
years of adult life.
exceedingly common in the population as a whole, especially in the middle to later
. Mild to moderate chronic gastritis is
Disorders of the Stomach
esophageal tube. Antispasmotic drugs (drugs that relax smooth muscle) can also be
rupture and death. Considerable benefit can be achieved by stretching the lower
tion of the esophageal mucosa, sometimes leading to severe substernal pain or even
during the long periods of esophageal stasis. The infection may also cause ulcera-
it often can hold as much as 1 liter of food, which often becomes putridly infected
time. Over months and years, the esophagus becomes tremendously enlarged until
food into the stomach for many hours, instead of the few seconds that is the normal
When achalasia becomes severe, the esophagus often cannot empty the swallowed
as food approaches this sphincter during swallowing.
transmit a signal to cause “receptive relaxation” of the gastroesophageal sphincter
agus remains spastically contracted, and the myenteric plexus has lost its ability to
lower two thirds of the esophagus. As a result, the musculature of the lower esoph-
esophagus then fails to pass from the esophagus into the stomach. Pathological
sphincter fails to relax during swallowing. As a result, food swallowed into the
Achalasia
such patients occasionally choke to death on their own vomitus.
because the anesthetic has blocked the reflex mechanism of swallowing. As a result,
instead of swallowing the materials again, they simply suck them into the trachea
they vomit large quantities of materials from the stomach into the pharynx; then,
occurs when patients are under deep anesthesia. Often, while on the operating table,
swallowing.
into the lungs instead of the esophagus, and (3) failure of the soft palate and
that swallowing cannot occur, (2) failure of the glottis to close so that food passes
When the swallowing mechanism is partially or totally paralyzed, the abnormal-
, can also prevent normal swallowing.
lowing muscles, as occurs in
damaging the swallowing center in the brain stem. Finally, paralysis of the swal-
, can prevent normal swallowing by
diseases, such as
can cause paralysis of significant portions of the swallowing mechanism. Also, a few
Damage to the 5th, 9th, or 10th cerebral nerve
Disorders of Swallowing and of the Esophagus
consequences.
iology. The purpose of this chapter, therefore, is to
C
H
A
P
T
E
R
6
6
819
Physiology of Gastrointestinal
Disorders
Effective therapy for most gastrointestinal disorders
depends on a basic knowledge of gastrointestinal phys-
discuss a few representative types of gastrointestinal
malfunction that have special physiologic bases or
Paralysis of the Swallowing Mechanism.
poliomyelitis or encephalitis
muscle dystrophy or in failure of neuromuscular trans-
mission in myasthenia gravis or botulism
ities that can occur include (1) complete abrogation of the swallowing act so
uvula to close the posterior nares so that food refluxes into the nose during
One of the most serious instances of paralysis of the swallowing mechanism
Achalasia and Megaesophagus.
is a condition in which the lower esophageal
studies have shown damage in the neural network of the myenteric plexus in the
end of the esophagus by means of a balloon inflated on the end of a swallowed
helpful.
Gastritis—Inflammation of the Gastric Mucosa

highly alkaline mucus.
of Brunner of the upper duodenum, which secrete a
glands that secrete mainly mucus, and, finally, the glands
mucous neck cells of the gastric glands, the deep pyloric
plus the mucous cell coating of the stomach mucosa, the
juice are well supplied with mucous glands, beginning
tralization of the gastric acid by duodenal juices. It will
The usual cause of peptic
the jejunum of the small intestine.
end of the stomach or, more rarely, in the lower end of
centimeters of the pylorus. In addition, peptic ulcers fre-
at which peptic ulcers most frequently occur, demon-
Figure 66–1 shows the points in the gastrointestinal tract
of gastric juice or upper small intestinal secretions.
. This is discussed in more detail in
red blood cells to mature in the bone marrow. The result
available from the foods to cause young, newly forming
factor, an adequate amount of vitamin B
is absorbed. And, without intrinsic
In the absence of intrinsic factor, only about 1/50 of
surface. This in turn makes it possible for the vitamin
complex reaches the terminal ileum, the intrinsic
small intestine. Then, when the intrinsic factor–vitamin
from the ileum. That is, intrinsic factor com-
parietal cells that secrete hydrochloric acid. Intrinsic
, secreted by the same
and achlorhydria. Normal gastric secretions contain a
Pernicious Anemia in Gastric Atrophy.
requires an acid medium for activity.
also usually is not secreted; even when it is, the lack of
ished acid secretion. When acid is not secreted, pepsin
Hypochlorhydria
hydrochloric acid; it is diagnosed when the pH of the
Achlorhydria
and, occasionally, to
achlorhy-
also leading eventually to gastric atrophy. Loss of the
develop autoimmunity against the gastric mucosa, this
tion remains. It is also believed that some people
tritis, the mucosa gradually becomes more and more
Gastric Atrophy.
digestion by the peptic digestive enzymes, thus fre-
and atrophy. It also makes the mucosa susceptible to
epithelium, creating additional havoc and leading to a
The hydrogen ions do then diffuse into the stomach
tritis, the permeability of the barrier is greatly increased.
mucus as far as the epithelial membrane itself. In gas-
the concentration of hydrogen ions in plasma, seldom
ions of the gastric juice, averaging about 100,000 times
The gastric barrier normally is resistant enough to dif-
tion are called the “gastric barrier.”
junctions between the adjacent epithelial cells. These
normally slight. This low level of absorption is mainly
often leading to severe acute or chronic gastritis. Two of
barrier—that is, to the mucous glands and to the tight
In addition, certain ingested irritant substances can be
regimen of antibacterial therapy.
This often can be treated successfully by an intensive
the stomach’s own peptic secretions.
mucosa. In a few cases, gastritis can be acute and severe,
deeply into the gastric mucosa, in many long-standing
and therefore not very harmful, or it can penetrate
The inflammation of gastritis may be only superficial
820
Unit XII
Gastrointestinal Physiology
cases causing almost complete atrophy of the gastric
with ulcerative excoriation of the stomach mucosa by
Research suggests that much gastritis is caused
by chronic bacterial infection of the gastric mucosa.
especially damaging to the protective gastric mucosal
epithelial junctions between the gastric lining cells—
the most common of these substances are excesses of
alcohol or aspirin.
Gastric Barrier and Its Penetration in Gastritis.
Absorp-
tion of food from the stomach directly into the blood is
caused by two specific features of the gastric mucosa:
(1) it is lined with highly resistant mucous cells that
secrete a viscid and adherent mucus and (2) it has tight
two together plus other impediments to gastric absorp-
fusion so that even the highly concentrated hydrogen
diffuse even to the slightest extent through the lining
vicious circle of progressive stomach mucosal damage
quently resulting in gastric ulcer.
In many people who have chronic gas-
atrophic until little or no gastric gland digestive secre-
stomach secretions in gastric atrophy leads to
dria
pernicious anemia.
Achlorhydria (and Hypochlorhydria).
means simply that the stomach fails to secrete
gastric secretions fails to decrease below 6.5 after
maximal stimulation.
means dimin-
acid prevents it from functioning because pepsin
Pernicious
anemia is a common accompaniment of gastric atrophy
glycoprotein called intrinsic factor
factor must be present for adequate absorption of
vitamin B
12
bines with vitamin B
12
in the stomach and protects it
from being digested and destroyed as it passes into the
B
12
factor binds with receptors on the ileal epithelial
B
12
to be absorbed.
the vitamin B
12
12
is not made
is pernicious anemia
Chapter 32.
Peptic Ulcer
A peptic ulcer is an excoriated area of stomach or intes-
tinal mucosa caused principally by the digestive action
strating that the most frequent site is within a few
quently occur along the lesser curvature of the antral
the esophagus where stomach juices frequently reflux.
A type of peptic ulcer called a marginal ulcer also often
occurs wherever a surgical opening such as a gastro-
jejunostomy has been made between the stomach and
Basic Cause of Peptic Ulceration.
ulceration is an imbalance between the rate of secretion
of gastric juice and the degree of protection afforded by
(1) the gastroduodenal mucosal barrier and (2) the neu-
be recalled that all areas normally exposed to gastric
with compound mucous glands in the lower esophagus
In addition to the mucus protection of the mucosa,
the duodenum is protected by the alkalinity of the small
Causes:
1. High acid and peptic content
2. Irritation
3. Poor blood supply
4. Poor secretion of mucus
5. Infection, H. pylori
Cardia
Marginal
ulcer
Pylorus
Ulcer
sites
Peptic ulcer.
Figure 66–1
H. pylori, Helicobacter pylori.
boxypolypeptidase, resulting in a vicious circle until
trypsin. Once this happens, the trypsin activates still
in the secretions, and a small
over-
tually, so much trypsinogen accumulates that it
dammed up in the ducts and acini of the pancreas. Even-
common bile duct. The pancreatic enzymes are then
When a gallstone blocks the papilla of Vater, this blocks
together account for more than 90 per cent of all cases.
by a gallstone; the two
blockage of the papilla of Vater
, and the second most common cause is
The most common cause of pancreatitis is
chronic pancreatitis.
pancreas, and this can occur in the form of either
ingested food cannot be used for nutrition, and copious,
and carbohydrates. As a result, large portions of the
sorbed, as well as one third to one half of the proteins
enzymes. Without these enzymes, as much as 60 per cent
pancreatic lipase, and still a few other digestive
motrypsin, carboxypolypeptidase, pancreatic amylase,
Loss of pancreatic juice means loss of trypsin, chy-
because of malignancy.
removed
of Vater, or (3) after the
pancreatic duct is blocked
(which is discussed later), (2) when the
tine. Lack of pancreatic secretion frequently occurs (1)
Abnormal Digestion of Food in the
Disorders of the
patient’s condition is so severe—including massive
prove to be miraculous. Even so, in a few instances, the
The newer physiologic approaches to therapy may
few months, and in many patients the ulcer also
week after the operation was performed. However,
gastric glands. This blocked almost all secretion of acid
most patients. Another therapy was to cut the two vagus
remove as much as four fifths of the stomach, thus
therapy were developed, it was often necessary to
In the past, before these approaches to peptic ulcer
receptors, thus
, an
of an acid-suppressant drug, especially
by two measures: (1) use of
changed immensely. Initial reports are that almost all
infectious basis for much peptic ulceration, therapy has
Physiology of Treatment.
down this barrier.
because it tends to break down the mucosal barrier; and
stimulation of the stomach secretory glands; (2)
, presumably because of increased nervous
any reason (for instance, even in psychic disturbances)
infection, studies in both animals and human beings
sometimes as much as twice normal. Although part of
peptic ulcer in the initial portion of the duodenum, the
the gastrointestinal wall, thus leading to peptic
that liquefy the barrier. As a result, the strong acidic
antibacterial therapy. Furthermore, the bacterium is
begins, it can last a lifetime unless it is eradicated by
Helicobacter pylori.
of the duodenal mucosa, infection most often caused by
troduodenal Mucosal Barrier.
two ways: (1) excess secretion of acid and pepsin by the
Therefore, a peptic ulcer can be caused in either of
bicarbonate, thus making still more sodium
promote rapid secretion of pancreatic juice. This
from the intestinal mucosa, which then
2. The presence of acid in the small intestine liberates
the rate of gastric emptying.
feedback from the duodenum, thereby decreasing
stomach, both by nervous reflexes and by hormonal
1. When excess acid enters the duodenum, it reflexly
plete, as follows:
Finally, two feedback control mechanisms normally
liver.
the large Brunner’s glands in the first few centimeters
ing digestion of the mucosa. In addition, large amounts
gastric juice, thus also inactivating pepsin and prevent-
, which contains large quantities of sodium
. Especially important is
Physiology of Gastrointestinal Disorders
Chapter 66
821
intestinal secretions
pancreatic
secretion
bicarbonate that neutralize the hydrochloric acid of the
of bicarbonate ions are provided in (1) the secretions of
of the duodenal wall and (2) in bile coming from the
ensure that this neutralization of gastric juices is com-
inhibits gastric secretion and peristalsis in the
secretin
passes by way of the blood to the pancreas to
juice also contains a high concentration of sodium
bicarbonate available for neutralization of the acid.
gastric mucosa or (2) diminished ability of the gastro-
duodenal mucosal barrier to protect against the diges-
tive properties of the stomach acid–pepsin secretion.
Specific Causes of Peptic Ulcer in
the Human Being
Bacterial Infection by Helicobacter pylori Breaks Down the Gas-
Many peptic ulcer patients
have been found to have chronic infection of the ter-
minal portions of the gastric mucosa and initial portions
the bacterium
Once this infection
capable of penetrating the mucosal barrier both by
virtue of its physical capability to burrow through the
barrier and by releasing bacterial digestive enzymes
digestive juices of the stomach secretions can then pen-
etrate into the underlying epithelium and literally digest
ulceration.
Other Causes of Ulceration.
In many people who have
rate of gastric acid secretion is greater than normal,
this increased secretion may be stimulated by bacterial
have shown that excess secretion of gastric juices for
may cause peptic ulceration.
Other factors that predispose to ulcers include (1)
smoking
alcohol,
(3) aspirin and other non-steroidal anti-inflammatory
drugs that also have a strong propensity for breaking
Since discovery of the bacterial
patients with peptic ulceration can be treated effectively
antibiotics along with other
agents to kill infectious bacteria and (2) administration
ranitidine
antihistaminic that blocks the stimulatory effect of his-
tamine on gastric gland histamine
2
reducing gastric acid secretion by 70 to 80 per cent.
reducing stomach acid–peptic juices enough to cure
nerves that supply parasympathetic stimulation to the
and pepsin and often cured the ulcer or ulcers within 1
much of the basal stomach secretion returned after a
returned.
bleeding from the ulcer—that heroic operative proce-
dures often must still be used.
Small Intestine
Small Intestine—Pancreatic Failure
A serious cause of abnormal digestion is failure of the
pancreas to secrete pancreatic juice into the small intes-
in pancreatitis
by a gallstone at the papilla
head of the pancreas has been
of the fat entering the small intestine may be unab-
fatty feces are excreted.
Pancreatitis.
Pancreatitis means inflammation of the
acute
pancreatitis or
drinking
excess alcohol
the main secretory duct from the pancreas as well as the
comes the trypsin inhibitor
quantity of trypsinogen becomes activated to form
more trypsinogen as well as chymotrypsinogen and car-
most of the proteolytic enzymes in the pancreatic ducts
the infectious agent toward the anus, and at the same
intestinal wall usually increases manyfold. As a result,
becomes greatly enhanced. In addition, motility of the
becomes extensively irritated, and its rate of secretion
Everywhere the infection is present, the mucosa
, the infection is most extensive
either by a virus or by bacteria in the intestinal tract. In
with important physiologic sequelae are the following.
through the large intestine. Several causes of diarrhea
ascending, transverse, and descending colons.
late proximal to this area, causing megacolon in the
this area of the large intestine. The sigmoid itself
of the sigmoid colon. As a consequence, neither defeca-
A frequent cause of megacolon is lack of or deficiency
Hirschsprung’s disease.
, or
3 to 4 inches. The condition is called
or sometimes only once a week. This allows tremendous
Occasionally, constipation is so severe that
rhea. After this, the cycle begins again, with repeated
mulated above a spastic sigmoid colon, excessive
causing serious constipation. After the constipation has
motility even normally is weak in the large intestine, so
segment of the sigmoid colon. It should be recalled that
much less likely.
intestine, the development of constipation in later life is
bowel habits early in life, usually defecating in the
For this reason, if a person establishes regular
atonic.
strong over months or years, and the colon becomes
tion, the reflexes themselves become progressively less
the natural defecation reflexes. Clinical experience
control defecation; this control is effected by inhibiting
Infants are seldom constipated, but part of their train-
tion of the normal defecation reflexes.
intestines, or ulcers, can cause constipation. A frequent
contents, such as tumors, adhesions that constrict the
late because of over-absorption of fluid. Any pathology
of dry, hard feces in the descending colon that accumu-
; it is often associated with large quantities
slow movement of feces through the
Large Intestine
Disorders of the
anemia of the pernicious anemia type, owing to dimin-
ulation caused by lack of vitamin K; and (4) macrocytic
because of lack of calcium); (3) inadequate blood coag-
body; (2) osteomalacia (demineralization of the bones
nutritional deficiency, often developing wasting of the
. As a result, the person suffers (1) severe
teins, carbohydrates, calcium, vitamin K, folic acid, and
In very severe cases of sprue, in addition to malab-
means simply excess fats in the stools.
, which
problem is one of absorption, not of digestion. In fact,
rather than undigested fat, demonstrating that the
of other digestive products. The fat that appears in the
In the early stages of sprue, intes-
unidentified infectious agents.
cific bacterium has been implicated as the cause, it is
treated with antibacterial agents. Even though no spe-
Tropical Sprue.
weeks, especially in children with this disease.
absorptive area of the gut. Removal of wheat and rye
disappear altogether, thus still further reducing the
severe forms, the villi themselves become blunted or
absorptive surface area as much as twofold. In the more
cytes on the villi are destroyed, thus decreasing the
the disease, only the microvilli of the absorbing entero-
tive effect on intestinal enterocytes. In milder forms of
in those who are susceptible, gluten has a direct destruc-
rye. Only some people are susceptible to this effect, but
present in certain types of grains, especially wheat and
, results from the toxic effects of
(in children), or
One type of sprue, called variously
” Mal-
sprue.
classified together under the general term “
decreased absorption by the mucosa; they are often
become well digested. Several diseases can cause
Occasionally, nutrients are not adequately absorbed
the pancreas to secrete digestive enzymes.
digest large portions of the pancreas itself, sometimes
and acini become activated. These enzymes rapidly
822
Unit XII
Gastrointestinal Physiology
completely and permanently destroying the ability of
Malabsorption by the Small
Intestinal Mucosa—Sprue
from the small intestine even though the food has
absorption also can occur when large portions of the
small intestine have been removed.
Nontropical Sprue.
idiopathic sprue, celiac disease
gluten
enteropathy
gluten
flour from the diet frequently results in cure within
A different type of sprue called tropical
sprue frequently occurs in the tropics and can often be
believed that this variety of sprue is usually caused by
inflammation of the intestinal mucosa resulting from
Malabsorption in Sprue.
tinal absorption of fat is more impaired than absorption
stools is almost entirely in the form of salts of fatty acids
the condition is frequently called steatorrhea
sorption of fats there is also impaired absorption of pro-
vitamin B
12
ished vitamin B
12
and folic acid absorption.
Constipation
Constipation means
large intestine
of the intestines that obstructs movement of intestinal
functional cause of constipation is irregular bowel
habits that have developed through a lifetime of inhibi-
ing in the early years of life requires that they learn to
shows that if one does not allow defecation to occur
when the defecation reflexes are excited or if one over-
uses laxatives to take the place of natural bowel func-
morning after breakfast when the gastrocolic and duo-
denocolic reflexes cause mass movements in the large
Constipation can also result from spasm of a small
that even a slight degree of spasm is often capable of
continued for several days and excess feces have accu-
colonic secretions often then lead to a day or so of diar-
bouts of alternating constipation and diarrhea.
Megacolon.
bowel movements occur only once every several days
quantities of fecal matter to accumulate in the colon,
causing the colon sometimes to distend to a diameter of
megacolon
of ganglion cells in the myenteric plexus in a segment
tion reflexes nor strong peristaltic motility can occur in
becomes small and almost spastic while feces accumu-
Diarrhea
Diarrhea results from rapid movement of fecal matter
Enteritis.
Enteritis means inflammation usually caused
usual infectious diarrhea
in the large intestine and the distal end of the ileum.
large quantities of fluid are made available for washing
time strong propulsive movements propel this fluid
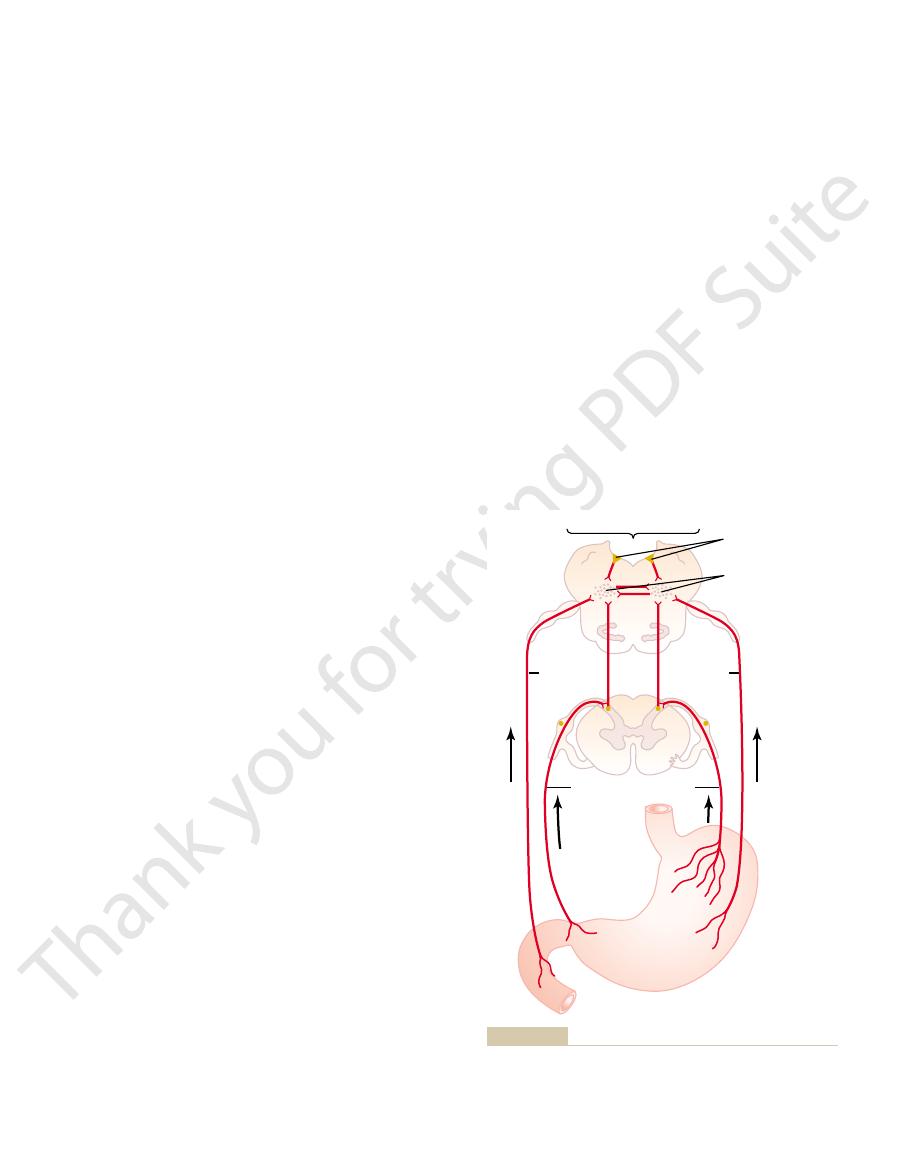
impulses are transmitted, as shown in Figure 66–2, by
upper portions of the small intestines. And the nerve
mainly from the pharynx, esophagus, stomach, and
The sensory signals that initiate vomiting originate
cially strong stimulus for vomiting.
overdistended, or even overexcitable. Excessive disten-
Vomiting is the means by which the upper gastroin-
Vomiting
Gastrointestinal Tract
General Disorders of the
bowel movements each day.
often cause adequate defecation. In this way, people
usually given in the morning shortly after a meal, can
occur, a small enema to excite action of this cord reflex,
injury. But, because the cord defecation reflex can still
loss of the voluntary aid to defecation—that is, loss of
cord reflex for defecation is still intact. Nevertheless,
the conus medullaris and the brain, the voluntary
When the spinal cord is injured somewhere between
sigmoid, rectum, and anus.
From Chapter 63 it will be recalled that defecation is
the colon. Even then the ulcers sometimes fail to heal,
gressed very far, the ulcers seldom will heal until an
tibility to ulcerative colitis. Once the condition has pro-
cause, there is a strong hereditary tendency for suscep-
bacterial infection not yet understood. Whatever the
destructive effect, but it also could result from chronic
The cause of ulcerative colitis is unknown. Some cli-
bowel movements.
enhanced. As a result, the patient has repeated diarrheal
30 minutes. Also, the colon’s secretions are greatly
mass movements
become inflamed and ulcerated. The motility of the
secretion of mucus in the distal colon. These two effects
emotional diarrhea, is caused by excessive
chogenic
to go into battle. This type of diarrhea, called
rhea that accompanies periods of nervous tension, such
therapy, as many as 50 per cent do.
antibiotics, almost no cholera patients die, but without
solutions. With proper therapy, along with the use of
as they are lost, mainly by giving the patient intravenous
The most important physiologic basis of therapy in
several days that death can ensue.
maximum of only 6 to 8 liters per day. Therefore, loss of
per day, although the colon can usually reabsorb a
ileum and colon. The amount can be 10 to 12 liters
colon bacilli). As explained in Chapter 65, cholera toxin
cholera
forward. This is an important mechanism for ridding the
Physiology of Gastrointestinal Disorders
Chapter 66
823
intestinal tract of a debilitating infection.
Of special interest is diarrhea caused by
(and
less often by other bacteria such as some pathogenic
directly stimulates excessive secretion of electrolytes
and fluid from the crypts of Lieberkühn in the distal
fluid and electrolytes can be so debilitating within
cholera is to replace the fluid and electrolytes as rapidly
Psychogenic Diarrhea.
Everyone is familiar with the diar-
as during examination time or when a soldier is about
psy-
stimulation of the parasympathetic nervous system,
which greatly excites both (1) motility and (2) excess
added together can cause marked diarrhea.
Ulcerative Colitis.
Ulcerative colitis is a disease in which
extensive areas of the walls of the large intestine
ulcerated colon is often so great that
occur much of the day rather than for the usual 10 to
nicians believe that it results from an allergic or immune
ileostomy is performed to allow the small intestinal con-
tents to drain to the exterior rather than to pass through
and the only solution might be surgical removal of the
entire colon.
Paralysis of Defecation in Spinal
Cord Injuries
normally initiated by accumulating feces in the rectum,
which causes a spinal cord–mediated defecation reflex
passing from the rectum to the conus medullaris of the
spinal cord and then back to the descending colon,
portion of the defecation act is blocked while the basic
the increased abdominal pressure and relaxation of the
voluntary anal sphincter—often makes defecation a dif-
ficult process in the person with this type of upper cord
with spinal cord injuries that do not destroy the conus
medullaris of the spinal cord can usually control their
testinal tract rids itself of its contents when almost any
part of the upper tract becomes excessively irritated,
tion or irritation of the duodenum provides an espe-
both vagal and sympathetic afferent nerve fibers to mul-
Chemoreceptor
trigger zone
“Vomiting center”
Vagal
afferents
Vagal
afferents
Apomorphine, morphine
Sympathetic afferents
extending into the spinal cord.
mainly in the medullary and pontile reticular formation but also
iting center includes multiple sensory, motor, and control nuclei
Neutral connections of the “vomiting center.” This so-called vom-
Figure 66–2
juices to flow backward into the stomach, and these
If the obstruction is beyond the stomach, antiperi-
contents occurs. This depresses bodily nutrition; it
after peptic ulceration, persistent vomiting of stomach
pylorus, which results often from fibrotic constriction
becomes obstructed. If the obstruction occurs at the
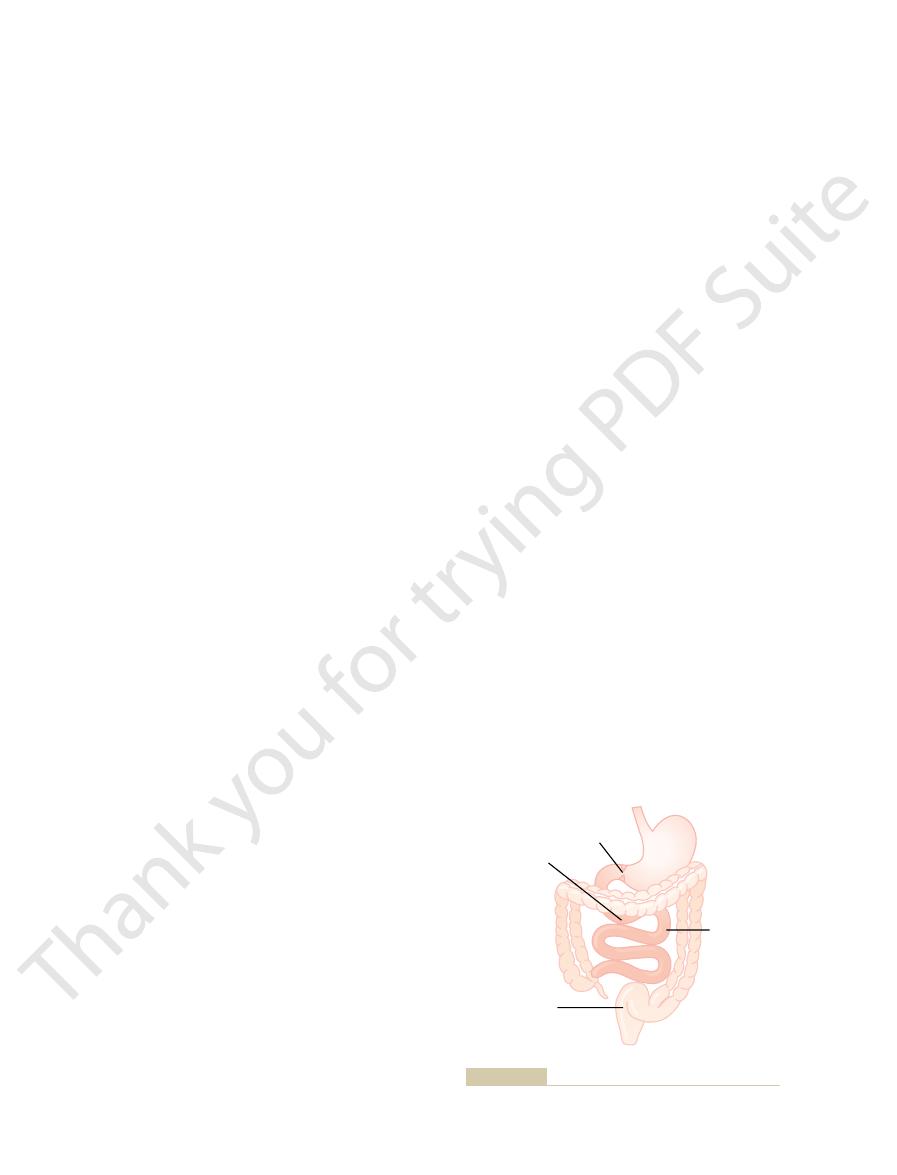
The abnormal consequences of obstruction de-
, and (4)
, (3)
, (2)
66–3. Some common causes of obstruction are (1)
almost any point along its course, as shown in Figure
The gastrointestinal tract can become obstructed at
Gastrointestinal Obstruction
without the prodromal sensation of nausea, indicating
cortex to initiate vomiting. Vomiting occasionally occurs
with motion sickness, or (3) impulses from the cerebral
of the vomiting center, and it can be caused by (1) irri-
knows that it is often a prodrome of vomiting. Nausea
vomiting.
, and finally to the
trigger zone
chemoreceptor
, then to the
labyrinth of the inner ear, and from here impulses are
ing: The motion stimulates receptors in the vestibular
people to vomit. The mechanism for this is the follow-
Also, it is well known that rapidly changing direction
irritative stimuli in the gastrointestinal tract itself.
vomiting. Destruction of this area blocks this type of
phine, and some digitalis derivatives, can directly
istration of certain drugs, including apomorphine, mor-
area can initiate vomiting; but, more important, admin-
trigger zone for vomiting.
chemoreceptor
nervous signals arising in areas of the brain. This is par-
testinal tract itself, vomiting can also be caused by
of Vomiting by Drugs or by Motion Sickness.
Chemoreceptor Trigger Zone” in the Brain Medulla for Initiation
Thus, the vomiting act results from a squeezing action
upward through the esophagus.
completely, allowing expulsion of the gastric contents
level. Finally, the lower esophageal sphincter relaxes
muscles, building the intragastric pressure to a high
traction of all the abdominal wall muscles. This squeezes
the posterior nares. Next comes a strong downward con-
into the lungs, and (4) lifting of the soft palate to close
open, (3) closing of the glottis to prevent vomitus flow
first effects are (1) a deep breath, (2) raising of the hyoid
ciently stimulated and the vomiting act instituted, the
Vomiting Act.
over and expels the vomitus to the exterior, as explained
the stomach into the esophagus. From here, a specific
sphincter, thus allowing vomitus to begin moving from
occur in both the duodenum and the stomach, along
At the onset of vomiting, strong intrinsic contractions
denum, become overly distended, this distention
portions of the gastrointestinal tract, especially the duo-
and stomach within 3 to 5 minutes. Then, as these upper
the intestine at a rate of 2 to 3 cm/sec; this process
ileum, and the antiperistaltic wave travels backward up
the digestive tract rather than downward. This
before vomiting appears. Antiperistalsis means peristal-
Antiperistalsis, the Prelude to Vomiting.
diaphragm and abdominal muscles.
the lower tract, and through spinal nerves to the
testinal tract, through vagal and sympathetic nerves to
9th, 10th, and 12th cranial nerves to the upper gastroin-
mitted from the vomiting center by way of the 5th, 7th,
together are called the “vomiting center.” From here,
824
Unit XII
Gastrointestinal Physiology
tiple distributed nuclei in the brain stem that all
motor impulses that cause the actual vomiting are trans-
In the early stages
of excessive gastrointestinal irritation or overdistention,
antiperistalsis begins to occur often many minutes
sis up
may begin as far down in the intestinal tract as the
can actually push a large share of the lower small intes-
tine contents all the way back to the duodenum
becomes the exciting factor that initiates the actual
vomiting act.
with partial relaxation of the esophageal-stomach
vomiting act involving the abdominal muscles takes
in the next paragraph.
Once the vomiting center has been suffi-
bone and larynx to pull the upper esophageal sphincter
traction of the diaphragm along with simultaneous con-
the stomach between the diaphragm and the abdominal
of the muscles of the abdomen associated with simulta-
neous contraction of the stomach wall and opening of
the esophageal sphincters so that the gastric contents
can be expelled.
“
Aside from the
vomiting initiated by irritative stimuli in the gastroin-
ticularly true for a small area located bilaterally on the
floor of the fourth ventricle called the
Electrical stimulation of this
stimulate this chemoreceptor trigger zone and initiate
vomiting but does not block vomiting resulting from
or rhythm of motion of the body can cause certain
transmitted mainly by way of the brain stem vestibular
nuclei into the cerebellum
vomiting center to cause
Nausea
Everyone has experienced the sensation of nausea and
is the conscious recognition of subconscious excitation
in an area of the medulla closely associated with or part
tative impulses coming from the gastrointestinal tract,
(2) impulses that originate in the lower brain associated
that only certain portions of the vomiting center are
associated with the sensation of nausea.
cancer
fibrotic constriction resulting from ulceration
or from peritoneal adhesions
spasm of a segment of
the gut
paralysis of a segment of the gut.
pend on the point in the gastrointestinal tract that
also causes excessive loss of hydrogen ions from the
stomach and can result in various degrees of whole-
body alkalosis.
staltic reflux from the small intestine causes intestinal
Causes
1. Cancer
2. Ulcer
3. Spasm
4. Paralytic ileus
5. Adhesions
High obstruction
causes extreme
vomiting
Obstruction at pylorus
causes acid vomitus
Obstruction below
duodenum causes
neutral or basic
vomitus
Low obstruction
causes extreme
constipation with
less vomiting
Obstruction in different parts of the gastrointestinal tract.
Figure 66–3
troenterol 17:943, 2003.
health and disease—sugars. Best Pract Res Clin Gas-
Wright EM, Martin MG, Turk E: Intestinal absorption in
drome. J Clin Gastroenterol 35(1 Suppl):S11, 2002.
Wood JD: Neuropathophysiology of irritable bowel syn-
Med 340(24):1888, 1999.
icity of nonsteroidal antiinflammatory drugs. N Engl J
Wolfe MM, Lichtenstein DR, Singh G: Gastrointestinal tox-
N Engl J Med 347(15):1175, 2002.
Helicobacter pylori
Suerbaum S, Michetti P:
prophylactic therapy. Clin Ther 26:197, 2004.
Spirt MJ: Stress-related mucosal disease: risk factors and
its variants: recent progress. Semin Pediatr Surg 13:18,
Puri P, Shinkai T: Pathogenesis of Hirschsprung’s disease and
347:417, 2002.
Podolsky DK: Inflammatory bowel disease. N Engl J Med
Tract. Baltimore: Williams and Wilkins, 1998.
Ming SC, Goldman H: Pathology of the Gastrointestinal
versies in surgery for IBD. Gastroenterology 126:1611,
Larson DW, Pemberton JH: Current concepts and contro-
inflammatory bowel disease. News Physiol Sci 16:272,
tion of intestinal mucosal immunity: implications in
Laroux FS, Pavlick KP, Wolf RE, Grisham MB: Dysregula-
Physiol Rev 82:245, 2002.
malian colon: mechanisms and implications for disease.
Kunzelmann K, Mall M: Electrolyte transport in the mam-
clinical perspective. J Clin Gastroenterol 36(5 Suppl):S29,
Kapadia CR: Gastric atrophy, metaplasia, and dysplasia: a
Mosby, 2001.
Johnson LR: Gastrointestinal Physiology, 6th ed. St. Louis:
287:G7, 2004
inflammation. Am J Physiol Gastrointest Liver Physiol
tal cancer in inflammatory bowel disease: the role of
Itzkowitz SH, Yio X: Inflammation and cancer. IV. Colorec-
targets in Crohn’s disease. N Engl J Med 346(8):614, 2002.
Elson CO: Genes, microbes, and T cells—new therapeutic
Crohn’s disease. Gastroenterology 126:1574, 2004.
Egan LJ, Sandborn WJ: Advances in the treatment of
Dig Dis 21:237, 2003.
and homocysteine. A review.
infection, vitamin B
pylori
Dierkes J, Ebert M, Malfertheiner P, Luley C:
biology and disease. J Clin Invest 113:321, 2004.
Helicobacter pylori
Blaser MJ, Atherton JC:
Gut 52:439, 2003.
tight junction barrier, ion transport, and inflammation.
epithelial responses to enteric pathogens: effects on the
Berkes J, Viswanathan VK, Savkovic SD, Hecht G: Intestinal
expelled through the lungs.
only about 0.6 liter. The remainder is normally absorbed
intestine each day averages 7 to 10 liters, whereas the
The amount of gases entering or forming in the large
sion of gas results from irritation of the large intestine,
for colonic bacteria. But in other instances, excess expul-
instance, beans contain an indigestible carbohydrate
unabsorbed fermentable types of carbohydrates. For
suitable medium for gas-forming bacteria, especially
such as vinegar. Some of these foods serve as a
onion, cauliflower, corn, and certain irritant foods
of flatus through the anus than others—beans, cabbage,
explosive mixture is sometimes formed. Use of the elec-
hydrogen become suitably mixed with oxygen, an actual
When methane and
, and
dioxide
from bacterial action, including especially
In the large intestine, most of the gases are derived
amounts of gas normally occur in the small intestine,
person these gases are expelled by belching. Only small
oxygen derived from swallowed air. In the typical
in the gut as a result of bacterial action, or (3) gases that
from three sources: (1) swallowed air, (2) gases formed
, can enter the gastrointestinal tract
Gases, called
Tract; “Flatus”
Gases in the Gastrointestinal
resulting from the severe vomiting.
severe vomiting does then occur. Prolonged obstruction
move from the small intestine into the large intestine,
stipation, but at first vomiting is not severe. After the
or more. The patient develops an intense feeling of con-
intestine, feces can accumulate in the colon for a week
equal, so that little change in acid-base balance occurs.
dehydrated, but the loss of acid from the stomach and
and electrolytes, so that he or she becomes severely
this instance, the person loses large amounts of water
juices are vomited along with the stomach secretions. In
Physiology of Gastrointestinal Disorders
Chapter 66
825
base from the small intestine may be approximately
If the obstruction is near the distal end of the large
large intestine has become completely filled and it
finally becomes impossible for additional chyme to
of the large intestine can finally causes rupture of the
intestine itself or dehydration and circulatory shock
flatus
diffuse from the blood into the gastrointestinal tract.
Most gases in the stomach are mixtures of nitrogen and
and much of this gas is air that passes from the stomach
into the intestinal tract.
carbon
, methane
hydrogen.
tric cautery during sigmoidoscopy has been known to
cause a mild explosion.
Certain foods are known to cause greater expulsion
that passes into the colon and becomes a superior food
which promotes rapid peristaltic expulsion of gases
through the anus before they can be absorbed.
average amount expelled through the anus is usually
into the blood through the intestinal mucosa and
References
persistence:
Helicobacter
12
2003
2001.
2004.
2004.
infection.