
lowing discussions.
very different when the person is breathing pure oxygen, as we see in the fol-
of acclimatized people can barely survive when breathing air. But the effect is
oxygen pressure in the alveoli. At the summit of Mount Everest, only the best
oxygen is continually being absorbed into the blood, leaving about 35 mm Hg
in the alveoli would be 40 mm Hg. However, some of this remaining alveolar
199 mm Hg would be oxygen and four fifths would be nitrogen; that is, the P
only 199 mm Hg. If there were no use of oxygen by the body, one fifth of this
person, 7 mm of the 206 mm Hg must be carbon dioxide, leaving
acclimatized
this must be water vapor, leaving only 206 mm Hg for all the other gases. In the
at the top of 29,028–foot Mount Everest. Forty-seven millimeters of mercury of
sea-level value of 760 mm Hg to 253 mm Hg, which is the usual measured value
oxygen. For instance, assume that the barometric pressure falls from the normal
falls to about 7 mm Hg because of increased respiration.
person, who increases his or her ventilation about fivefold, the P
acclimatized
falls from the sea-level value of 40 mm Hg to lower values. In the
In the case of carbon dioxide, during exposure to very high altitudes, the alve-
the body temperature is normal, regardless of altitude.
centration. Water vapor pressure in the alveoli remains 47 mm Hg as long as
These two gases dilute the oxygen in the alveoli, thus reducing the oxygen con-
alveoli. Also, water vaporizes into the inspired air from the respiratory surfaces.
Even at high altitudes,
Carbon Dioxide and Water Vapor Decrease the Alveolar Oxygen.
at Different Elevations
18 mm Hg.
at sea level about 159 mm Hg, but at 50,000 feet only
proportionately, remaining at all times slightly less than 21 per cent of the total
metric pressure decreases, the atmospheric oxygen partial pressure decreases
of all the hypoxia problems in high-altitude physiology because, as the baro-
50,000 feet, 87 mm Hg. This decrease in barometric pressure is the basic cause
barometric pressure is 760 mm Hg; at 10,000 feet, only 523 mm Hg; and at
at different altitudes, showing that at sea level, the
oxygen pressures
Table 43–1 gives the approximate
Effects of Low Oxygen Pressure on the Body
body. This chapter deals with these problems.
forces, weightlessness, and so forth) on the human
in aviation, mountain climbing, and space vehicles,
Aviation, High-Altitude,
C
H
A
P
T
E
R
4
3
537
and Space Physiology
As we have ascended to higher and higher altitudes
it has become progressively more important to
understand the effects of altitude and low gas pres-
sures (as well as several other factors—acceleratory
Barometric Pressures at Different Altitudes.
baro-
metric and
barometric pressure—Po
2
Alveolar P
O
2
carbon dioxide is continually excreted from the pulmonary blood into the
olar Pco
2
co
2
Now let us see how the pressures of these two gases affect the alveolar
o
2
unacclimatized person breathing air, beginning at an
Acute Effects of Hypoxia
operates perfectly.
47,000 feet, provided the oxygen-supplying equipment
23,000 feet and when breathing pure oxygen is about
feet when one is breathing air. In addition, because an
air. For instance, the arterial saturation at 47,000 feet
tion curves in Figure 43–1, one notes that an aviator
Unpressurized Airplane
and When Breathing Oxygen in an
The “Ceiling” When Breathing Air
ascends to about 39,000 feet; then it falls rapidly to
when one is breathing pure oxygen. Note that the sat-
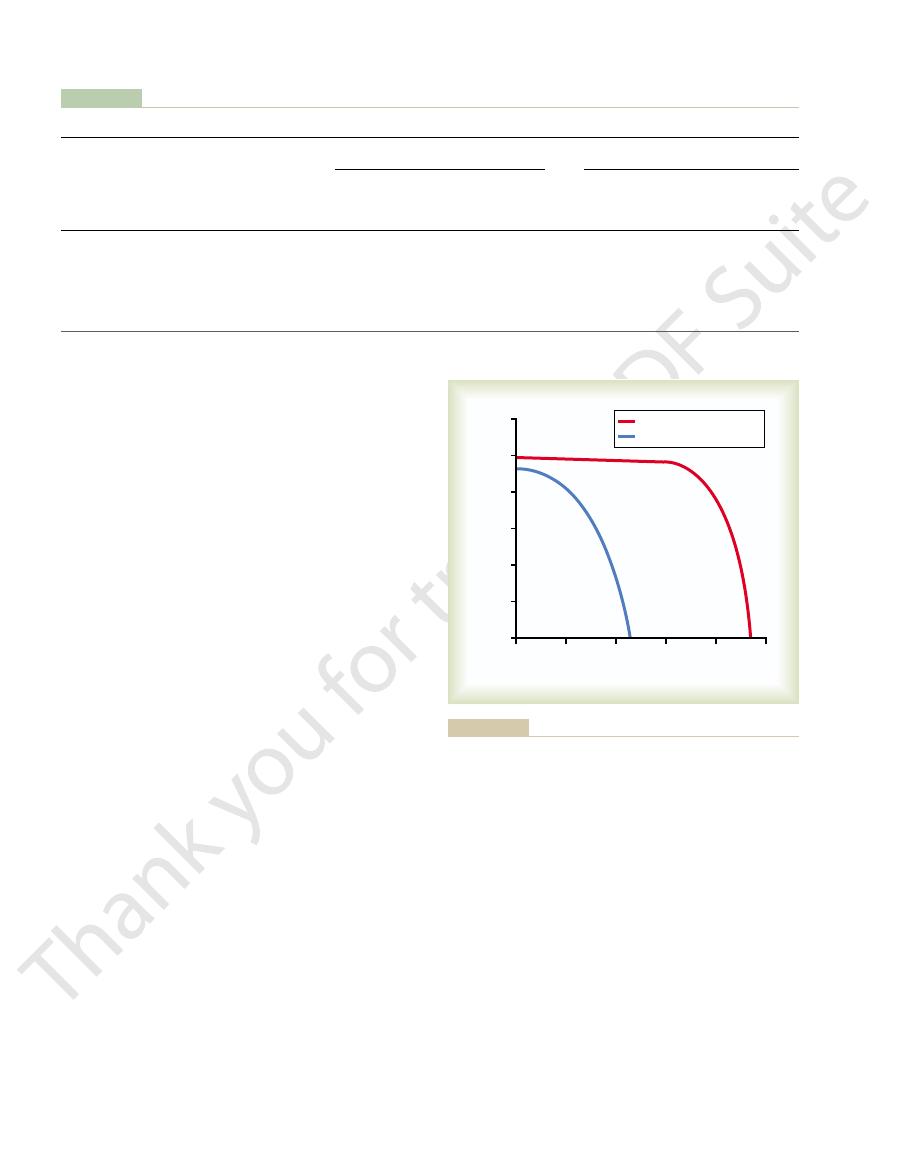
The red curve of Figure 43–1 shows arterial blood
air (see Table 43–1).
139 mm Hg instead of the 18 mm Hg when breathing
as high as
nitrogen becomes occupied by oxygen. At 30,000 feet,
When a person breathes pure oxygen instead of air,
at Different Altitudes
Effect of Breathing Pure Oxygen on
and much less at still higher altitudes.
falls rapidly, as shown by the blue curve of the figure,
cent. Above 10,000 feet, the arterial oxygen saturation
10,000 feet, even when air is breathed, the arterial
while breathing oxygen. Up to an altitude of about
Figure 43–1 shows arterial blood oxygen saturation at
than in the unacclimatized person, as we discuss later.
person but only to 53 mm Hg in the acclimatized. The
tude, it falls to about 40 mm Hg in the unacclimatized
is 104 mm Hg; at 20,000 feet alti-
level, the alveolar P
person. At sea
acclimatized
unacclimatized
Table 43–1 shows the approximate P
The fifth column of
Aviation, Space, and Deep-Sea Diving Physiology
538
Unit VIII
Alveolar P
O
2
at Different Altitudes.
o
2
s in the alveoli
at different altitudes when one is breathing air for both
the
and the
o
2
difference between these two is that alveolar ventila-
tion increases much more in the acclimatized person
Saturation of Hemoglobin with Oxygen at Different Altitudes.
different altitudes while a person is breathing air and
oxygen saturation remains at least as high as 90 per
until it is slightly less than 70 per cent at 20,000 feet
Alveolar P
O
2
most of the space in the alveoli formerly occupied by
an aviator could have an alveolar Po
2
hemoglobin oxygen saturation at different altitudes
uration remains above 90 per cent until the aviator
about 50 per cent at about 47,000 feet.
Comparing the two arterial blood oxygen satura-
breathing pure oxygen in an unpressurized airplane
can ascend to far higher altitudes than one breathing
when one is breathing oxygen is about 50 per cent and
is equivalent to the arterial oxygen saturation at 23,000
unacclimatized person usually can remain conscious
until the arterial oxygen saturation falls to 50 per cent,
for short exposure times the ceiling for an aviator in
an unpressurized airplane when breathing air is about
Some of the important acute effects of hypoxia in the
Table 43–1
Effects of Acute Exposure to Low Atmospheric Pressures on Alveolar Gas Concentrations and Arterial Oxygen Saturation*
Alveoli
Alveoli
Saturation
Alveoli
Alveoli
Saturation
Pressure
Air
in
Oxygen
in
P
in
Oxygen
P
in
P
Barometric
P
Arterial
Arterial
Breathing Air
Breathing Pure Oxygen
O
2
in
P
CO
2
O
2
CO
2
O
2
50,000
87
18
24
16
15
40,000
141
29
36
58
84
30,000
226
47
24 (7)
18 (30)
24 (38)
40
139
99
20,000
349
73
24 (10)
40 (53)
73 (85)
40
262
100
10,000
523
110
36 (23)
67 (77)
90 (92)
40
436
100
0
760
159
40 (40)
104 (104)
97 (97)
40
673
100
(mm Hg)
(mm Hg)
(%)
(mm Hg)
(mm Hg)
(%)
Altitude (ft)
(mm Hg)
(mm Hg)
* Numbers in parentheses are acclimatized values.
0
10
20
30
40
50
Altitude (thousands of feet)
Arterial oxygen saturation (per cent)
50
60
70
80
90
100
Breathing pure oxygen
Breathing air
ing air and when breathing pure oxygen.
Effect of high altitude on arterial oxygen saturation when breath-
Figure 43–1
). This occurs
in the nonpulmonary tissues, which is called
growth of
, so that the amount
over a period of weeks
The cardiac output
tion—Increased Tissue Capillarity.
Peripheral Circulatory System Changes During Acclimatiza-
conditions.
of the lungs, which are poorly perfused under usual
increase in pulmonary arterial blood pressure; this
interface still more. A final part results from an
expands the surface area of the alveolar-capillary
results from an increase in lung air volume, which
which oxygen can diffuse into the blood. Another part
monary capillary blood volume, which expands the
altitude.
increase as much as threefold during exercise. A
21 ml/mm Hg/min, and this diffusing capacity can
by 20 to 30 per cent, and this increase times the
In addition, the blood volume also increases, often
of 40 to 45 to an average of about 60, with an average
a time, the hematocrit rises slowly from a normal value
increase in red blood cell production. Ordinarily, when
Increase in Red Blood Cells and Hemoglobin Concentration
for the alkalosis.
tion. Thus, the respiratory centers are much more
bicarbonate excretion. This metabolic compensation
Chapter 30. The kidneys respond to decreased P
kidneys for the respiratory alkalosis, as discussed in
activity of the center.
center, thus increasing the respiratory stimulatory
This in turn decreases the pH in the fluids surround-
the cerebrospinal fluid as well as in the brain tissues.
The cause of this fading inhibition is believed to be
ceptor stimulus from hypoxia, and ventilation in-
inhibition fades away, allowing the respiratory center
. But during the ensuing 2 to 5 days, this
peripheral arterial chemoreceptors in the carotid and
to stimulate respiration by way of the
of low P
pH of the body fluids. These changes
carbon dioxide, reducing the P
The immediate increase in pulmonary ventilation on
chemoreceptors increase ventilation still more, up to
remains at very high altitude for several days, the
without the increased ventilation. Then, if the person
high altitude, and it alone allows the person to rise
Therefore, compensation occurs within seconds for the
arterial chemoreceptors, and this increases alveolar
Increased Pulmonary Ventilation—Role of Arterial Chemore-
vascularity of the peripheral tissues, and (5) increased
increased diffusing capacity of the lungs, (4) increased
tion, (2) increased numbers of red blood cells, (3)
The principal means by which acclimatization comes
still higher altitudes.
the body. And it becomes possible for the person to
, so that it causes fewer deleterious effects on
acclimatized
A person remaining at high altitudes for days, weeks,
Acclimatization to Low P
narily falls to about 50 per cent of normal, and after
stays at 15,000 feet for 1 hour, mental proficiency ordi-
movements. For instance, if an unacclimatized aviator
ment, memory, and performance of discrete motor
decreased mental proficiency, which decreases judg-
matized person, in coma, followed shortly thereafter
18,000 feet and end, above 23,000 feet in the unaccli-
sionally nausea, and sometimes euphoria.These effects
mental and muscle fatigue, sometimes headache, occa-
altitude of about 12,000 feet, are drowsiness, lassitude,
Aviation, High-Altitude, and Space Physiology
Chapter 43
539
progress to a stage of twitchings or seizures above
by death.
One of the most important effects of hypoxia is
18 hours at this level it falls to about 20 per cent of
normal.
O
2
or years becomes more and more
to the
low Po
2
work harder without hypoxic effects or to ascend to
about are (1) a great increase in pulmonary ventila-
ability of the tissue cells to use oxygen despite low Po
2
.
ceptors.
Immediate exposure to low Po
2
stimulates the
ventilation to a maximum of about 1.65 times normal.
several thousand feet higher than would be possible
about five times normal.
rising to a high altitude blows off large quantities of
co
2
and increasing the
inhibit the brain
stem respiratory center and thereby oppose the effect
O
2
aortic bodies
to respond with full force to the peripheral chemore-
creases to about five times normal.
mainly a reduction of bicarbonate ion concentration in
ing the chemosensitive neurons of the respiratory
An important mechanism for the gradual decrease
in bicarbonate concentration is compensation by the
co
2
by reducing hydrogen ion secretion and increasing
for the respiratory alkalosis gradually reduces plasma
and cerebrospinal fluid bicarbonate concentration and
pH toward normal and removes part of the inhibitory
effect on respiration of low hydrogen ion concentra-
responsive to the peripheral chemoreceptor stimulus
caused by the hypoxia after the kidneys compensate
During Acclimatization.
As discussed in Chapter 32,
hypoxia is the principal stimulus for causing an
a person remains exposed to low oxygen for weeks at
increase in whole blood hemoglobin concentration
from normal of 15 g/dl to about 20 g/dl.
increased blood hemoglobin concentration gives an
increase in total body hemoglobin of 50 or more per
cent.
Increased Diffusing Capacity After Acclimatization.
It will
be recalled that the normal diffusing capacity for
oxygen through the pulmonary membrane is about
similar increase in diffusing capacity occurs at high
Part of the increase results from increased pul-
capillaries and increases the surface area through
forces blood into greater numbers of alveolar capil-
laries than normally—especially in the upper parts
often increases as much as 30 per cent immediately
after a person ascends to high altitude but then
decreases back toward normal
as the blood hematocrit increases
of oxygen transported to the peripheral body tissues
remains about normal.
Another circulatory adaptation is
increased numbers of systemic circulatory capillaries
in-
creased tissue capillarity (or angiogenesis
in increasing work capacity, consider this: The work
To give an idea of the importance of acclimatization
uptake that the body can achieve.
In general, work capacity is reduced in direct pro-
not only skeletal muscles but also cardiac muscles.
muscles is greatly decreased in hypoxia. This includes
hypoxia, as discussed earlier, the work capacity of all
High Altitudes and Positive Effect
Reduced Work Capacity at
high-altitude natives.
, indicating that oxygen transport to the tissues is
for the lowlanders, despite the very low arterial
altitude natives is only 15 mm Hg less than the venous
altitude. Note also that the venous P
in the natives at high altitude is only 40 mm Hg,
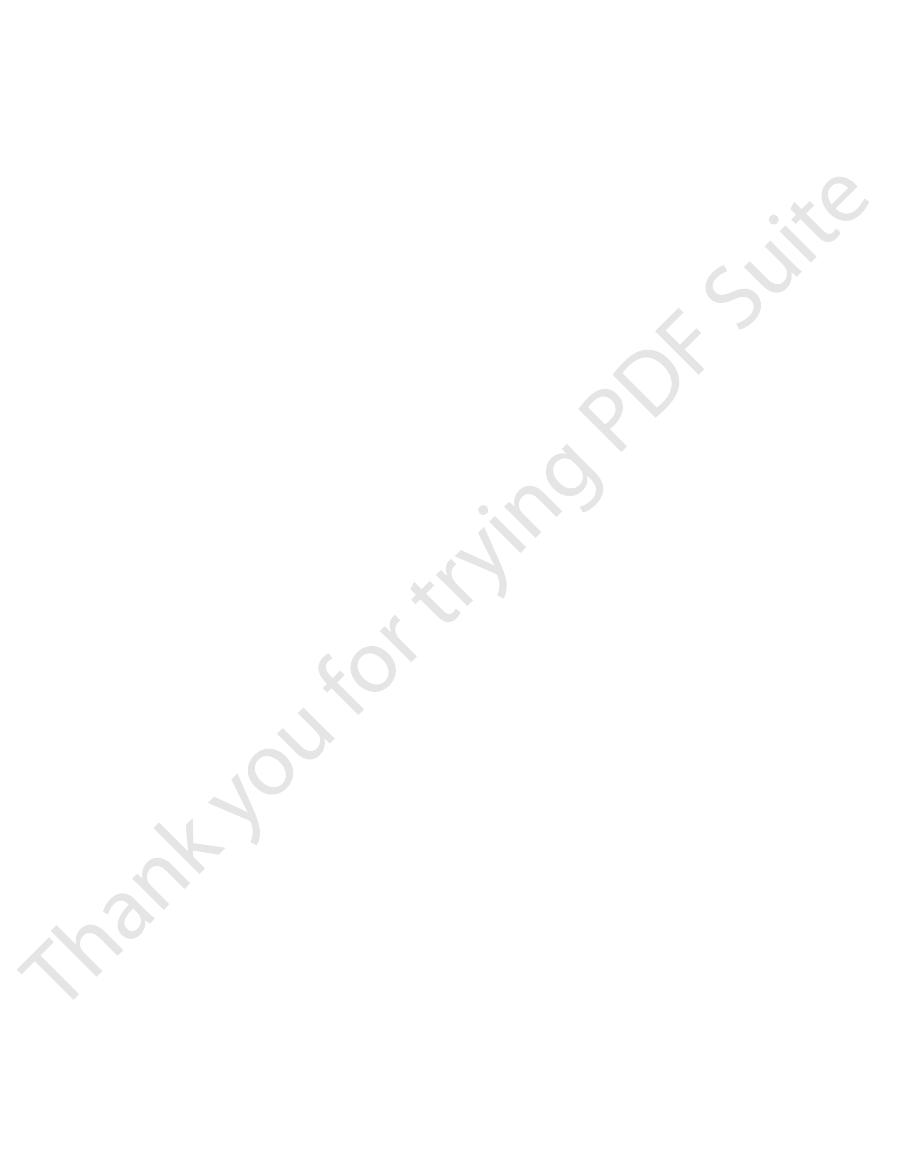
who live at 15,000 feet. Note that the arterial oxygen
highly facilitated in these natives. For instance, Figure
than the hearts of lowlanders.
amounts of cardiac output, are considerably larger
their hearts, which from birth onward pump extra
ratio of ventilatory capacity to body mass. In addition,
the body size is somewhat decreased, giving a high
The chest size, especially, is greatly increased, whereas
years. Acclimatization of the natives begins in infancy.
acclimatized lowlanders, even though the lowlanders
tization, the natives are superior to even the best-
and live there all their lives. In all aspects of acclima-
feet. Many of these natives are born at these altitudes
group in the Peruvian Andes lives at an altitude of
Many native human beings in the Andes and in the
at High Altitudes
of Native Human Beings Living
Natural Acclimatization
than can their sea-level counterparts.
than in sea-level inhabitants. Therefore, it is presumed
13,000 to 17,000 feet, cell mitochondria and cellular
caused by pulmonary hypertension at high altitude.
instance, capillary density in right ventricular muscle
increase in capillarity is especially marked. For
In active tissues exposed to chronic hypoxia, the
to high altitude.
Aviation, Space, and Deep-Sea Diving Physiology
540
Unit VIII
especially in animals born and bred at high altitudes
but less so in animals that later in life become exposed
increases markedly because of the combined effects
of hypoxia and excess workload on the right ventricle
Cellular Acclimatization.
In animals native to altitudes of
oxidative enzyme systems are slightly more plentiful
that the tissue cells of high altitude–acclimatized
human beings also can use oxygen more effectively
Himalayas live at altitudes above 13,000 feet—one
17,500 feet and works a mine at an altitude of 19,000
might also have lived at high altitudes for 10 or more
Delivery of oxygen by the blood to the tissues is also
43–2 shows oxygen-hemoglobin dissociation curves for
natives who live at sea level and for their counterparts
Po
2
but because of the greater quantity of hemoglobin,
the quantity of oxygen in their arterial blood is greater
than that in the blood of the natives at the lower
o
2
in the high-
Po
2
Po
2
exceedingly effective in the naturally acclimatized
of Acclimatization
In addition to the mental depression caused by
portion to the decrease in maximum rate of oxygen
capacities as per cent of normal for unacclimatized and
acclimatized people at an altitude of 17,000 feet are as
follows:
Acclimatized for 2 months
68
Work capacity
(per cent of normal)
Unacclimatized 50
Native living at 13,200 feet but working at
almost equal to that of a lowlander at sea level, but
Thus, naturally acclimatized native persons can
17,000 feet
87
achieve a daily work output even at high altitude
even well-acclimatized lowlanders can almost never
achieve this result.
Acute Mountain Sickness and
High-Altitude Pulmonary Edema
A small percentage of people who ascend rapidly to
high altitudes become acutely sick and can die if not
(Venous values)
0
20
40
60
80
100 120 140
Pressure of oxygen in blood (P
O
2
) (mm Hg)
Quantity of oxygen in blood (vol %)
0
2
4
6
8
10
12
14
16
18
20
22
24
26
28
Sea-level dwellers
Mountain dwellers
(15,000 ft)
(Arterial values)
X
X
X
X
level residents. PAHO Scientific Publication No. 140, Life at High
contents as recorded in their native surroundings. (Data from
showing the respective arterial and venous P
) and sea-level residents (
red curve
residents (
Figure 43–2
Oxygen-hemoglobin dissociation curves for blood of high-altitude
blue curve),
O
2
levels and oxygen
Oxygen-dissociation curves for bloods of high-altitude and sea-
Altitudes, 1966.)
the lower vessels. Because the heart cannot pump
pressure in the vessels of the lower body increases,
tion, the pressure becomes nearly 300 mm Hg. And, as
increased (to about 450 mm Hg). In the sitting posi-
5 G and
Thus, if the centrifugal acceleratory force is
centrifuged toward the lowermost part of the body.
positive G,
When an aviator is subjected to
translocated by centrifugal forces.
latory system, because blood is mobile and can be
The most impor-
Effects of Centrifugal Acceleratory Force on the Body—
1 G.
down by his belt is equal to the weight of his body, the
applied to his body; if the force with which he is held
negative G
5 G.
pull-out from a dive, the force acting on the seat is
of gravity. If the force with which he presses against
1 G because it is equal to the pull
gravity and is equal to his weight. The intensity of this
aviator is simply sitting in his seat, the force with which
When an
Measurement of Acceleratory Force—“G.”
. It is also obvious that the force
obvious that as the velocity increases, the
of curvature of the turn. From this formula, it is
is velocity of travel, and
is centrifugal acceleratory force,
When an airplane makes a turn, the force of cen-
Centrifugal Acceleratory Forces
vehicle turns, centrifugal acceleration.
at the end of flight, deceleration; and every time the
beginning of flight, simple linear acceleration occurs;
acceleratory forces affect the body during flight. At the
motion in airplanes or spacecraft, several types of
on the Body in Aviation and
Effects of Acceleratory Forces
a lower altitude.
further compounds the problem. Most of these people
blood flow where the blood is poorly oxygenated; this
vessels, thus causing an excess of pulmonary shunt
fails. Third, the alveolar arteriolar spasm diverts much
sure rises excessively, and the right side of the heart
oles become constricted, the pulmonary arterial pres-
alveoli are now in the low-oxygen state, all the arteri-
alveoli, as explained in Chapter 38. But because
of the lung hypoxia. This results from the hypoxic
oxygen delivery also begins to decrease. Second, the
the blood viscosity increases severalfold; this increased
threefold: First, the red cell mass becomes so great that
The causes of this sequence of events are probably
altitude.
fall, (5) congestive heart failure ensues, and (6) death
enlarged, (4) the peripheral arterial pressure begins to
tization, (3) the right side of the heart becomes greatly
hematocrit become exceptionally high, (2) the pul-
the following effects occur: (1) the red cell mass and
, in which
chronic mountain sickness
Occasionally, a person who remains at high altitude
within hours.
dysfunction that can be lethal. Allowing the person
occurs. Extension of the process to progressively
unconstricted pulmonary vessels. The postulated
parts, so that more and more of the pulmonary
to constrict potently, but the constriction is much
The severe hypoxia causes the pulmonary arterioles
unknown, but a suggested answer is the following:
. The cause of this is still
The cerebral edema can then lead to severe
causes fluid to leak into the cerebral tissues.
thus increasing capillary pressure, which in turn
arterioles increases blood flow into the capillaries,
vessels, caused by the hypoxia. Dilation of the
. This is believed to result
ascent. Two events frequently occur:
given oxygen or removed to a low altitude. The sick-
Aviation, High-Altitude, and Space Physiology
Chapter 43
541
ness begins from a few hours up to about 2 days after
1. Acute cerebral edema
from local vasodilation of the cerebral blood
disorientation and other effects related to cerebral
dysfunction.
2. Acute pulmonary edema
greater in some parts of the lungs than in other
blood flow is forced through fewer and fewer still
result is that the capillary pressure in these areas of
the lungs becomes especially high and local edema
more areas of the lungs leads to spreading
pulmonary edema and severe pulmonary
to breathe oxygen usually reverses the process
Chronic Mountain Sickness
too long develops
monary arterial pressure becomes elevated even more
than the normal elevation that occurs during acclima-
often follows unless the person is removed to a lower
viscosity tends to decrease tissue blood flow so that
pulmonary arterioles become vasoconstricted because
vascular constrictor effect that normally operates to
divert blood flow from low-oxygen to high-oxygen
all the
of the blood flow through nonalveolar pulmonary
recover within days or weeks when they are moved to
Space Physiology
Because of rapid changes in velocity and direction of
trifugal acceleration is determined by the following
relation:
in which f
m is the
mass of the object, v
r is radius
force of
centrifugal acceleration increases in proportion to the
square of the velocity
of acceleration is directly proportional to the sharpness
of the turn (the less the radius).
he is pressing against the seat results from the pull of
force is said to be
+
the seat becomes five times his normal weight during
+
If the airplane goes through an outside loop so that
the person is held down by his seat belt,
is
negative force is
-
(Positive G)
Effects on the Circulatory System.
tant effect of centrifugal acceleration is on the circu-
blood is
+
the person is in an immobilized standing position,
the pressure in the veins of the feet becomes greatly
these vessels passively dilate so that a major portion
of the blood from the upper body is translocated into
f
mv
r
=
2
used by astronauts.
Therefore, we see the reason for the reclining seats
continue for as long as several minutes at a time.
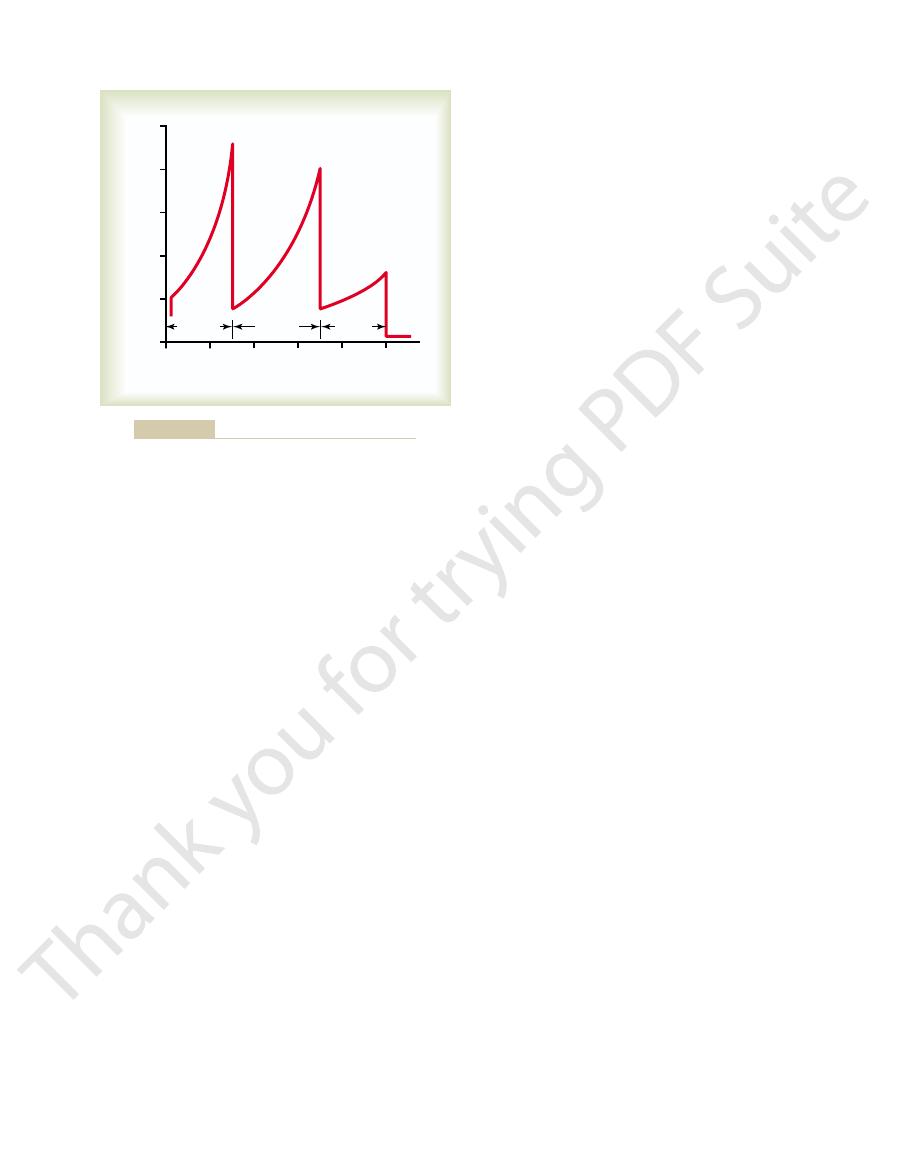
, this amount of acceleration can be withstood
could not withstand this much acceleration, but in a
high as 8 G. In the standing position, the human body
eration as high as 9 G, and the second-stage booster as
Figure 43
negative.
, one positive and the other
tion can be tremendous; both of these are types
However, blast-off acceleration and landing decelera-
when the spacecraft goes into abnormal gyrations.
spacecraft cannot make rapid turns; therefore, cen-
Unlike an airplane, a
Acceleratory Forces in Space Travel.
Effects of Linear Acceleratory Forces
certainly would still be less than 10 G.
this procedure were used, the limit of safety almost
tions despite submersion in water. Therefore, even if
tissues, and diaphragm into seriously abnormal posi-
the lungs still allows displacement of the heart, lung
acting in the body. However, the presence of air in
retically, a pilot submerged in a tank or suit of water
ating compression bags as the G increases. Theo-
in the lower abdomen and legs. The simplest of these
by delaying the onset of blackout. Also, special
vessels of the abdomen can be prevented, there-
abdomen, some of the pooling of blood in the large
collapse that might occur during positive G. First, if
Protection of the Body Against Centrifugal Acceleratory
tive G. As a result, the eyes often become temporarily
brain to prevent intracerebral vascular rupture.
that blood is centrifuged toward the cranial vessels,
expected for the following reason: The cerebrospinal
cranium show less tendency for rupture than would be
brain to rupture. However, the vessels inside the
sure reaches 300 to 400 mm Hg, sometimes causing
20 G, for instance) and centrifugation of the blood
Occasionally, negative G forces can be so great
hyperemia of the head. Occasionally, psychotic distur-
nent harm, although causing intense momentary
manently than the effects of positive G. An aviator can
The effects of negative G on the body are
before vertebral fracture occurs is about 20 G.
vertebrae. The degree of positive acceleration that the
Effects on the Vertebrae.
acceleration is continued, the person will die.
ness shortly thereafter. If this great degree of
exes.
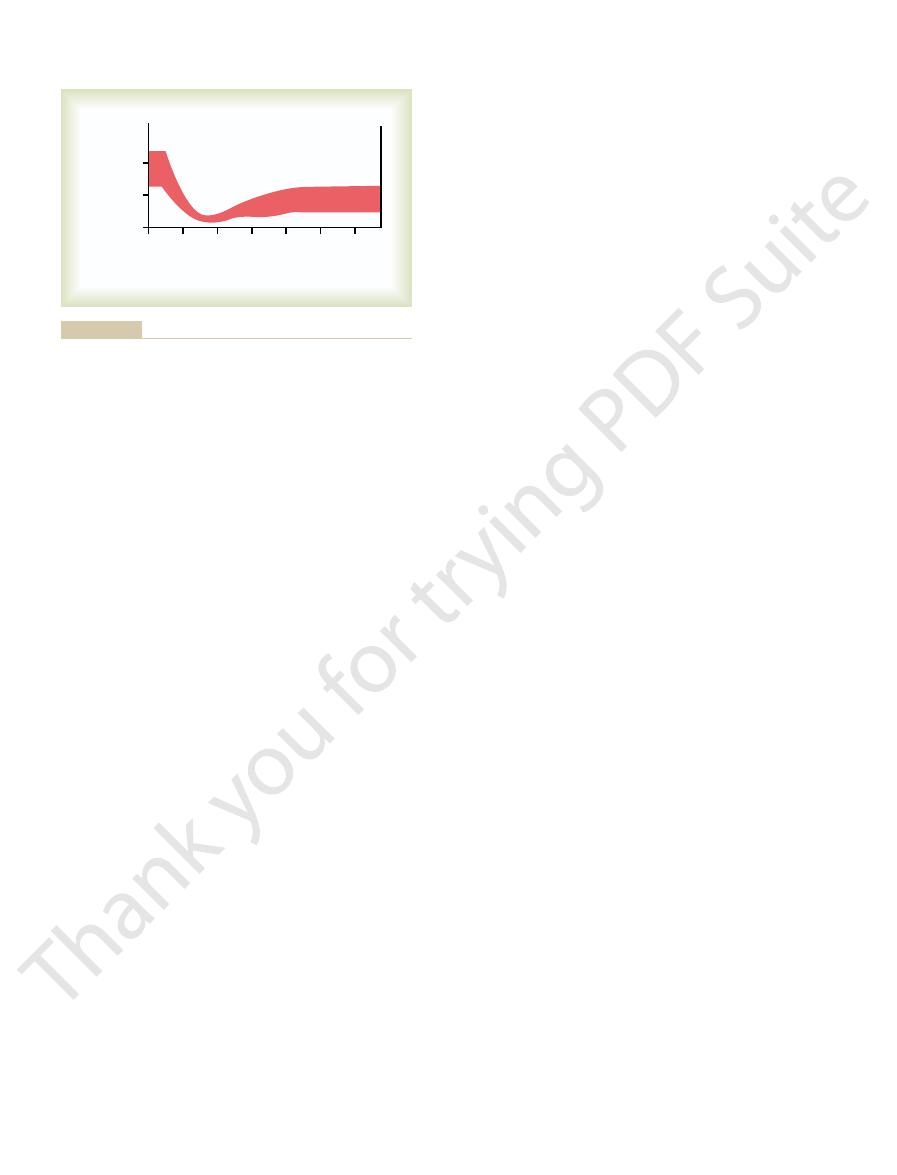
20 mm Hg within another 10 to 15 seconds. This sec-
sure of about 55 mm Hg and a diastolic pressure of
below 22 mm Hg for the
sitting person. Note that both these pressures fall
3.3 G is suddenly applied to a
diastolic arterial pressures (top and bottom curves,
Figure 43
in this way in the lower body, the less
unless blood returns to it, the greater the quantity of
Aviation, Space, and Deep-Sea Diving Physiology
542
Unit VIII
blood “pooled”
that is available for the cardiac output.
–3 shows the changes in systolic and
respectively) in the upper body when a centrifugal
acceleratory force of
+
first few seconds after the
acceleration begins but then return to a systolic pres-
ondary recovery is caused mainly by activation of the
baroreceptor refl
Acceleration greater than 4 to 6 G causes “black-
out” of vision within a few seconds and unconscious-
Extremely high acceleratory
forces for even a fraction of a second can fracture the
average person can withstand in the sitting position
Negative G.
less dramatic acutely but possibly more damaging per-
usually go through outside loops up to negative accel-
eratory forces of
-4 to -5 G without causing perma-
bances lasting for 15 to 20 minutes occur as a result of
brain edema.
(
-
into the head is so great that the cerebral blood pres-
small vessels on the surface of the head and in the
fluid is centrifuged toward the head at the same time
and the greatly increased pressure of the cerebrospinal
fluid acts as a cushioning buffer on the outside of the
Because the eyes are not protected by the cranium,
intense hyperemia occurs in them during strong nega-
blinded with “red-out.”
Forces.
Specific procedures and apparatus have been
developed to protect aviators against the circulatory
the aviator tightens his or her abdominal muscles to
an extreme degree and leans forward to compress the
“anti-
G” suits have been devised to prevent pooling of blood
applies positive pressure to the legs and abdomen by
infl
might experience little effect of G forces on the circu-
lation because the pressures developed in the water
pressing on the outside of the body during centrifugal
acceleration would almost exactly balance the forces
on the Body
trifugal acceleration is of little importance except
of linear acceleration
–4 shows an approximate profile of accel-
eration during blast-off in a three-stage spacecraft,
demonstrating that the first-stage booster causes accel-
semireclining position transverse to the axis of acceler-
ation
with ease despite the fact that the acceleratory forces
0
5
10
15
20
25
30
Time from start of G to symptoms
(sec)
Arterial pressure
(mm Hg)
0
50
100
tolerance to positive acceleration. J Aviation Med 22:382, 1951.)
from Martin EE, Henry JP: Effects of time and temperature upon
person to an acceleratory force from top to bottom of 3.3. G. (Data
arterial pressures after abrupt and continuing exposure of a sitting
Figure 43–3
Changes in systolic (top of curve) and diastolic (bottom of curve)
nearby heavenly body is still active. However, the
gravity to pull on the body, because gravity from any
inside its chambers. The cause of this is not failure of
bottom, sides, or top of the spacecraft but simply
. That is, the person is not drawn toward the
near-zero G force, which is sometimes called
, or a state of
Weightlessness in Space
system for recycling has yet to be achieved.
process of photosynthesis. A completely satisfactory
release oxygen. Others depend on biological methods,
physical procedures, such as electrolysis of water to
again. Some recycling processes depend on purely
proposed for use of the same oxygen over and over
supply. For this reason, recycling techniques have been
For space travel lasting more than several months,
plugs.
760 mm Hg. The presence of nitrogen in the mixture
equal to those in normal air are used, with four times
used, but in the modern space shuttle, gases about
ing pure oxygen at about 260 mm Hg pressure was
earlier space missions, a capsule atmosphere contain-
centration low enough to prevent suffocation. In some
spacecraft. Most important, the oxygen concentration
Because there is no atmosphere in outer space, an arti-
“Artificial Climate” in the
cushion the shock of landing.
brae, or leg. Consequently, the trained parachutist
of the body, resulting in fracture of his pelvis, verte-
the earth with extended legs, and this will result in
from a height of about 6 feet. Unless forewarned, the
is properly trained in landing. Actually, the force of
1/81 the impact force without a parachute. Even so,
second, and the force of impact against the earth is
other words, the speed of landing is about 20 feet per
chutist to about one ninth the terminal velocity. In
The usual-sized parachute slows the fall of the para-
pounds can occur on the parachute shrouds.
parachute, an
per hour (175 feet per second). If the parachutist has
that after falling for about 12 seconds, the person will
exactly balances the acceleratory force of gravity, so
Finally, the deceleratory force of the air resistance
the air resistance tending to slow the fall also increases.
per second; and so on. As the velocity of fall increases,
(if there is no air resistance); in 2 seconds it is 64 feet
However, because of the acceleratory force of gravity,
When the parachuting aviator leaves the airplane, his
Deceleratory Forces Associated with Parachute Jumps.
than is necessary at lower velocities.
for a short time. Therefore, deceleration must be
this, a human being can withstand far less deceleration
versus Mach 100 about 10,000-fold. But in addition to
of the velocity, which alone increases the
for safe deceleration. The principal reason for this dif-
0.12 mile, whereas a person traveling at a speed of
spacecraft re-enters the atmosphere. A person travel-
Aviation, High-Altitude, and Space Physiology
Chapter 43
543
Problems also occur during deceleration when the
ing at Mach 1 (the speed of sound and of fast air-
planes) can be safely decelerated in a distance of about
Mach 100 (a speed possible in interplanetary space
travel) would require a distance of about 10,000 miles
ference is that the total amount of energy that must
be dispelled during deceleration is proportional to
the square
required distance for decelerations between Mach 1
if the period of deceleration lasts for a long time than
accomplished much more slowly from high velocities
velocity of fall is at first exactly 0 feet per second.
within 1 second his velocity of fall is 32 feet per second
be falling at a “terminal velocity” of 109 to 119 miles
already reached terminal velocity before opening his
“opening shock load” of up to 1200
the force of impact is still great enough to cause con-
siderable damage to the body unless the parachutist
impact with the earth is about the same as that which
would be experienced by jumping without a parachute
parachutist will be tricked by his senses into striking
tremendous deceleratory forces along the skeletal axis
strikes the earth with knees bent but muscles taut to
Sealed Spacecraft
ficial atmosphere and climate must be produced in a
must remain high enough and the carbon dioxide con-
as much nitrogen as oxygen and a total pressure of
greatly diminishes the likelihood of fire and explosion.
It also protects against development of local patches
of lung atelectasis that often occur when breathing
pure oxygen because oxygen is absorbed rapidly when
small bronchi are temporarily blocked by mucous
it is impractical to carry along an adequate oxygen
such as use of algae with their large store of chloro-
phyll to release oxygen from carbon dioxide by the
A person in an orbiting satellite or a nonpropelled
spacecraft experiences weightlessness
micro-
gravity
floats
gravity acts on both the spacecraft and the person at
0
1
2
3
4
5
Minutes
Acceleration (G)
0
10
8
6
4
2
First
booster
Second
booster
Space
ship
Acceleratory forces during takeoff of a spacecraft.
Figure 43–4
we learned? J Appl Physiol 91:2415, 2001.
Zhang LF: Vascular adaptation to microgravity: what have
Society, 1998.
and Medicine. Bethesda, MD: American Physiological
West JB: High Life
West JB: Man in space. News Physiol Sci 1:198, 1986.
Physiol Sci 1:25, 1986.
West JB: Climbing Mount Everest without oxygen. News
ight. Nutrition 18:849, 2002.
Smith SM, Heer M: Calcium and bone metabolism during
Biol 204(Pt 18):3151, 2001.
standing human adaptation to altitude in the Andes. J Exp
Rupert JL, Hochachka PW: Genetic approaches to under-
cepts. Annu Rev Med 47:267, 1996.
Hultgren HN: High-altitude pulmonary edema: current con-
failure of reabsorption? News Physiol Sci 18:55, 2003.
Hoschele S, Mairbaurl H: Alveolar
ance. News Physiol Sci 17:122, 2002.
Hochachka PW, Beatty CL, Burelle Y, et al: The lactate
91:2374, 2001.
ight: a NASA perspective. J Appl Physiol
Harm DL, Jennings RT, Meck JV, et al: Gender issues related
345:107, 2001.
Hackett PH, Roach RC: High-altitude illness. N Engl J Med
control by space travel. Acta Physiol Scand 177:299, 2003.
Eckberg DL: Bursting into space: alterations of sympathetic
sures. J Gravit Physiol 9:1, 2002.
static intolerance: implications for effective countermea-
Convertino VA: Mechanisms of microgravity induced ortho-
361:1967, 2003.
Basnyat B, Murdoch DR: High-altitude illness. Lancet
ight. J Appl Physiol 81:98,
Alfrey CP, Udden MM, Leach-Huntoon C, et al: Control of
Physiol 95:2185, 2003.
ight and ground-based models. J Appl
unweighting: space
Adams GR, Caiozzo VJ, Baldwin KM: Skeletal muscle
to 2 to 3 G.
periods (e.g., 1 hour each day) of centrifugal accelera-
more effectively attenuate these changes. One such
measures, in addition to exercise, that can prevent or
emergency landing. Therefore, considerable research
nauts after they land, especially in the event of an
of other planets, such as Mars, the effects of prolonged
tness. As space
bone, and muscle
ight cardiovascular,
ing to the full gravity of Earth. Astronauts returning
ability to stand
exes, and reduced orthostatic tolerance. These
capacity, reduced blood volume, impaired barorecep-
, which includes decreased work
each month even though they continue to exercise.
ight. Studies of astronauts
vascular system, skeletal muscles, and bone despite rig-
ights and prolonged exposure to microgravity,
Prolonged Exposure to Weightlessness.
Cardiovascular, Muscle, and Bone “Deconditioning” During
mechanisms.
tendency to faint (and still do, to some extent) when
rst few days after returning to earth. They also had a
the exercise program had been less vigorous, the astro-
prolonged space missions.
for an extended period of time. For this reason, exer-
from the bones, as well as loss of bone mass. Most of
cardiac output, and (5) loss of calcium and phosphate
strength and work capacity, (4) decrease in maximum
decrease in red blood cell mass, (3) decrease in muscle
are the following: (1) decrease in blood volume, (2)
The observed effects of prolonged stay in space
the same time lack of gravitational signals.
arriving in the equilibrium centers of the brain, and at
rst 2 to 5 days of space travel. This probably
sickness, with nausea and sometimes vomiting, during
to oppose the force of gravity.
static pressures, and (3) diminished physical activity
of travel, (2) translocation of
lessness: (1) motion sickness during the
of weightlessness is not too long. Most of the problems
cance, as long as the period
. The
Physiologic Problems of Weightlessness (Microgravity)
For this reason, the person simply is not attracted
the same time, so that both are pulled with exactly the
Aviation, Space, and Deep-Sea Diving Physiology
544
Unit VIII
same acceleratory forces and in the same direction.
toward any specific wall of the spacecraft.
physiologic problems of weightlessness have not
proved to be of much signifi
that do occur are related to three effects of the weight-
first few days
fluids within the body
because of failure of gravity to cause normal hydro-
because no strength of muscle contraction is required
Almost 50 per cent of astronauts experience motion
the fi
results from an unfamiliar pattern of motion signals
these same effects also occur in people who lie in bed
cise programs are carried out by astronauts during
In previous space laboratory expeditions in which
nauts had severely decreased work capacities for the
fi
they stood up during the first day or so after return to
gravity because of diminished blood volume and
diminished responses of the arterial pressure control
During very long
space fl
gradual “deconditioning” effects occur on the cardio-
orous exercise during the fl
on space flights lasting several months have shown that
they may lose as much 1.0 percent of their bone mass
Substantial atrophy of cardiac and skeletal muscles
also occurs during prolonged exposure to a micro-
gravity environment.
One of the most serious effects is cardiovascular
“deconditioning”
tor refl
changes greatly limit the astronauts’
upright or perform normal daily activities after return-
from space flights lasting 4 to 6 months are also sus-
ceptible to bone fractures and may require several
weeks before they return to pre-fl
fi
flights become
longer in preparation for possible human exploration
microgravity could pose a very serious threat to astro-
effort has been directed toward developing counter-
countermeasure that is being tested is the application
of intermittent “artificial gravity” caused by short
tion of the astronauts while they sit in specially
designed short-arm centrifuges that create forces of up
References
fl
red blood cell mass in spacefl
1996.
to spacefl
paradox in human high-altitude physiological perform-
flooding at high altitude:
space fl
—History of High-Altitude Physiology