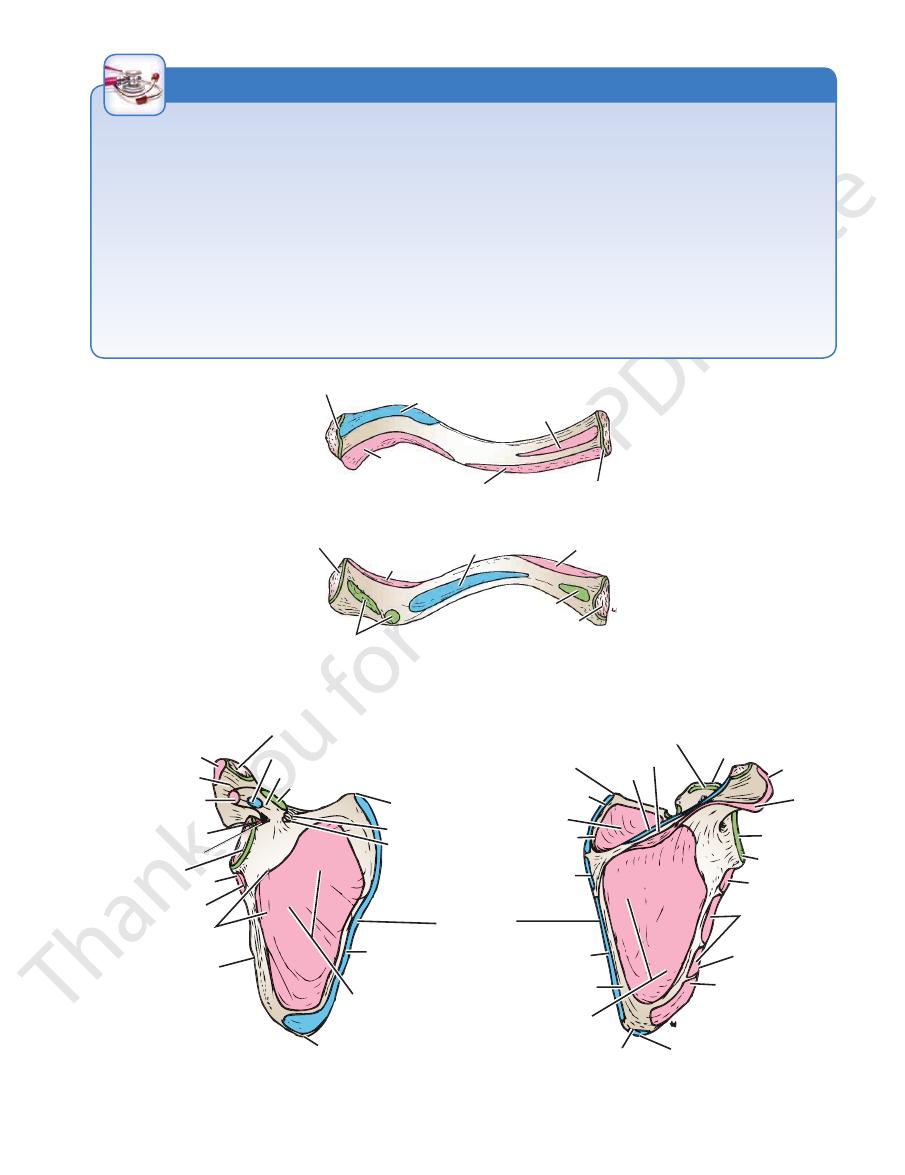
lates with the sternum and 1st costal cartilage medially and
across the root of the neck just beneath the skin. It articu
The clavicle is a long, slender bone that lies horizontally
Clavicle
joint.
which articulate with one another at the acromioclavicular
The shoulder girdle consists of the clavicle and the scapula,
activity.
Bones of the Shoulder Girdle
and Arm
-
with the acromion process of the scapula laterally (Fig. 9.5).
Witch’s Milk in the Newborn
The condition is resolved spontaneously as the maternal hor
may be expressed from the nipples.
witch’s milk,
fluid, called
in both sexes during the first week of life; in some cases a milky
hormones cross the placental barrier and cause proliferation
While the fetus is in the uterus, the maternal and placental
of the duct epithelium and the surrounding connective tissue.
This proliferation may cause swelling of the mammary glands
-
mone levels in the child fall.
C L I N I C A L N O T E S
Basic Anatomy
339
permits pathologic examination of the lymph nodes for possible
tasize into the thorax through the small amount of intervening
in the early stages. However, the prognosis is relatively poor
tumor can usually be felt with the flat of the examining hand
Since the amount of breast tissue in the male is small, the
cinomas of the breast. This fact tends to be overlooked when
metastases.
Carcinoma in the Male Breast
Carcinoma in the male breast accounts for about 1% of all car-
examining the male patient.
in the male, because the carcinoma cells can rapidly metas-
tissue.
Development of the Breasts
Unilateral or bilateral enlargement of the male breast occasionally
is recognized as a circular pigmented area of
month, the
At the fifth
which grow into the underlying mesenchyme. Meanwhile, the
becomes slightly depressed, and sends off 15 to 20 solid cords,
small part in the pectoral region. This localized area thickens,
along this ridge. In the human, the ridge disappears except for a
inguinal region. In animals, several mammary glands are formed
which extends from the axilla obliquely to the
In the young embryo, a linear thickening of ectoderm appears
called the milk ridge,
underlying mesenchyme proliferates, and the depressed ecto-
dermal thickening becomes raised to form the nipple.
areola
skin around the future nipple.
Polythelia
Supernumerary nipples occasionally occur along a line corre-
sponding to the position of the milk ridge. They are liable to be
mistaken for moles.
Retracted Nipple or Inverted Nipple
Retracted nipple is a failure in the development of the nipple
during its later stages. It is important clinically, because normal
suckling of an infant cannot take place, and the nipple is prone to
infection (see also page 338).
Micromastia
An excessively small breast on one side occasionally occurs,
resulting from lack of development.
Macromastia
Diffuse hypertrophy of one or both breasts occasionally occurs
at puberty in otherwise normal girls.
Gynecomastia
occurs, usually at puberty. The cause is unknown, but the condi-
tion is probably related to some form of hormonal imbalance.
E M B R Y O L O G I C N O T E S
pectoralis major
apical lymph nodes
pectoralis minor
central
lymph nodes
internal thoracic
lymph nodes
anterior axillary
or pectoral lymph
nodes
FIGURE 9.3
Lymph drainage of the breast.
340
CHAPTER 9
The Upper Limb
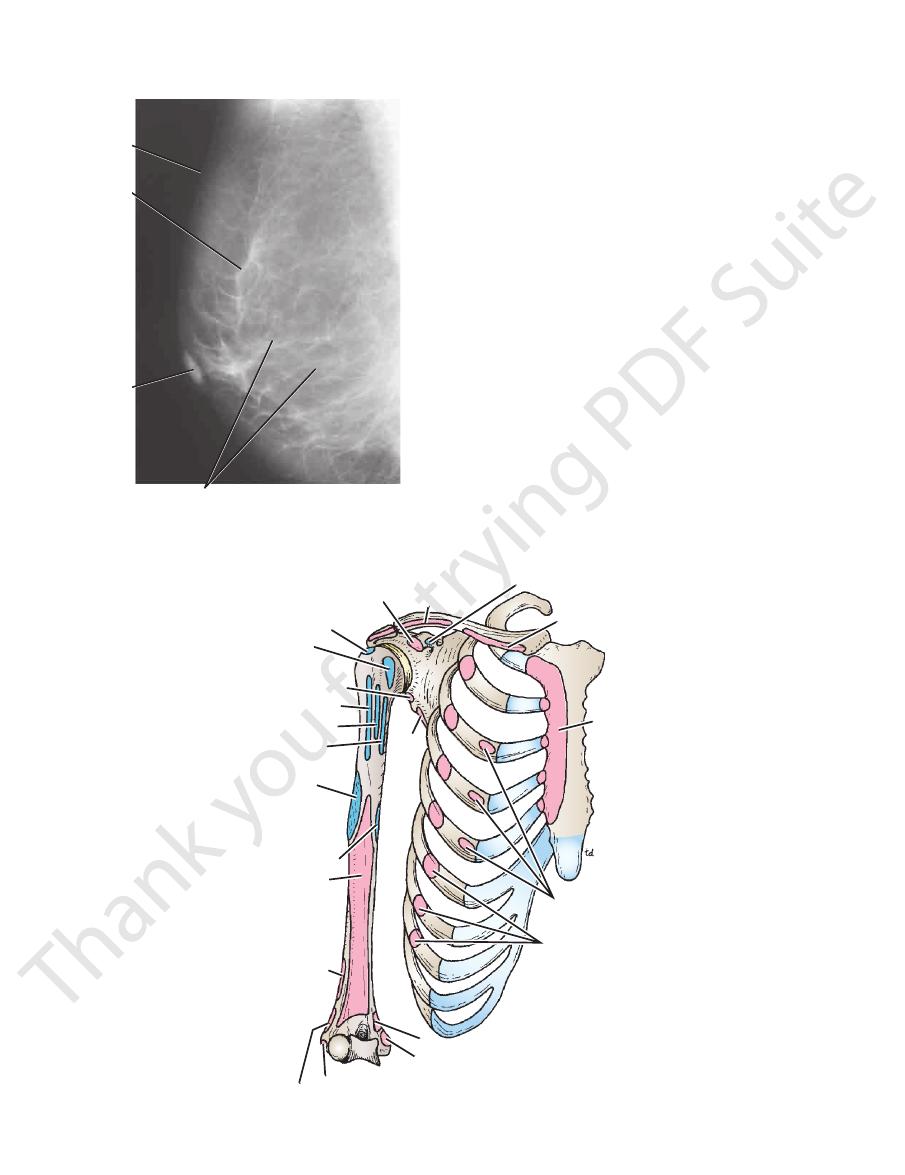
skin
glandular tissue supported
by connective tissue
dense
fibrous
septa
nipple
FIGURE 9.4
Mediolateral mammogram showing the glandu
the 7th thoracic vertebra.
subject and marks the level of the 7th rib and the spine of
of the scapula can be palpated easily in the living
rior angle
infe
below (Fig. 9.5). The
infraspinous fossa
above and an
supraspinous fossa
scapula is divided by the spine into the
The posterior surface of the
subscapular fossa.
the shallow
The anterior surface of the scapula is concave and forms
(Fig. 9.7).
suprascapular notch
coracoid process is the
ment for muscles and ligaments. Medial to the base of the
and forward above the glenoid cavity and provides attach
projects upward
coracoid process
the shoulder joint. The
which articulates with the head of the humerus at
fossa,
or
glenoid cavity,
angle of the scapula forms the pear-shaped
which articulates with the clavicle. The superolateral
mion,
acro
ward. The lateral end of the spine is free and forms the
projects back
spine of the scapula
its posterior surface, the
the posterior chest wall between the 2nd and 7th ribs. On
The scapula is a flat triangular bone (Fig. 9.7) that lies on
in Figure 9.6.
muscles and ligaments attached to the clavicle are shown
and its lateral third is concave forward. The important
The medial two thirds of the clavicle is convex forward
axial skeleton and provides attachment for muscles.
trunk. It also transmits forces from the upper limb to the
The clavicle acts as a strut that holds the arm away from the
lar tissue supported by the connective tissue septa.
-
Scapula
-
-
-
-
coracobrachialis and
short head of biceps
supraspinatus
subscapularis
long head of triceps
pectoralis major
latissimus dorsi
teres major
deltoid
coracobrachialis
brachialis
brachioradialis
extensor carpi radialis longus
common flexor tendon
pronator teres
serratus anterior
pectoralis minor
pectoralis major
pectoralis major
pectoralis minor
deltoid
teres
minor
common extensor tendon
FIGURE 9.5
vicle, scapula, and humerus.
Muscle attachments to the bones of the thorax, cla
Fractures of the Clavicle
fracture of the bone. This may be the cause of persistent pain
pectoralis major. The medial end is tilted upward by the sterno
move freely on the trunk. Unfortunately, because of its position,
The clavicle is a strut that holds the arm laterally so that it can
it is exposed to trauma and transmits forces from the upper limb
to the trunk. It is the most commonly fractured bone in the body.
The fracture usually occurs as a result of a fall on the shoulder
or outstretched hand. The force is transmitted along the clavicle,
which breaks at its weakest point, the junction of the middle and
outer thirds. After the fracture, the lateral fragment is depressed
by the weight of the arm, and it is pulled medially and forward by
the strong adductor muscles of the shoulder joint, especially the
-
cleidomastoid muscle.
The close relationship of the supraclavicular nerves to the
clavicle may result in their involvement in callus formation after
over the side of the neck.
Compression of the Brachial Plexus, Subclavian
Artery, and Subclavian Vein by the Clavicle
The interval between the clavicle and the first rib in some patients
may become narrowed and thus is responsible for compression
of nerves and blood vessels. (See discussion of thoracic outlet
syndrome on page 39.)
C L I N I C A L N O T E S
capsule of sternoclavicular joint
trapezius
deltoid
sternocleidomastoid
pectoralis major
capsule of acromioclavicular joint
superior surface
articular surface for acromium
deltoid
subclavius
pectoralis major
coracoclavicular ligament
costoclavicular
ligament
articular surface for
sternum and first costal cartilage
inferior surface
FIGURE 9.6
Important muscular and ligamentous attachments to the right clavicle.
deltoid
acromion
short head of biceps
and coracobrachialis
supraglenoid
tubercle
long head of biceps
glenoid fossa
lateral border
anterior surface
inferior angle
subscapularis
serratus anterior
suprascapular
notch
suprascapular
ligament
superior angle
coracoclavicular ligament
coracoid process
pectoralis minor
articular surface for clavicle
levator scapulae
supraspinatus
supraspinous
fossa
rhomboid minor
rhomboid major
infraspinous fossa
infraspinatus
latissimus dorsi
inferior angle
teres major
lateral border
teres minor
long head of
triceps
capsule of
shoulder joint
glenoid fossa
acromion
coracoid process
coracoacromial ligament
posterior surface
superior angle
trapezius
spine of scapula
deltoid
medial border
infraglenoid tubercle
subscapular fossa
long head of triceps
FIGURE 9.7
Important muscular and ligamentous attachments to the right scapula.
341
342
CHAPTER 9
scapula are shown in Figure 9.7.
The important muscles and ligaments attached to the
The Upper Limb
Fractures of the Scapula
Fractures of the scapula are usually the result of severe
trauma, such as occurs in run-over accident victims or in
occupants of automobiles involved in crashes. Injuries are
usually associated with fractured ribs. Most fractures of
the scapula require little treatment because the muscles
on the anterior and posterior surfaces adequately splint the
serratus anterior. Such imbalance can be detected by careful
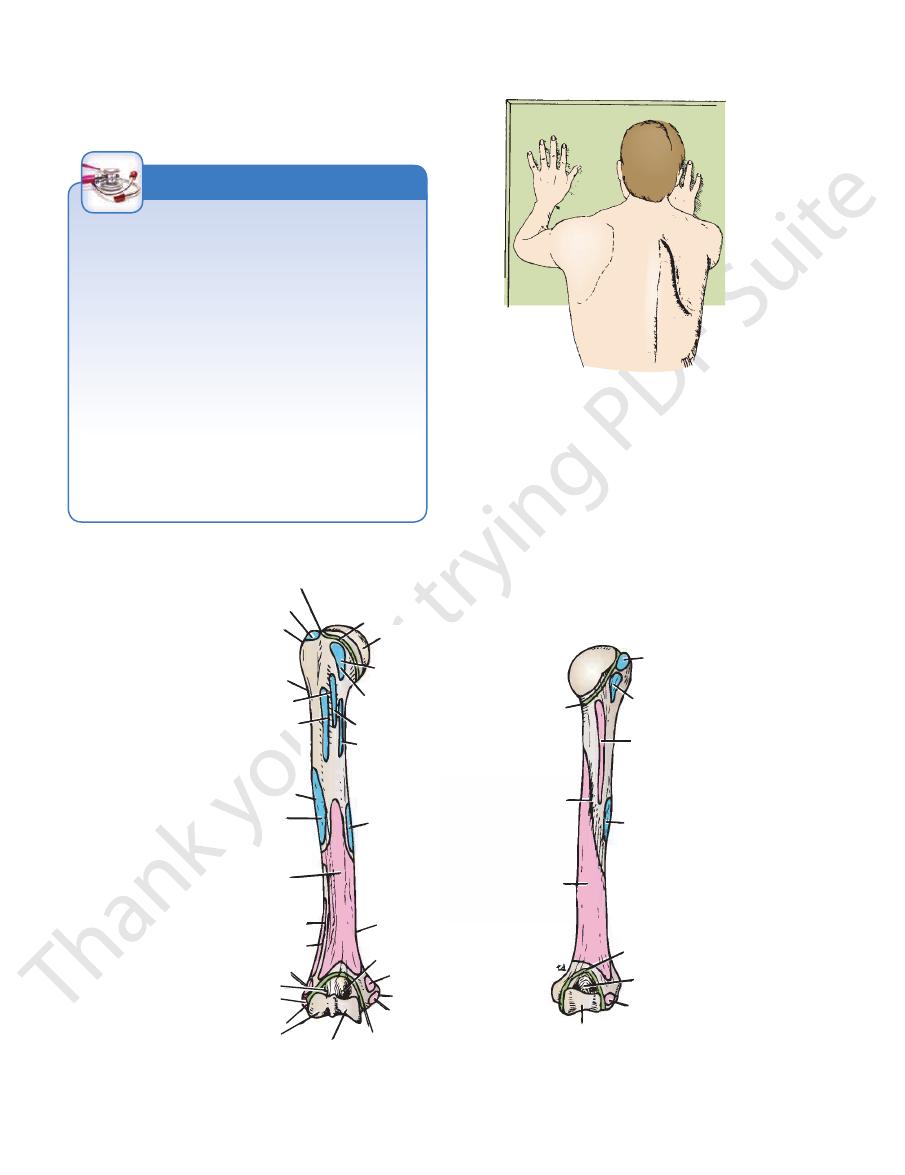
as in dropped shoulder, which occurs with paralysis of the tra
fragments.
Dropped Shoulder and Winged Scapula
The position of the scapula on the posterior wall of the thorax
is maintained by the tone and balance of the muscles attached
to it. If one of these muscles is paralyzed, the balance is upset,
-
pezius, or winged scapula (Fig. 9.8), caused by paralysis of the
physical examination.
C L I N I C A L N O T E S
FIGURE 9.8
Winging of the right scapula.
glenoid cavity of the scapula. Immediately below the head
forms about one third of a sphere and articulates with the
(Fig. 9.9), which
head
upper end of the humerus has a
joint and with the radius and ulna at the elbow joint. The
The humerus articulates with the scapula at the shoulder
Humerus
anatomic neck
supraspinatus
greater tuberosity
surgical neck
bicipital groove
pectoralis major
deltoid tuberosity
deltoid
brachialis
lateral supracondylar ridge
brachioradialis
extensor carpi radialis longus
radial fossa
lateral epicondyle
capitulum
trochlea
capsule of elbow joint
common flexor tendon
medial epicondyle
pronator teres
coronoid fossa
medial
supracondylar ridge
coracobrachialis
teres major
latissimus dorsi
subscapularis
lesser tuberosity
head
capsule of shoulder joint
anterior surface
capsule of
shoulder joint
spiral groove
medial head of triceps
trochlea
anconeus
olecranon fossa
capsule of elbow joint
deltoid
lateral head of triceps
teres minor
infraspinatus
posterior surface
common extensor tendon
FIGURE 9.9
Important muscular and ligamentous attachments to the right humerus.
Basic Anatomy
the upper part of the arm and the side of the chest
The axilla, or armpit, is a pyramid-shaped space between
humerus are shown in Figure 9.9.
The important muscles and ligaments attached to the
elbow joint is extended (Fig. 9.9).
which receives the olecranon process of the ulna when the
olecranon fossa,
ulna. Above the trochlea posteriorly is the
the same movement receives the coronoid process of the
which during
coronoid fossa,
trochlea anteriorly is the
the head of the radius when the elbow is flexed. Above the
which receives
radial fossa,
Above the capitulum is the
articulation with the trochlear notch of the ulna (Fig. 9.9).
for
trochlea
the head of the radius, and the pulley-shaped
for articulation with
capitulum
ligaments, the rounded
for the attachment of muscles and
lateral epicondyles
medial
The lower end of the humerus possesses the
(Fig. 9.9).
which accommodates the radial nerve
spiral groove,
Behind and below the tuberosity
deltoid tuberosity.
lateral aspect of the shaft is a roughened elevation called
About halfway down the
surgical neck.
shaft is a narrow
Where the upper end of the humerus joins the
ital groove.
separated from each other by the
lesser tuberosities,
and
greater
Below the neck are the
anatomic neck.
343
is the
bicip-
the
is a
and
The Axilla
(Fig. 9.11). It forms an important passage for nerves,
pectoralis minor muscles (Figs. 9.12, 9.13, and 9.14)
By the pectoralis major, subclavius, and
Anterior wall:
The walls of the axilla are made up as follows:
Walls of the Axilla
(Fig. 9.11).
the teres major muscle), and medially by the chest wall
lary fold (formed by the tendon of latissimus dorsi and
the pectoralis major muscle), behind by the posterior axil
the anterior axillary fold (formed by the lower border of
is bounded in front by
(Fig. 9.11). The lower end, or
scapula, and medially by the outer border of the first rib
in front by the clavicle, behind by the upper border of the
is directed into the root of the neck and is bounded
apex,
the neck to the upper limb. The upper end of the axilla, or
blood, and lymph vessels as they travel from the root of
base,
-
■
■
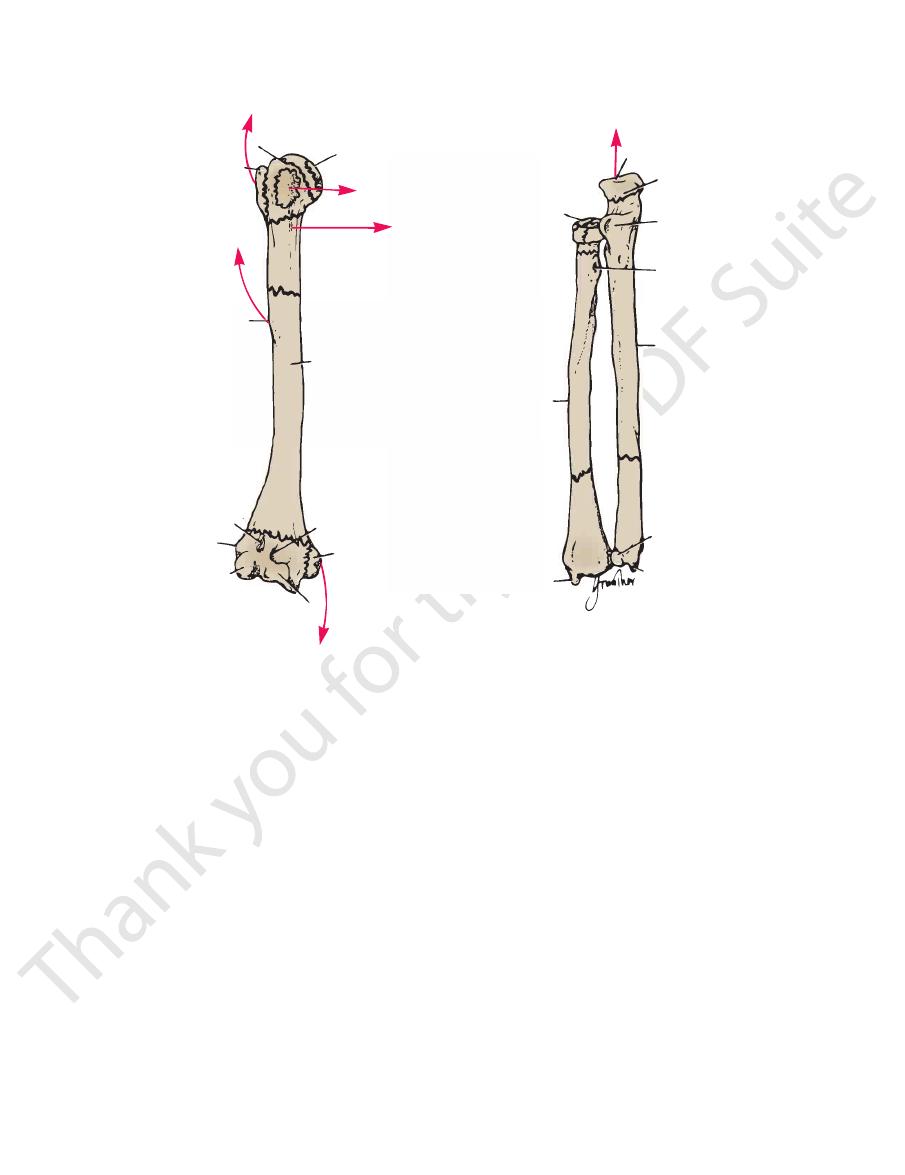
Fractures of the Proximal End of the Humerus
on the irregular bony surface after the bone fragments are
cess of the fracture (in the callus), or can undergo irritation
forcibly abducted. The ulnar nerve can be injured at the time
medial collateral ligament of the elbow joint if the forearm is
The medial epicondyle (Fig. 9.10) can be avulsed by the
on the brachial artery can occur at the time of the fracture or
occur when the child falls on the outstretched hand with the
Supracondylar fractures (Fig. 9.10) are common in children and
the insertion of the deltoid muscle (Fig. 9.10). When the fracture
The surgical neck of the humerus (Fig. 9.10), which lies immedi
shoulder joint has been reduced. In this situation, open reduction of
in the greater tuberosity remaining displaced posteriorly after the
dislocation, severe tearing of the cuff with the fracture can result
dons form part of the rotator cuff. When associated with a shoulder
natus muscle. The bone fragment will have the attachments of the
trauma, displaced by the glenoid labrum during dislocation of the
The greater tuberosity of the humerus can be fractured by direct
Humeral Head Fractures
Fractures of the humeral head (Fig. 9.10) can occur during the
process of anterior and posterior dislocations of the shoulder
joint. The fibrocartilaginous glenoid labrum of the scapula pro-
duces the fracture, and the labrum can become jammed in the
defect, making reduction of the shoulder joint difficult.
Greater Tuberosity Fractures
shoulder joint, or avulsed by violent contractions of the supraspi-
supraspinatus, teres minor, and infraspinatus muscles, whose ten-
the fracture is necessary to attach the rotator cuff back into place.
Lesser Tuberosity Fractures
Occasionally, a lesser tuberosity fracture accompanies poste-
rior dislocation of the shoulder joint. The bone fragment receives
the insertion of the subscapularis tendon (Fig. 9.10), a part of the
rotator cuff.
Surgical Neck Fractures
-
ately distal to the lesser tuberosity, can be fractured by a direct
blow on the lateral aspect of the shoulder or in an indirect man-
ner by falling on the outstretched hand.
Fractures of the Shaft of the Humerus
Fractures of the humeral shaft are common; displacement of
the fragments depends on the relation of the site of fracture to
line is proximal to the deltoid insertion, the proximal fragment
is adducted by the pectoralis major, latissimus dorsi, and teres
major muscles; the distal fragment is pulled proximally by the
deltoid, biceps, and triceps. When the fracture is distal to the
deltoid insertion, the proximal fragment is abducted by the del-
toid, and the distal fragment is pulled proximally by the biceps
and triceps. The radial nerve can be damaged where it lies in
the spiral groove on the posterior surface of the humerus under
cover of the triceps muscle.
Fractures of the Distal End of the Humerus
elbow partially flexed. Injuries to the median, radial, and ulnar
nerves are not uncommon, although function usually quickly
returns after reduction of the fracture. Damage to or pressure
from swelling of the surrounding tissues; the circulation to the
forearm may be interfered with, leading to Volkmann’s ischemic
contracture (see page 383).
of the fracture, can become involved later in the repair pro-
reunited.
C L I N I C A L N O T E S
344
CHAPTER 9
The Upper Limb
anatomic neck
head
surgical neck
PM
shaft of humerus
coronoid
fossa
medial
epicondyle
CF
trochlea
lateral epicondyle
radial fossa
deltoid tuberosity
D
TR
olecranon process
trochlear notch
coronoid process
bicipital tuberosity
shaft of ulna
head
styloid process
styloid process
shaft of radius
A
B
head
S
greater tuberosity
SUB
capitulum
FIGURE 9.10
A.
among these structures in the axilla is an important nerve
the trunk, down as far as the level of the umbilicus. Lying
from the upper limb and the breast and from the skin of
and lymph vessels and lymph nodes, which drain lymph
and its tributaries, which drain blood from the upper limb;
which supply blood to the upper limb; the axillary vein
The axilla contains the axillary artery and its branches,
Contents of the Axilla
armpit.
and joins the fascial floor of the
ligament of the axilla
suspensory
muscle and then continues downward as the
and 9.14). Below, it splits to enclose the pectoralis minor
tissue that is attached above to the clavicle (Figs. 9.13
The clavipectoral fascia is a strong sheet of connective
Clavipectoral Fascia
divide it into three parts (see page 350).
of nerves. It is used when describing the axillary artery to
ula. It crosses the axillary artery and the brachial plexus
inserted by its apex into the coracoid process of the scap
3rd, 4th, and 5th ribs and runs upward and laterally to be
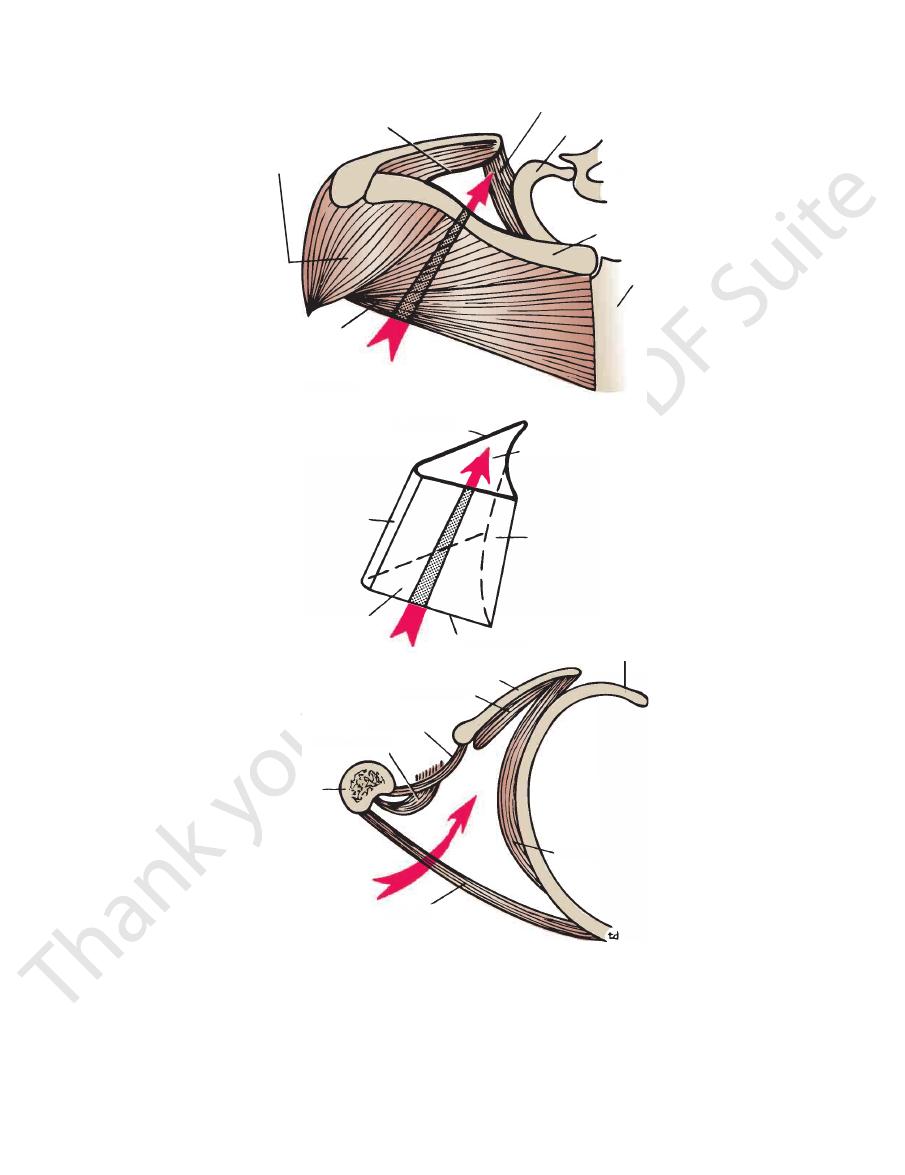
beneath the pectoralis major (Fig. 9.13). It arises from the
The pectoralis minor is a thin triangular muscle that lies
Pectoralis Minor
Key Muscles in the Axilla
Tables 9.1, 9.2, and 9.3.
muscles forming the walls of the axilla are described in
The origins, insertions, nerve supply, and actions of the
the upper limb and many lymph nodes.
The axilla contains the principal vessels and nerves to
rior and posterior walls (Fig. 9.14).
is formed by the skin stretching between the ante
The
in the bicipital groove of the humerus (Figs. 9.14, 9.15,
By the coracobrachialis and biceps muscles
Lateral wall:
(Figs. 9.14, 9.15, and 9.16)
costal spaces covered by the serratus anterior muscle
By the upper four or five ribs and the inter
Medial wall:
9.14, 9.15, and 9.16)
and teres major muscles from above down (Figs. 9.13,
By the subscapularis, latissimus dorsi,
Posterior wall:
major; CF, pull of common flexure muscles; TR, triceps; SUB, subscapularis.
bony fragments on the site of the fracture line and the pull of the muscles. S, supraspinatus; D, deltoid; PM, pectoralis
Common fractures of the radius and ulna. The displacement of the
Common fractures of the humerus. B.
■
■
■
■
-
■
■
and 9.16)
base
-
-
Basic Anatomy
345
superior border of scapula
deltoid
serratus anterior
first rib
T1
clavicle
sternum
inlet from above
pectoralis
major
posterior wall
lateral wall
outlet
inlet
medial wall
anterior wall
subscapularis
teres major
latissimus dorsi
humerus
pectoralis
major
serratus anterior
outlet
walls
fourth rib
scapula
T1
clavicle
stern
rom above
ctoralis
major
posterior wall
lateral wall
outlet
inlet
medial wall
anterior wall
subscapularis
teres major
latissimus dorsi
rus
pectoralis
major
serratus anterior
fourth rib
scapula
FIGURE 9.11
Inlet, walls, and outlet of the right axilla.
346
CHAPTER 9
The Upper Limb
cephalic vein
deltoid
acromium
trapezius
supraclavicular nerves
sternocleidomastoid
external oblique aponeurosis
lateral thoracic artery
long thoracic nerve
serratus anterior
intercostobrachial nerve
teres major
latissimus dorsi
subscapularis
medial cutaneous nerve of arm
axillary vein
axillary artery
long head of triceps
biceps and
coracobrachialis
clavicle
manubrium sterni
body of sternum
pectoralis major
cutaneous branches of
intercostal nerves
xiphoid process
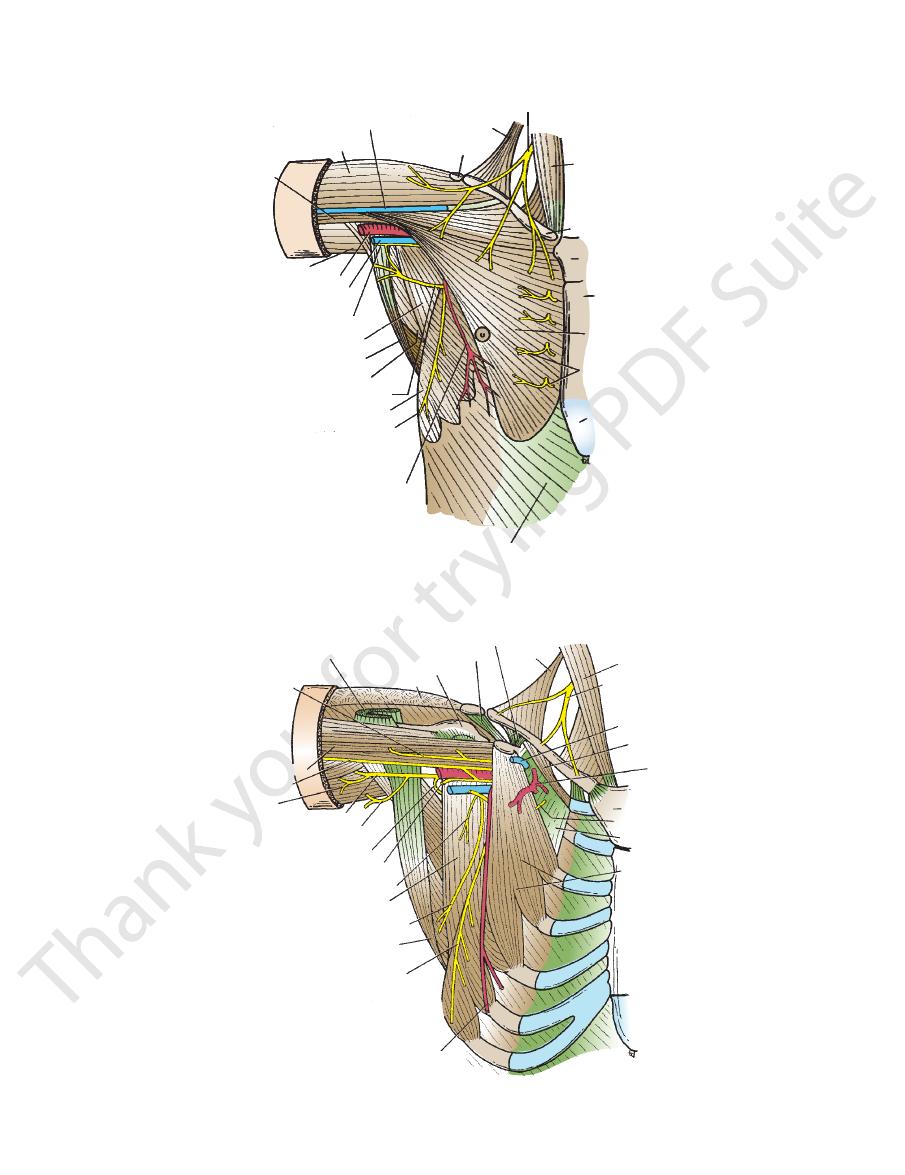
FIGURE 9.12
Pectoral region and axilla.
pectoralis major
musculocutaneous nerve
median nerve
nerves to the triceps
radial nerve
posterior cutaneous nerve of arm
axillary nerve
ulnar nerve
lower subscapular nerve
subscapularis
middle subscapular nerve
latissimus dorsi
long thoracic nerve
lateral thoracic artery
pectoralis minor
clavipectoral fascia
lateral pectoral nerve
manubrium sterni
thoracoacromial
artery
subclavius
cephalic vein
supraclavicular nerves
sternocleidomastoid
trapezius
coracoclavicular ligament
coracoacromial ligament
greater tuberosity
deltoid
coracobrachialis
FIGURE 9.13
Pectoral region and axilla; the pectoralis major muscle has been removed to display the underlying structures.
Basic Anatomy
347
long thoracic nerve
anterior intercostal membrane
levator scapulae
trapezius
dorsal scapular nerve
suprascapular nerve
lateral cord of brachial plexus
musculocutaneous
nerve
radial nerve
axillary nerve
subscapular nerves
thoracodorsal nerve
subscapular artery
subscapularis
serratus anterior
external intercostal muscle
short head of biceps
coraco-brachialis
medial head of triceps
long head of triceps
pectoralis major
deltoid
pectoralis minor
axillary vein
subclavius muscle
C5
6
7
8
T1
nerve to subclavius
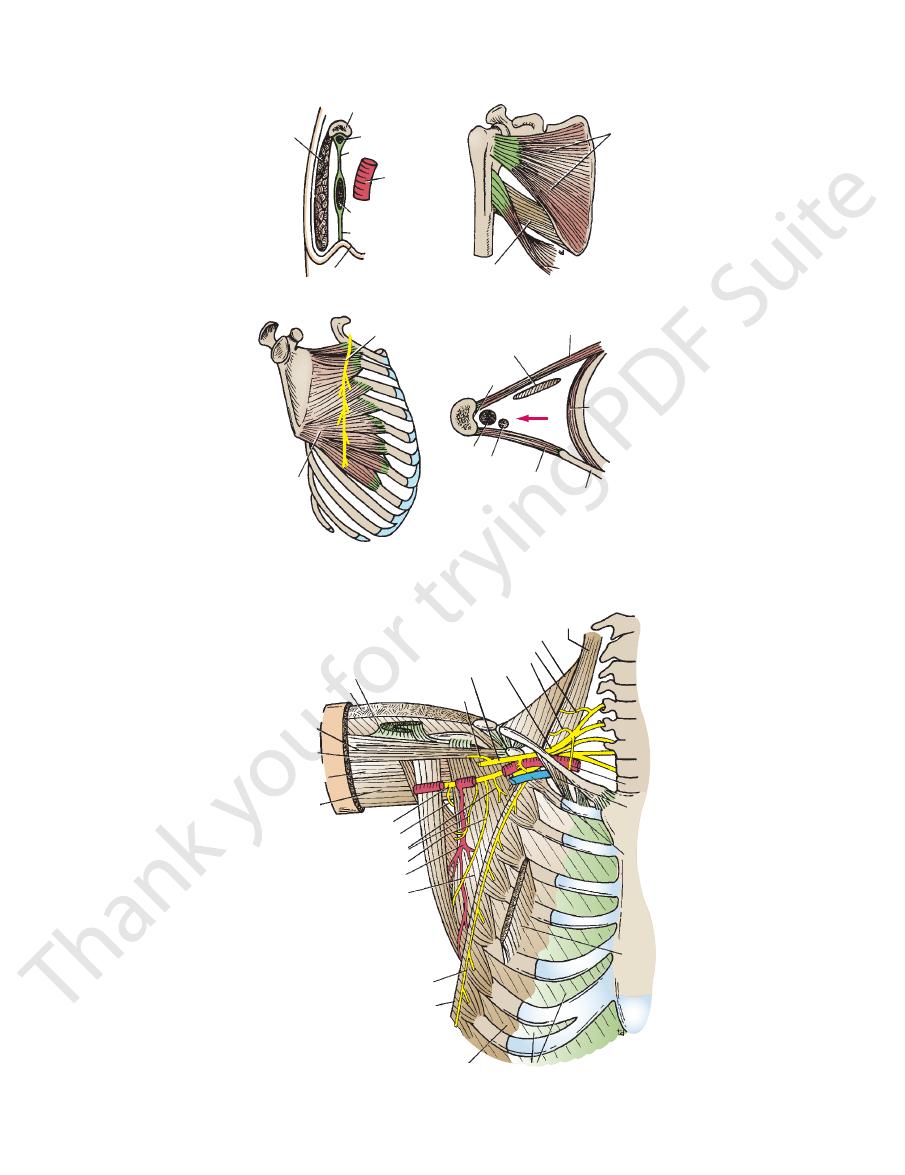
FIGURE 9.15
Pectoral region and axilla; the pectoralis major and minor muscles and the clavipectoral fascia have been
removed to display the underlying structures.
clavicle
subclavius
clavipectoral fascia
axillary
artery
pectoralis minor
suspensory
ligament
deep fascia of armpit
anterior wall
subscapularis
latissimus dorsi
teres major
posterior wall
long thoracic nerve
serratus
anterior
medial wall
pectoralis minor
pectoralis major
serratus anterior
scapula
teres major
coracobrachialis
biceps
bicipital groove
of humerus
lateral wall
pectoralis
major
FIGURE 9.14
Structures that form the walls of the axilla. The lateral wall is indicated by the arrow.
348
CHAPTER 9
The Upper Limb
Muscles Connecting the Upper Limb to the Thoracic Wall
T A B L E 9 . 1
Muscle
Origin
Insertion
Nerve Supply
Nerve Roots
a
Action
Pectoralis major
Clavicle, sternum,
and upper six
costal cartilages
Lateral lip of
bicipital groove
of humerus
Medial and lateral
pectoral nerves from
brachial plexus
C5, 6, 7, 8; T1
Adducts arm and rotates
it medially; clavicular
fibers also flex arm
Pectoralis minor
3rd, 4th, and
5th ribs
Coracoid process
of scapula
Medial pectoral nerve
from brachial plexus
C6, 7, 8
Depresses point of
shoulder; if the scapula
is fixed, it elevates the
ribs of origin
Subclavius
1st costal cartilage
Clavicle
Nerve to subclavius
from upper trunk of
brachial plexus
C5, 6
Depresses the clavicle
and steadies this bone
during movements of
the shoulder girdle
Serratus anterior
Upper eight ribs
Medial border
and inferior
angle of
scapula
Long thoracic nerve
C5, 6, 7
Draws the forward
anterior around the
thoracic wall; rotates
scapula
a
The predominant nerve root supply is indicated by boldface type.
musculocutaneous
nerve
short head
of biceps
long head of biceps
median
nerve
subscapular
artery
subscapularis
latissimus
dorsi
RIGHT SIDE
tendon of pectoralis major (reflected)
tendon of pectoralis minor (cut)
lateral chord of
brachial plexus
coracoid process
clavicle
axillary artery
axillary vein (cut)
subclavius
manubrium
sterni
body of
sternum
lateral thoracic
artery
thoracodorsal
nerve
serratus anterior
external
oblique
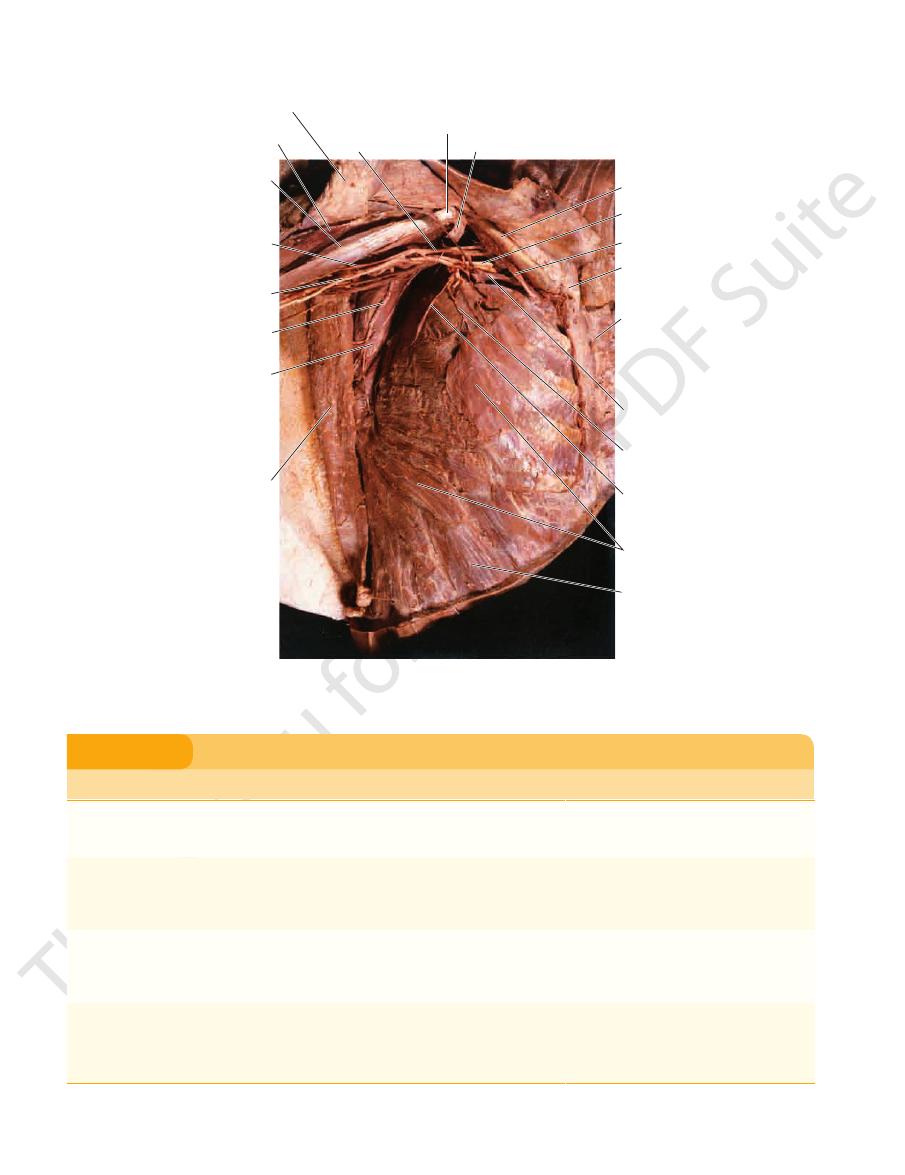
FIGURE 9.16
ascia have been
Dissection of the right axilla. The pectoralis major and minor muscles and the clavipectoral f
removed to display the underlying structures.
Basic Anatomy
349
Muscles Connecting the Upper Limb to the Vertebral Column
T A B L E 9 . 2
Transverse processes
Trapezius
Muscle
Origin
Insertion
Nerve Supply
Nerve Roots
a
Action
Occipital bone,
ligamentum nuchae,
spine of 7th cervical
vertebra, spines of all
thoracic vertebrae
Upper fibers into
lateral third of
clavicle; middle and
lower fibers into
acromion and spine
of scapula
Spinal part of
accessory
nerve (motor)
and C3 and 4
(sensory)
XI cranial
nerve (spinal
part)
Upper fibers elevate
the scapula; middle
fibers pull scapula
medially; lower fibers
pull medial border of
scapula downward
Latissimus
dorsi
Iliac crest, lumbar fascia,
spines of lower six
thoracic vertebrae,
lower three or four
ribs, and inferior angle
of scapula
Floor of bicipital
groove of humerus
Thoracodorsal
nerve
C6, 7, 8,
Extends, adducts, and
medially rotates the
arm
Levator
scapulae
of 1st four cervical
vertebrae
Medial border of
scapula
C3 and 4 and
dorsal
scapular
nerve
C3, 4, 5
Raises medial border of
scapula
Rhomboid
minor
Ligamentum nuchae and
spines of 7th cervical
and 1st thoracic
vertebrae
Medial border of
scapula
Dorsal scapular
nerve
C4, 5
Raises medial border of
scapula upward and
medially
Rhomboid
major
Second to 5th thoracic
spines
Medial border of
scapula
Dorsal scapular
nerve
C4, 5
Raises medial border of
scapula upward and
medially
a
The predominant nerve root supply is indicated by boldface type.
Muscles Connecting the Scapula to the Humerus
T A B L E 9 . 3
Teres minor
Teres major
Muscle
Origin
Insertion
Nerve Supply
Nerve Roots
a
Action
Deltoid
Lateral third
of clavicle,
acromion, spine
of scapula
Middle of lateral
surface of shaft
of humerus
Axillary nerve
C5, 6
Abducts arm; anterior fibers
flex and medially rotate
arm; posterior fibers extend
and laterally rotate arm
Supraspinatus
Supraspinous fossa
of scapula
Greater tuberosity
of humerus;
capsule of
shoulder joint
Suprascapular
nerve
C4, 5, 6
Abducts arm and stabilizes
shoulder joint
Infraspinatus
Infraspinous fossa
of scapula
Greater tuberosity
of humerus;
capsule of
shoulder joint
Suprascapular
nerve
(C4), 5, 6
Laterally rotates arm and
stabilizes shoulder joint
Lower third of
lateral border of
scapula
Medial lip of
bicipital groove
of humerus
Lower subscapular
nerve
C6, 7
Medially rotates and adducts
arm and stabilizes shoulder
joint
Upper two thirds of
lateral border of
scapula
Greater tuberosity
of humerus;
capsule of
shoulder joint
Axillary nerve
(C4), C5, 6
Laterally rotates arm and
stabilizes shoulder joint
Subscapularis
Subscapular fossa
Lesser tuberosity of
humerus
Upper and lower
subscapular
nerves
C5, 6, 7
Medially rotates arm and
stabilizes shoulder joint
a
The predominant nerve root supply is indicated by boldface type.
350
CHAPTER 9
lary artery and divides it into three parts (Figs. 9.13, 9.15,
The pectoralis minor muscle crosses in front of the axil
of the neck, it is seen to be continuous with the prevertebral
If this sheath is traced upward into the root
axillary sheath.
enclosed with them in a connective tissue sheath called the
the cords of the brachial plexus and their branches and is
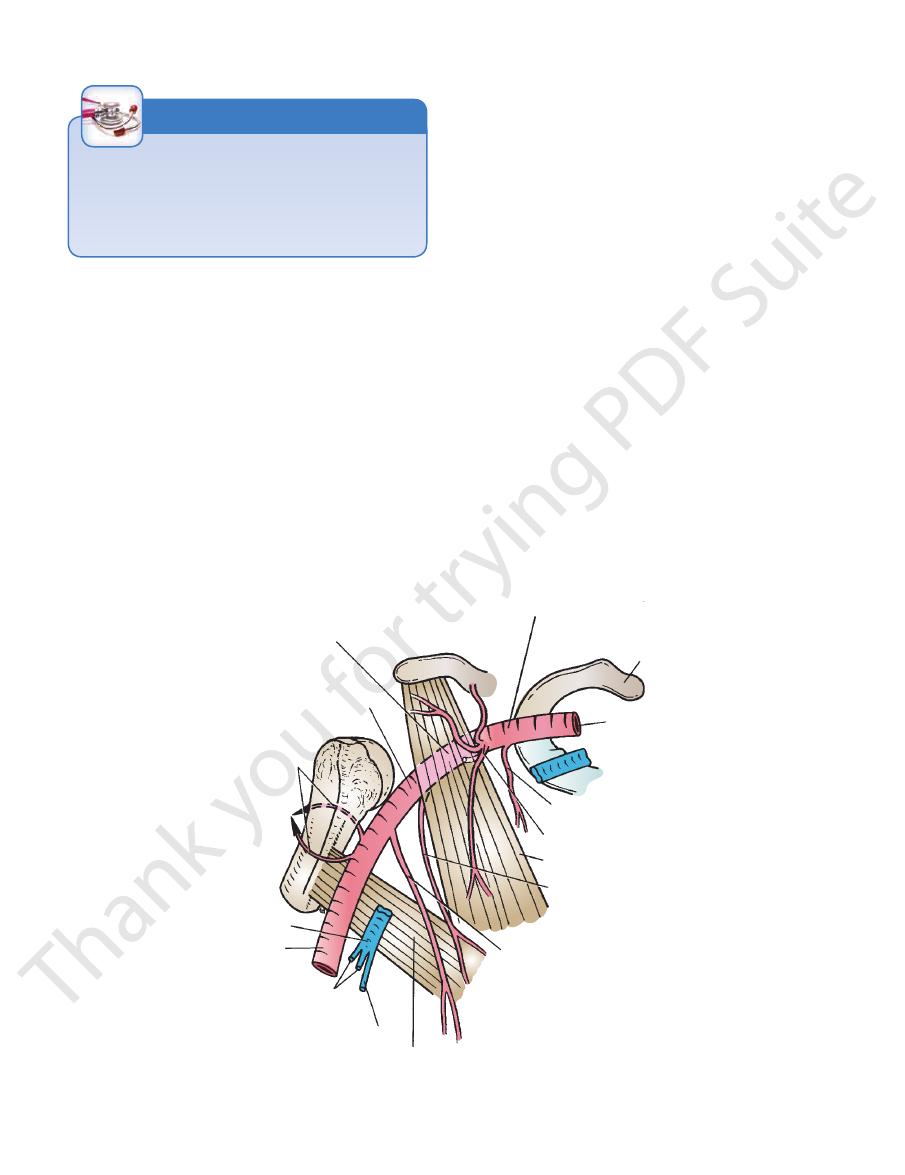
artery. Throughout its course, the artery is closely related to
the teres major muscle, where it continues as the brachial
the subclavian (Fig. 9.17) and ends at the lower border of
at the lateral border of the 1st rib as a continuation of
The axillary artery (Figs. 9.12, 9.13, 9.15, and 9.16) begins
Axillary Artery
limb. These structures are embedded in fat.
plexus, the brachial plexus, which innervates the upper
The Upper Limb
fascia.
-
and 9.17).
Absent Pectoralis Major
Occasionally, parts of the pectoralis major muscle may be
absent. The sternocostal origin is the most commonly missing
part, and this causes weakness in adduction and medial rota-
tion of the shoulder joint.
C L I N I C A L N O T E S
First Part of the Axillary Artery
the subscapularis muscle, and the shoulder joint
The posterior cord of the brachial plexus,
Posteriorly:
and the skin (Figs. 9.13 and 9.17)
The pectoralis minor, the pectoralis major,
Anteriorly:
Relations
pectoralis minor muscle (Fig. 9.17).
This lies behind the
Second Part of the Axillary Artery
The axillary vein (Fig. 9.15 and 9.16)
Medially:
The three cords of the brachial plexus (Fig. 9.15)
Laterally:
ratus anterior) (Fig. 9.15)
The long thoracic nerve (nerve to the ser
Posteriorly:
cephalic vein crosses the artery (Figs. 9.13 and 9.15).
The pectoralis major and the skin. The
Anteriorly:
Relations
pectoralis minor (Fig. 9.17).
lateral border of the 1st rib to the upper border of the
This extends from the
■
■
■
■
-
■
■
■
■
■
■
■
■
(Fig. 9.15)
the teres major (Fig. 9.17).
lower border of the pectoralis minor to the lower border of
This extends from the
Third Part of the Axillary Artery
the axillary vein (Figs. 9.15, 9.16, and 9.20)
The medial cord of the brachial plexus and
Medially:
9.13, 9.15, and 9.16)
The lateral cord of the brachial plexus (Figs.
Laterally:
■
■
■
■
second part of axillary artery
third part of axillary artery
anterior and posterior
circumflex humeral
arteries
axillary vein
brachial artery
venae comitantes
of brachial artery
basilic vein
teres major
subscapular artery
lateral thoracic artery
pectoralis minor
thoracoacromial artery
highest thoracic artery
subclavian artery
first rib
first part of axillary artery
FIGURE 9.17
Parts of the axillary artery and its branches. Note the formation of the axillary vein at the lower border of the
teres major muscle.
Basic Anatomy
branches of the axillary artery, and the cephalic vein.
The vein receives tributaries, which correspond to the
subclavian vein.
ends at the lateral border of the 1st rib by becoming the
It runs upward on the medial side of the axillary artery and
tantes of the brachial artery and the basilic vein (Fig. 9.17).
of the teres major muscle by the union of the venae comi
The axillary vein (Fig. 9.12) is formed at the lower border
Axillary Vein
of the humerus, respectively (Fig. 9.17).
wind around the front and the back of the surgical neck
posterior circumflex humeral arter
anterior
The
subscapularis muscle.
runs along the lower border of the
subscapular artery
The
From the third part:
of the pectoralis minor (Fig. 9.17).
runs along the lower border
lateral thoracic artery
The
terminal branches.
immediately divides into
thoracoacromial artery
The
From the second part:
upper border of the pectoralis minor.
is small and runs along the
highest thoracic artery
The
From the first part:
Branches of the Axillary Artery
medial cutaneous nerve of the arm (Fig. 9.13)
The ulnar nerve, the axillary vein, and the
Medially:
culocutaneous nerves also lies on the lateral side (Figs.
humerus. The lateral root of the median and the mus
The coracobrachialis, the biceps, and the
Laterally:
behind the artery (Figs. 9.15 and 9.16).
the teres major. The axillary and radial nerves also lie
The subscapularis, the latissimus dorsi, and
Posteriorly:
the median nerve (Fig. 9.13).
lower down the artery, it is crossed by the medial root of
The pectoralis major for a short distance;
Anteriorly:
Relations
351
■
■
■
■
■
■
-
9.13 and 9.16).
■
■
and
-
ies
-
duce the nerve block. The position of the sheath can be verified
of the sheath. The anesthetic solution is then injected into the
pressure, and a syringe needle is inserted into the proximal part
be obtained. The distal part of the sheath is closed with finger
the brachial plexus, a brachial plexus nerve block can easily
Because the axillary sheath encloses the axillary vessels and
Spontaneous Thrombosis of the Axillary Vein
Spontaneous thrombosis of the axillary vein occasionally
occurs after excessive and unaccustomed movements of the
arm at the shoulder joint.
The Axillary Sheath and a Brachial Plexus Nerve
Block
sheath, and the solution is massaged along the sheath to pro-
by feeling the pulsations of the third part of the axillary artery.
C L I N I C A L N O T E S
Brachial Plexus
the axillary artery (Figs. 9.15 and 9.20). The medial cord
brachial plexus lie above and lateral to the first part of
All three cords of the
Cords of the Brachial Plexus
are enclosed in the axillary sheath.
Here, the brachial plexus and the axillary artery and vein
arranged around the axillary artery in the axilla (Fig. 9.15).
and are fully described on page XXX. The cords become
reside in the lower part of the posterior triangle of the neck
The roots, trunks, and divisions of the brachial plexus
posterior cord.
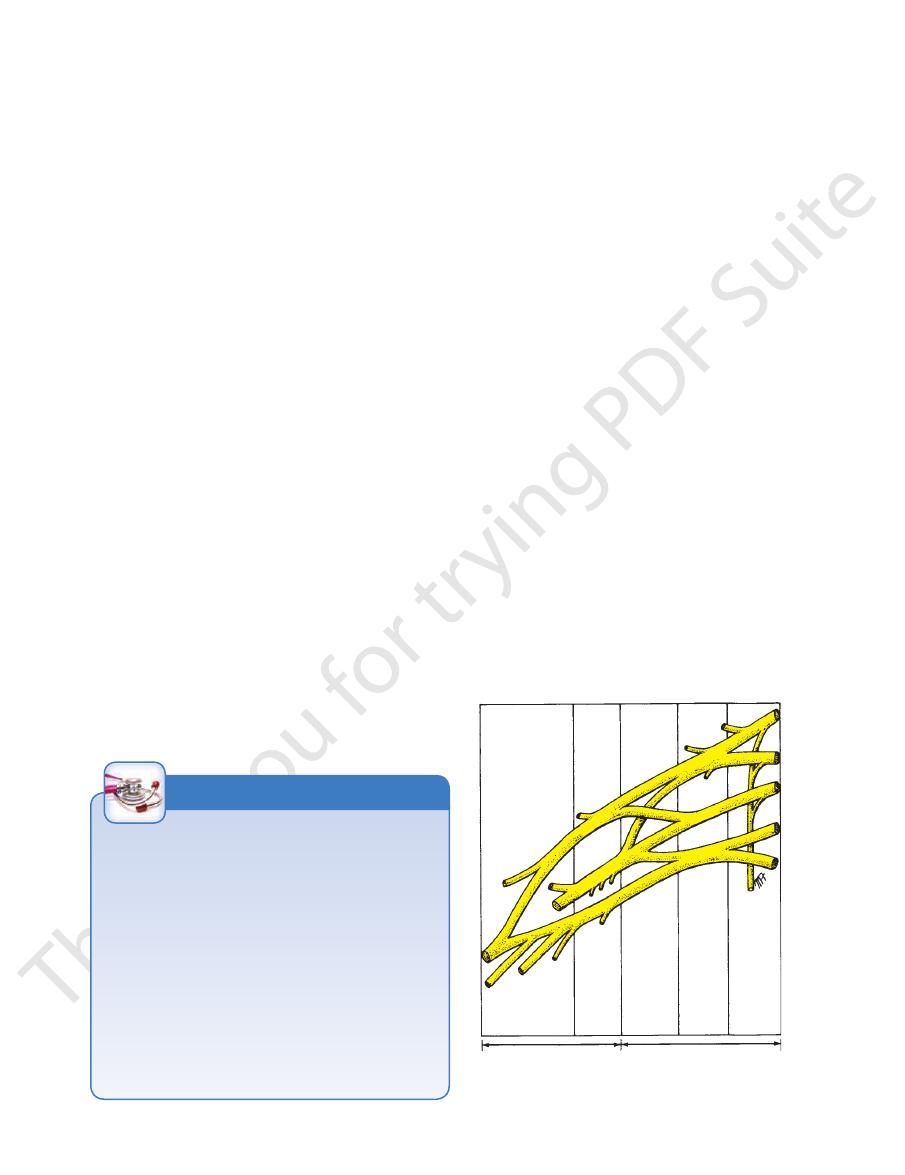
divisions of all three trunks join to form the
and the posterior
medial cord,
lower trunk continues as the
the anterior division of the
lateral cord,
unite to form the
sions. The anterior divisions of the upper and middle trunks
Each trunk then divides into anterior and posterior divi
lower trunk.
and the roots of C8 and T1 unite to form the
middle trunk,
the root of C7 continues as the
upper trunk,
(Fig. 9.18). The roots of C5 and 6 unite to form the
cords
roots, trunks, divisions,
The plexus can be divided into
the 1st thoracic spinal nerves (Figs. 9.18 and 9.19).
of the anterior rami of the 5th, 6th, 7th, and 8th cervical and
is formed in the posterior triangle of the neck by the union
to the various parts of the upper limb. The brachial plexus
arranged and distributed efficiently in different nerve trunks
ers derived from different segments of the spinal cord to be
This allows the nerve fib
brachial plexus.
plexus called the
At the root of the neck, the nerves form a complicated
secretomotor supply to the sweat glands.
sels by the sympathetic vasomotor nerves; and sympathetic
the muscles; influence over the diameters of the blood ves
deep structures, such as the joints; motor innervation to
important functions: sensory innervation to the skin and
The nerves entering the upper limb provide the following
-
-
and
-
main branches cords
divisions trunks
roots
lateral
upper
posterior
middle
medial
lower
anterior
rami
C5
6
7
8
T1
axilla
posterior triangle of neck
FIGURE 9.18
The formation of the main parts of the brachial
plexus. Note the locations of the different parts.

352
CHAPTER 9
of the axillary artery (Fig. 9.20).
the medial cord of the brachial plexus and descends in front
arises from
medial cutaneous nerve of the forearm
The
the skin on the medial side of the arm.
cutaneous branch of the 2nd intercostal nerve). It supplies
9.20) and is joined by the intercostobrachial nerve (lateral
from the medial cord of the brachial plexus (Figs. 9.12 and
(T1) arises
medial cutaneous nerve of the arm
The
muscle, and supplies the pectoralis major muscle (Fig. 9.19).
the brachial plexus, supplies and pierces the pectoralis minor
arises from the medial cord of
medial pectoral nerve
The
no branches in the axilla.
eral side of the axillary artery. The median nerve gives off
median nerve trunk, and this passes downward on the lat
9.13 and 9.19). It is joined by the medial root to form the
tinuation of the lateral cord of the brachial plexus (Figs.
is the direct con
lateral root of the median nerve
The
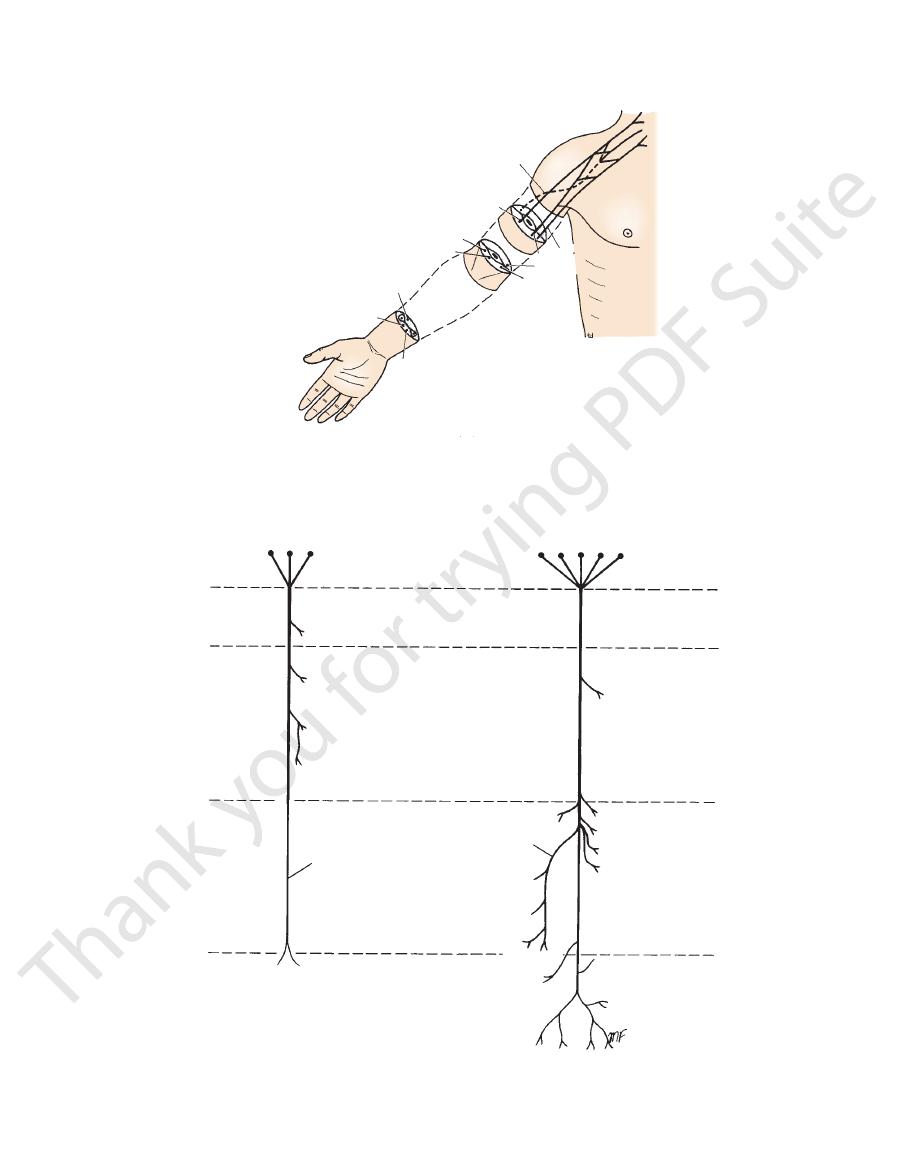
the musculocutaneous nerve is given in Figure 9.22.
9.13 and 9.20). A summary of the complete distribution of
muscle, and leaves the axilla by piercing that muscle (Figs.
cord of the brachial plexus, supplies the coracobrachialis
arises from the lateral
musculocutaneous nerve
The
cle (Figs. 9.13 and 9.20).
the brachial plexus and supplies the pectoralis major mus
arises from the lateral cord of
lateral pectoral nerve
The
anterior muscle, which it supplies.
and 9.19). It descends over the lateral surface of the serratus
behind the axillary vessels and brachial plexus (Figs. 9.15
axilla by passing down over the lateral border of the 1st rib
roots of the brachial plexus in the neck and enters the
(C5, 6, and 7) arises from the
long thoracic nerve
The
accessory phrenic nerve.
phrenic nerve; this branch, when present, is referred to as
clinically because it may give a contribution (C5) to the
clavius muscle (Figs. 9.15, 9.19, and 9.20). It is important
(C5 and 6) supplies the sub
nerve to the subclavius
The
Branches of the Brachial Plexus Found in the Axilla
are summarized in Table 9.4.
The branches of the brachial plexus and their distribution
Radial nerve
Axillary nerve
Thoracodorsal nerve
Upper and lower subscapular nerves
Posterior cord
Medial root of median nerve
Ulnar nerve
nerve of forearm
Medial cutaneous nerve of arm and medial cutaneous
Medial pectoral nerve
Medial cord
Lateral root of median nerve
Musculocutaneous nerve
Lateral pectoral nerve
Lateral cord
infraspinatus muscles)
Suprascapular nerve (supplies the supraspinatus and
Nerve to subclavius (C5 and 6)
Upper trunk
Long thoracic nerve (C5, 6, and 7)
Dorsal scapular nerve (C5)
Roots
plexus (Figs. 9.19 and 9.21) are as follows:
of the different parts of the brachial
branches
The
artery in its third part (Fig. 9.20).
trunks of the upper limb continue this relationship to the
Most branches of the cords that form the main nerve
cated by their names.
ship to the second part of the axillary artery that is indi
(Fig. 9.20). Thus, the cords of the plexus have the relation
cord lies on the lateral side of the second part of the artery
lies behind the second part of the artery, and the lateral
second part of the artery (Fig. 9.20). The posterior cord
crosses behind the artery to reach the medial side of the
The Upper Limb
-
-
■
■
■
■
■
■
■
■
■
■
-
the
-
-
-
dorsal scapular nerve
nerve to subclavius
suprascapular nerve
lateral pectoral nerve
thoracodorsal nerve
musculocutaneous nerve
axillary nerve
radial nerve
median nerve
ulnar nerve
medial cutaneous nerve of the forearm
medial cutaneous nerve of the arm
medial pectoral nerve
upper and lower
subscapular nerves
long thoracic nerve
T1
8
7
6
C5
FIGURE 9.19
Roots, trunks, divisions, cords, and terminal branches of the brachial plexus.

Basic Anatomy
posterior cord of the brachial plexus and supply the upper
arise from the
upper and lower subscapular nerves
The
given in Figure 9.22.
gram of the complete distribution of the median nerve is
of the median nerve (Figs. 9.13 and 9.20). A summary dia
the third part of the axillary artery to join the lateral root
medial cord of the brachial plexus and crosses in front of
arises from the
medial root of the median nerve
The
given in Figure 9.23.
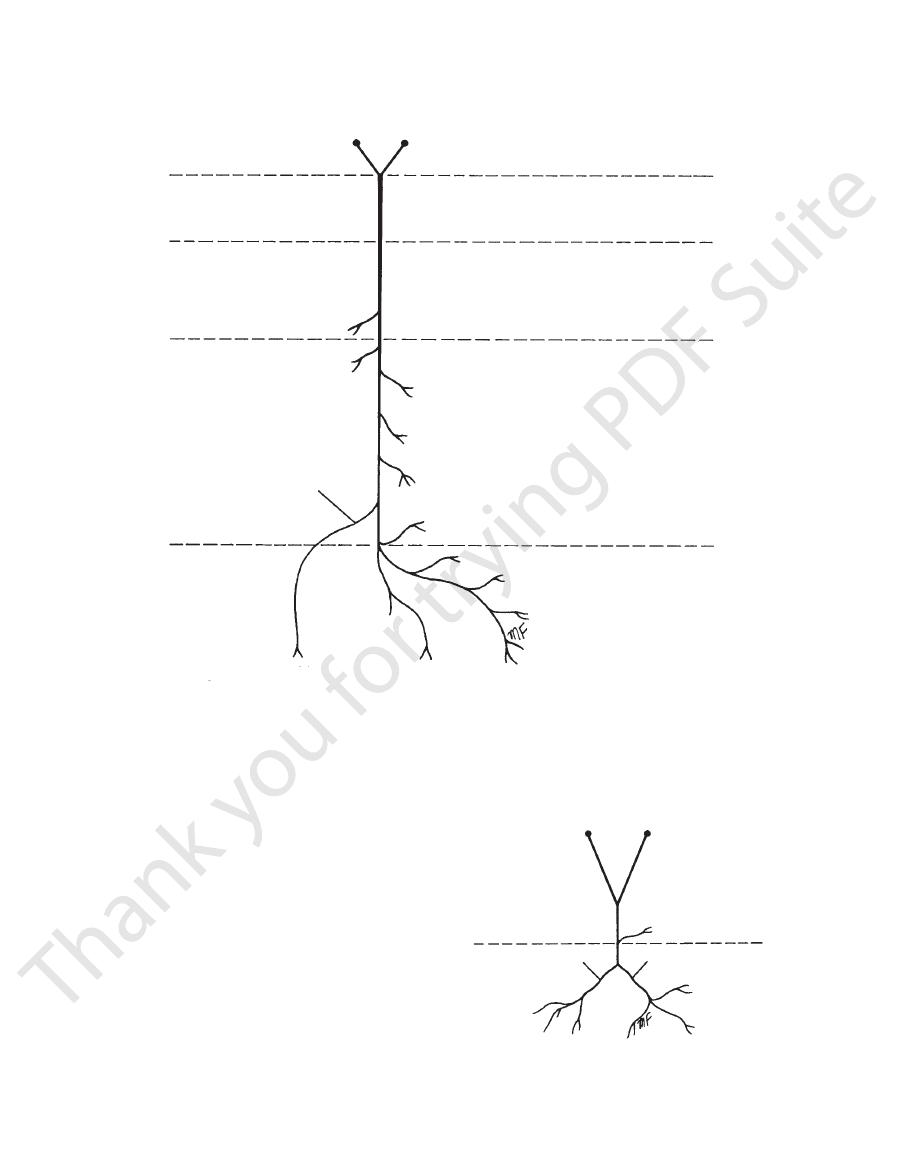
mary of the complete distribution of the ulnar nerve is
The ulnar nerve gives off no branches in the axilla. A sum
between the axillary artery and vein (Figs. 9.13 and 9.20).
cord of the brachial plexus and descends in the interval
(C8 and T1) arises from the medial
ulnar nerve
The
353
-
-
and lower parts of the subscapularis muscle. In addition,
the lower subscapular nerve supplies the teres muscle
(Figs. 9.15 and 9.19).
and lies behind the axillary artery (Figs. 9.15, 9.19, and 9.20).
is the largest branch of the brachial plexus
radial nerve
The
Figure 9.24.
complete distribution of the axillary nerve is given in
posterior branches (see page 361). A summary of the
branch to the shoulder joint, it divides into anterior and
quadrangular space (see page 361). Having given off a
and 9.19). It turns backward and passes through the
of the posterior cord of the brachial plexus (Figs. 9.15
is one of the terminal branches
axillary nerve
The
latissimus dorsi muscle (Figs. 9.15 and 9.19).
of the brachial plexus and runs downward to supply the
arises from the posterior cord
thoracodorsal nerve
The
medial cutaneous nerve of arm
axillary vein
medial cutaneous nerve of forearm
axillary artery
axillary vein
medial cutaneous nerve of arm
axillary artery
nerve to subclavius
lateral pectoral nerve
suprascapular nerve
dorsal scapular nerve
C5
6
7
8
T1
long thoracic nerve
pectoralis minor
ulnar nerve
radial nerve
median nerve
musculocutaneous nerve
pectoralis major
teres major
ulnar nerve
radial nerve
median nerve
musculocutaneous nerve
coracobrachialis
humerus
bicipital groove
biceps
medial cutaneous nerve
of forearm
A
B
FIGURE 9.20
A.
the level of the teres major muscle.
Relations of the brachial plexus and its branches to the axillary artery and vein. B. Section through the axilla at
354
CHAPTER 9
The Upper Limb
Summary of the Branches of the Brachial Plexus and their Distribution
T A B L E 9 . 4
surface of lateral three and a half fingers; articular branches to elbow, wrist,
first two lumbricals (by way of anterior interosseous branch), flexor pollicis
superficialis, abductor pollicis brevis, flexor pollicis brevis, opponens pollicis,
third and fourth lumbricals, interossei, palmaris brevis, skin of medial half of
Flexor carpi ulnaris and medial half of flexor digitorum profundus, flexor digiti
of lateral three and a half fingers; articular branches to elbow, wrist, and
nerve of forearm; skin on lateral side of dorsum of hand and dorsal surface
nerve of arm, posterior cutaneous nerve of arm, and posterior cutaneous
pollicis longus, extensor pollicis brevis; skin, lower lateral cutaneous
extensor digiti minimi, extensor indicis, abductor pollicis longus, extensor
extensor carpi radialis brevis, extensor carpi ulnaris, extensor digitorum,
deep radial nerve branch supplies extensor muscles of forearm: supinator,
Triceps, anconeus, part of brachialis, extensor carpi radialis longus; via
Deltoid and teres minor muscles; upper lateral cutaneous nerve of arm supplies
Coracobrachialis, biceps brachii, brachialis muscles; supplies skin along lateral
Upper Trunk
Rhomboid minor, rhomboid major, levator scapulae muscles
Branches
Distribution
Roots
Dorsal scapular nerve (C5)
Long thoracic nerve (C5, 6, 7)
Serratus anterior muscle
Suprascapular nerve (C5, 6)
Supraspinatus and infraspinatus muscles
Nerve to subclavius (C5, 6)
Subclavius
Lateral Cord
Lateral pectoral nerve (C5, 6, 7)
Pectoralis major muscle
Musculocutaneous nerve (C5, 6, 7)
border of forearm when it becomes the lateral cutaneous nerve of forearm
Lateral root of median nerve (C5, 6, 7)
See medial root of median nerve
Posterior Cord
Upper subscapular nerve (C5, 6)
Subscapularis muscle
Thoracodorsal nerve (C6, 7, 8)
Latissimus dorsi muscle
Lower subscapular nerve (C5, 6)
Subscapularis and teres major muscles
Axillary nerve (C5, 6)
skin over lower half of deltoid muscle
Radial nerve (C5, 6, 7, 8; T1)
hand
Medial Cord
Medial pectoral nerve (C8; T1)
Pectoralis major and minor muscles
Medial cutaneous nerve of arm joined by
intercostal brachial nerve from second
intercostal nerve (C8; T1, 2)
Skin of medial side of arm
Medial cutaneous nerve of forearm (C8; T1)
Skin of medial side of forearm
Ulnar nerve (C8; T1)
minimi, opponens digiti minimi, abductor digiti minimi, adductor pollicis,
dorsum of hand and palm, skin of palmar and dorsal surfaces of medial one
and a half fingers
Medial root of median nerve (with lateral root)
forms median nerve (C5, 6, 7, 8; T1)
Pronator teres, flexor carpi radialis, palmaris longus, flexor digitorum
longus, flexor digitorum profundus (lateral half), pronator quadratus; palmar
cutaneous branch to lateral half of palm and digital branches to palmar
and carpal joints
Basic Anatomy
355
median nerve
deep branch of radial nerve
musculocutaneous nerve
radial nerve
musculocutaneous nerve
radial nerve
ulnar nerve
median nerve
ulnar nerve
median
nerve
ulnar nerve
C5
6
7
8
T1
FIGURE 9.21
ferent fascial compartments of the arm and forearm.
Distribution of the main branches of the brachial plexus to dif
musculocutaneous nerve
median nerve
C5 C6 C7 C8 T1
C5 C6 C7
axilla
coracobrachialis
biceps
upper arm
brachialis
(greater part)
elbow joint
forearm
lateral cutaneous
nerve of forearm
hand
no branches
brachial
plexus
brachial artery
elbow joint
anterior interosseous
nerve
flexor pollicis
longus
flexor digitorum
profundus (lateral half)
pronator quadratus
palmar cutaneous branch
wrist joint
pronator teres
flexor carpi radialis
palmaris longus
flexor digitorum
superficialis
three thenar muscles
first two lumbricals
palmar digital branches
to lateral 3
1
/
2
fingers
FIGURE 9.22
Summary of the main branches of the musculocutaneous and median nerves.
356
CHAPTER 9
abdominal wall above the level of the umbilicus.
the breast and superficial vessels from the anterolateral
nodes receive lymph vessels from the lateral quadrants of
of the pectoralis minor behind the pectoralis major, these
Lying along the lower border
Anterior (pectoral) group:
The lymph nodes are arranged in six groups (Fig. 9.26).
upper limb.
above the level of the umbilicus, and the vessels from the
superficial lymph vessels from the thoracoabdominal walls
lymph vessels from the lateral quadrants of the breast, the
The axillary lymph nodes (20 to 30 in number) drain
Lymph Nodes of the Axilla
described on page 429.
Lesions of the brachial plexus and its branches are
distribution of the radial nerve is given in Figure 9.25.
middle of the back of the arm. A summary of the complete
(Fig. 9.13). The latter branch is distributed to the skin on the
triceps muscle and the posterior cutaneous nerve of the arm
It gives off branches to the long and the medial heads of the
The Upper Limb
■
■
ulnar nerve
C8
T1
axilla
upper arm
forearm
hand
elbow joint
flexor carpi ulnaris
posterior cutaneous branch
skin of medial side
of dorsum of hand
and medial 1
1/2
fingers
palmar digital
branches to medial
1
1/2
fingers
palmaris
brevis
no branches
brachial plexus
flexor digitorum
profundus (medial half)
ulnar artery
palmar cutaneous branch
wrist joint
muscles of hypothenar eminence
adductor pollicis
third and fourth lumbricals
interossei
joints of hand
FIGURE 9.23
Summary of the main branches of the ulnar nerve.
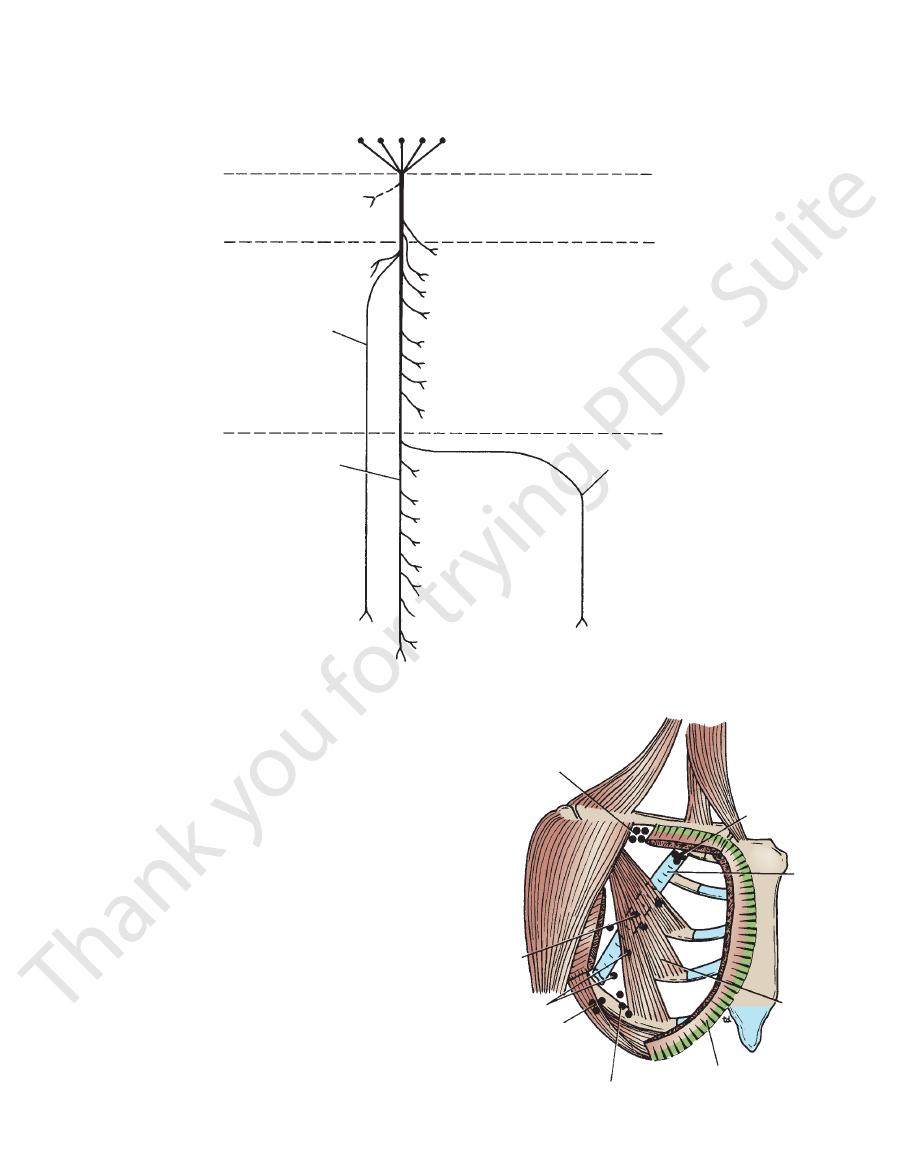
axillary nerve
axilla
scapular
region
skin over lower
half of deltoid
deltoid
anterior branch
posterior branch
shoulder joint
brachial plexus
teres minor
C5
C6
upper lateral cutaneous
nerve of arm to skin
over lower half of deltoid
FIGURE 9.24
Summary of the main branches of the axillary
nerve.
Basic Anatomy
large veins at the root of the neck.
tively, the lymph trunks may drain directly into one of the
the right side, it drains into the right lymph trunk. Alterna
On the left side, this trunk drains into the thoracic duct; on
subclavian lymph trunk.
The apical nodes drain into the
lymph vessels from all the other axillary nodes.
eral border of the 1st rib, these nodes receive the efferent
Lying at the apex of the axilla at the lat
Apical group:
vessels from the lateral side of the hand, forearm, and arm.
pectoralis major muscles and receive superficial lymph
the axilla. They lie in the groove between the deltoid and
not strictly axillary nodes because they are located outside
These nodes are
Infraclavicular (deltopectoral) group:
three groups.
axillary fat, these nodes receive lymph from the above
Lying in the center of the axilla in the
Central group:
ing the lateral side—see infraclavicular nodes, below).
of the upper limb (except those superficial vessels drain
lary vein, these nodes receive most of the lymph vessels
Lying along the medial side of the axil
Lateral group:
the iliac crests.
lymph vessels from the back, down as far as the level of
subscapularis muscle, these nodes receive superficial
Lying in front of the
Posterior (subscapular) group:
357
■
■
■
■
-
-
■
■
■
■
■
■
-
-
lateral 3
fingers
radial nerve
C5 C6 C7 C8 T1
brachial plexus
posterior cutaneous
nerve of arm
axilla
lower lateral
cutaneous nerve
of arm
upper arm
deep branch
of radial nerve
forearm
triceps (long head)
triceps (medial head)
triceps (lateral head)
triceps (medial head)
brachialis (small part)
brachioradialis
extensor carpi
radialis brevis
elbow joint
extensor carpi
supinator
extensor digitorum
extensor digiti minimi
extensor carpi ulnaris
abductor pollicis longus
extensor pollicis longus
extensor pollicis brevis
extensor indicis
posterior cutaneous
nerve of forearm
skin of lateral side of
superficial branch
dorsum of hand and
1/2
FIGURE 9.25
Summary of the main branches of the radial nerve.
infraclavicular group
apical group
axillary
vein
pectoralis
minor
pectoralis major
anterior group
posterior
group
lateral group
central
group
FIGURE 9.26
Different groups of lymph nodes in the axilla.