
chest wall, they create sound that can be heard.
vessels or ventricles come into contact with a “sounding board,” such as the
walls are then transmitted mainly along the arteries. When the vibrations of the
these valves and the ventricular walls. The vibrations occurring in the arterial
between the walls of the arteries and the semilunar valves, as well as between
arteries, which causes a short period of reverberation of blood back and forth
toward the ventricles, and their elastic stretch recoils the blood back into the
at the end of systole. When the semilunar valves close, they bulge backward
The second heart sound results from sudden closure of the semilunar valves
the stethoscope.
adjacent tissues to the chest wall, where they can be heard as sound by using
and causes vibrating turbulence in the blood. The vibrations travel through the
causes the blood and the ventricular walls, as well as the taut valves, to vibrate
back surging blood to bounce forward again into each respective ventricle. This
The elastic tautness of the chordae tendineae and of the valves then causes the
toward the atria until the chordae tendineae abruptly stop the back bulging.
A-V valves (the tricuspid and mitral valves), causing them to close and bulge
That is, in generating the first heart sound, con-
diately after closure,
vents significant sound. Instead, the cause is
up vibrations. However, this has been shown to cause little, if any, of the sound,
of the heart sounds was that the “slapping” together of the valve leaflets sets
The earliest explanation for the cause
sidered to start when the A-V valves close at the onset of ventricular systole.
because the normal pumping cycle of the heart is con-
and the “dub” is called
systole. The “lub” sound is called the
ventricular (A-V) valves at the beginning of systole, and the “dub” is associated
described as “lub, dub, lub, dub.”The “lub” is associated with closure of the atrio-
Listening with a stethoscope to a normal heart, one hears a sound usually
Heart Sounds
conditions. Then we discuss what happens in the
chapter, we first discuss the factors that cause the
audible sounds occur when the valves open. In this
the valves causes audible sounds. Ordinarily, no
Chapter 9, where it was pointed out that
Dynamics of Valvular and
Heart Valves and Heart Sounds;
C
H
A
P
T
E
R
2
3
269
Congenital Heart Defects
Function of the heart valves was discussed in
closing of
sounds in the heart under normal and abnormal
overall circulatory system when valvular or congen-
ital heart defects are present.
Normal Heart Sounds
with closure of the semilunar (aortic and pulmonary) valves at the end of
first heart sound,
the second heart sound,
Causes of the First and Second Heart Sounds.
because the blood between the leaflets cushions the slapping effect and pre-
vibration of the taut valves imme-
along with vibration of the adjacent walls of the heart and
major vessels around the heart.
traction of the ventricles first causes sudden backflow of blood against the
from all these areas, the cardiologist distinguishes
Figure 23–2
aid of a stethoscope, is called
Listening to the sounds of the body, usually with the
of Normal Heart Sounds
Chest Surface Areas for Auscultation
caused by the inrush of blood into the ventricles, which
occurs when the atria contract, and presumably, it is
frequency—usually 20 cycles/sec or less. This sound
diogram, but it can almost never be heard with a
usually so low that the ear cannot hear it, yet it can
sary for reverberation. The frequency of this sound is
of diastole, the ventricles are not filled sufficiently to
of the sack to cause vibrations in its walls. The reason
water from a faucet into a paper sack, the inrushing
ing blood from the atria. This is analogous to running
third of diastole.
Occasionally a weak, rumbling third
respective sounds.
the first heart sound. The clinician uses these differ-
in comparison with the much looser, less elastic ven-
with the much less taut A-V valves, and (2) the greater
quency than the first heart sound for two reasons: (1)
The second heart sound normally has a higher fre-
cannot be heard with a stethoscope.
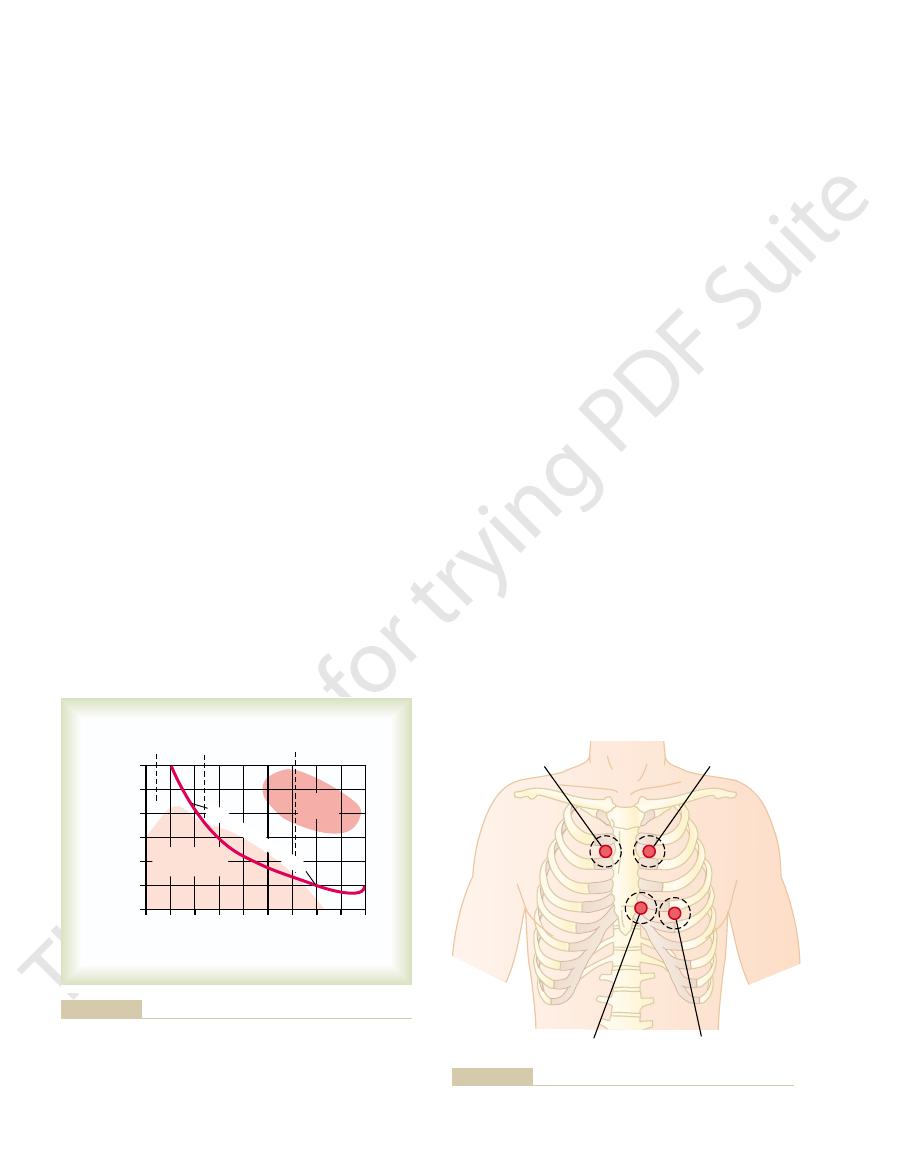
lower shaded area in Figure 23–1. For this reason,
peaking at about 20 cycles/sec, as illustrated by the
the audible range, going down to 3 to 4 cycles/sec and
these sounds, by far a larger proportion of the re-
When special electronic apparatus is used to record
about 40 cycles/sec, and goes up above 500 cycles/sec.
begins at the lowest frequency the ear can detect,
and second heart sounds, as shown in Figure 23–1,
The audible range of frequency (pitch) in the first
a shorter time than do the A-V valves.
more taut than the A-V valves, so that they vibrate for
and the second about 0.11 second. The reason for the
The
270
Unit IV
The Circulation
Duration and Pitch of the First and Second Heart Sounds.
duration of each of the heart sounds is slightly more
than 0.10 second—the first sound about 0.14 second,
shorter second sound is that the semilunar valves are
corded sound is at frequencies and sound levels below
major portions of the heart sounds can be recorded
electronically in phonocardiograms even though they
the tautness of the semilunar valves in comparison
elastic coefficient of the taut arterial walls that provide
the principal vibrating chambers for the second sound,
tricular chambers that provide the vibrating system for
ences to distinguish special characteristics of the two
Third Heart Sound.
heart sound is heard at the beginning of the middle
A logical but unproved explanation
of this sound is oscillation of blood back and forth
between the walls of the ventricles initiated by inrush-
water reverberating back and forth between the walls
the third heart sound does not occur until the middle
third of diastole is believed to be that in the early part
create even the small amount of elastic tension neces-
often be recorded in the phonocardiogram.
Atrial Heart Sound (Fourth Heart Sound).
An atrial heart
sound can sometimes be recorded in the phonocar-
stethoscope because of its weakness and very low
initiates vibrations similar to those of the third heart
sound.
auscultation.
shows the areas of the chest wall from which the dif-
ferent heart valvular sounds can best be distinguished.
Although the sounds from all the valves can be heard
the sounds from the different valves by a process of
Dynes
/c
m
0
8
32
64 128 256 512
2048 4096
Inaudible
Heart sounds
and murmurs
Speech
area
100
10
1
0.1
0.01
0.001
0.0001
1024
2
Frequency in cycles per second
Heart sounds
and murmurs
Threshold of audibili
ty
JL, McGrath JJ: Cardiac Auscultation, 2nd ed. New York: Grune
40 and 520 cycles/sec. (Modified from Butterworth JS, Chassin
showing that the range of sounds that can be heard is between
and heart murmurs in relation to the threshold of audibility,
Amplitude of different-frequency vibrations in the heart sounds
Figure 23–1
& Stratton, 1960.)
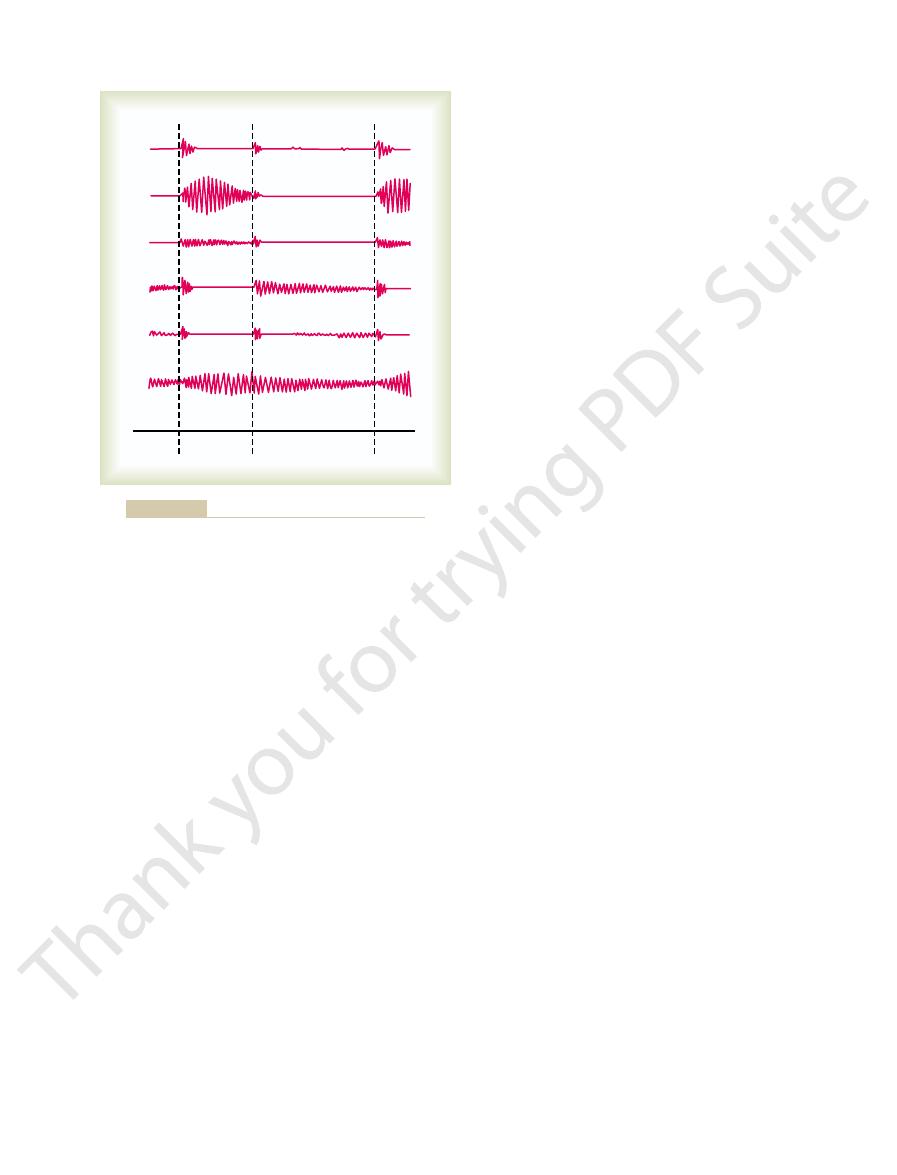
Aortic area
Pulmonic area
Mitral area
Tricuspid area
Chest areas from which sound from each valve is best heard.
Figure 23–2
Other Causes of Valvular Lesions.
tence of at least some degree of regurgitation, and vice
Conversely, when the valve
often become solid, scarred masses.
the leaflets, which are normally filmy and free-flapping,
tions of adjacent valve leaflets. Also, the free edges of
lesions become scar tissue, permanently fusing por-
stuck together. Then, weeks, months, or years later, the
taneously, so that the edges of the leaflets become
The lesions of acute rheumatic
Scarring of the Valves.
valves.
severely, probably because the low-pressure stresses
and pulmonary valves, are usually affected much less
quently damaged. The right heart valves, the tricuspid
damaged, and the aortic valve is second most fre-
other valves, it is the one most often seriously
the heart valves. Because the mitral valve receives
In rheumatic fever, large hemorrhagic, fibrinous,
the kidneys has a similar immunologic basis.
type of reaction are discussed in Chapter 34, and it is
bodies. The principles of immunity that relate to this
certain susceptible areas, such as the heart valves. The
blood—1 year or more.
severe immunologic damage. These reactions continue
with other protein tissues of the body, often causing
The antibodies
antibodies.
ferent proteins against which the person’s reticuloen-
infection. But the streptococci also release several dif-
tially cause a sore throat, scarlet fever, or middle ear
by group A hemolytic streptococci. These bacteria ini-
The sequence of events almost always begins with a
tococcal toxin in the following manner.
damaged or destroyed. It is usually initiated by strep-
rheumatic fever.
Rheumatic Valvular Lesions
Valvular Lesions
people.
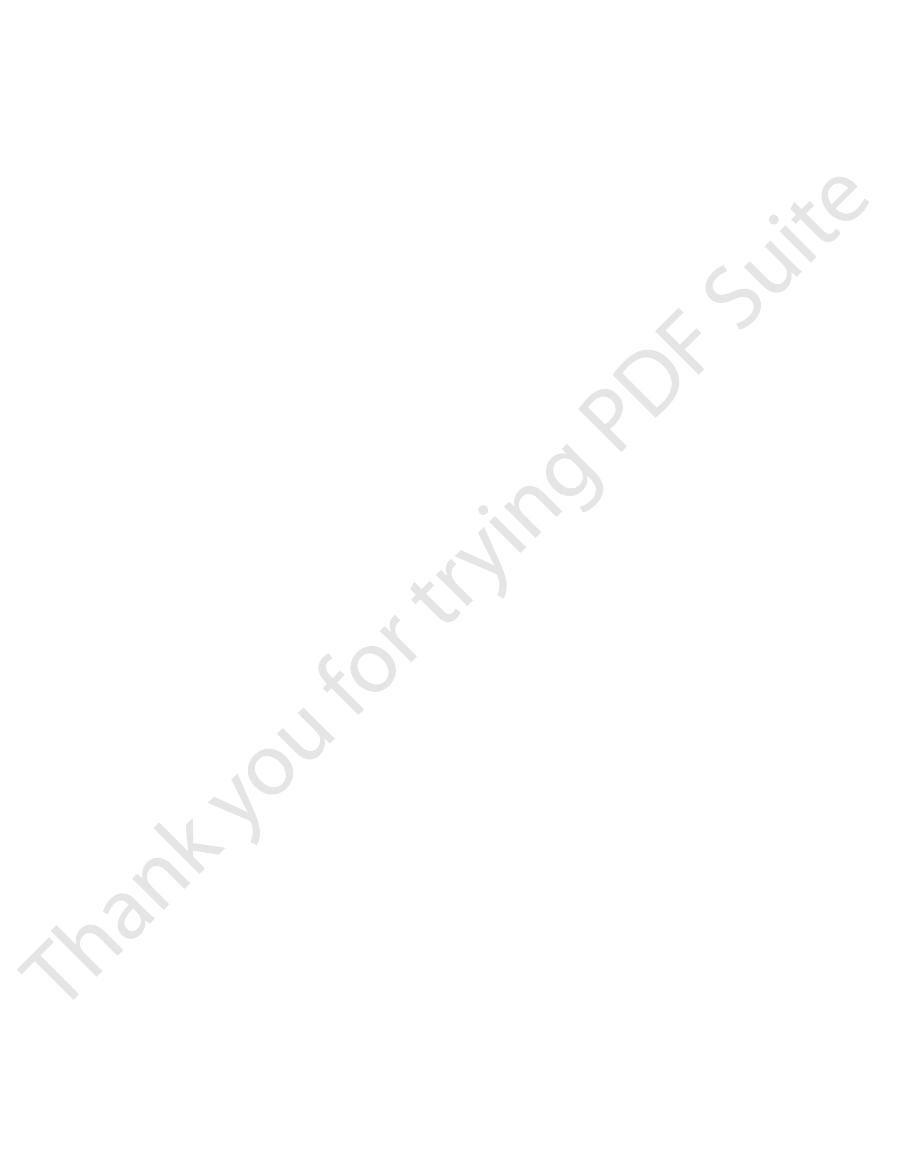
one third to one half of all people, and the atrial heart
rumble. The third heart sound can be recorded in only
even the very weak atrial sound. Note specifically that
tions of the first, second, and third heart sounds and
example of normal heart sounds, showing the vibra-
schematically in Figure 23–3. Recording A is an
and the heart sounds appear as waves, as shown
phonocardio-
ing apparatus. The recording is called a
quency sound is placed on the chest, the heart sounds
Phonocardiogram
posteriorly.
nearest the surface of the chest; the heart is rotated
of the left ventricle, which is the portion of the heart
the right ventricle, and the mitral area is over the apex
along the pulmonary artery. The tricuspid area is over
mission up the aorta, and the pulmonic area is upward
are not directly over the valves themselves. The aortic
The areas for listening to the different heart sounds
sound components from each valve.
from one area to another, noting the loudness of the
elimination. That is, he or she moves the stethoscope
Heart Valves and Heart Sounds; Dynamics of Valvular and Congenital Heart Defects
Chapter 23
271
sounds in different areas and gradually picking out the
area is upward along the aorta because of sound trans-
so that the remainder of the left ventricle lies more
If a microphone specially designed to detect low-fre-
can be amplified and recorded by a high-speed record-
gram,
the third and atrial heart sounds are each a very low
sound can be recorded in perhaps one fourth of all
By far the greatest number of valvular lesions results
from
Rheumatic fever is an autoim-
mune disease in which the heart valves are likely to be
preliminary streptococcal infection caused specifically
dothelial system produces
react not only with the streptococcal protein but also
to take place as long as the antibodies persist in the
Rheumatic fever causes damage especially in
degree of heart valve damage is directly correlated
with the concentration and persistence of the anti-
noted in Chapter 31 that acute glomerular nephritis of
bulbous lesions grow along the inflamed edges of
more trauma during valvular action than any of the
that act on these valves are slight compared with
the high-pressure stresses that act on the left heart
fever frequently occur on adjacent valve leaflets simul-
A valve in which the leaflets adhere to one another
so extensively that blood cannot flow through it nor-
mally is said to be stenosed.
edges are so destroyed by scar tissue that they cannot
close as the ventricles contract, regurgitation (back-
flow) of blood occurs when the valve should be closed.
Stenosis usually does not occur without the coexis-
versa.
Stenosis or lack of one
or more leaflets of a valve also occurs occasionally as
a congenital defect. Complete lack of leaflets is rare;
1st
2nd
3rd
Atrial
Diastole
Systole
Diastole
Systole
Aortic regurgitation
Mitral regurgitation
Aortic stenosis
Normal
Patent ductus
arteriosus
Mitral stenosis
A
B
C
D
E
F
Phonocardiograms from normal and abnormal hearts.
Figure 23–3
When the aortic valve is seriously
increases fourfold to fivefold, creating a tremendously
aorta. Sometimes the left ventricular muscle mass
and aortic regurgitation, the left ventricular muscula-
Hypertrophy of the Left Ventricle.
Some of these compensations are the following.
can ameliorate the severity of the circulatory defects.
aorta. Therefore, in either case, the
empty adequately, whereas in
aortic stenosis,
Stenosis and Aortic Regurgitation
Dynamics of the Circulation in Aortic
Heart Disease
Dynamics in Valvular
Abnormal Circulatory
timing, extra review should be undertaken until it is
during diastole. If the reader does not understand this
occur only during systole, whereas the murmurs of
murmur is also evident. Note especially that the
systole and diastole, and the relative timing of each
weakest. The phonocardiograms show how the inten-
murmur, and the mitral stenotic lesion causes the
mitral stenosis. It is obvious from these phonocardio-
stenosis, mitral regurgitation, aortic regurgitation, and
grams B, C, D, and E of Figure 23–3 show, respectively,
Phonocardiograms of Valvular Murmurs.
begins.
for blood to reverberate, and a low rumbling murmur
after partial filling, the ventricle has stretched enough
may be heard during the first third of diastole. Then,
this reason, even in severe mitral stenosis, no murmur
back and forth between the walls of the ventricle. For
During the early part of diastole, a left ventricle with
the low-frequency end of human hearing.
frequency, so that most of the sound spectrum is below
Figure 23–3) are usually weak and of very low
cle does not develop. Consequently, the abnormal
rises above 30 mm Hg, a large pressure differential
cle, and because the pressure in the left atrium seldom
In mitral stenosis,
atrium. As a result, the sound of mitral regurgitation
However, the left atrium is so deep within the chest
tion but occurring during systole rather than diastole.
ing C, Figure 23–3) similar to that of aortic regurgita-
high-frequency “blowing,” swishing sound (see record-
This also causes a
during systole.
tation, blood flows backward through the mitral valve
ventricle.
cle (see recording D, Figure 23–3). This murmur results
a “blowing” murmur of relatively high pitch with a
high-pressure aorta into the left ventricle, causing
during diastole,
tation, no abnormal sound is heard during systole,
lower neck, a phenomenon known as a “thrill.”
feet away from the patient. Also, the sound vibrations
arteries of the neck. This sound is harsh and in severe
tion, and a loud murmur (see recording B, Figure 23–3)
the blood in the root of the aorta. The turbulent blood
opening of the valve. This causes
during systole,
while the pressure in the aorta is still normal. Thus,
sure in the left ventricle rises as high as 300 mm Hg,
the resistance to ejection, sometimes the blood pres-
small fibrous opening of the aortic valve. Because of
In aortic stenosis,
valves, as follows.
murmurs,” occur when there are abnormalities of the
many abnormal heart sounds, known as “heart
As shown by the phonocardiograms in Figure 23–3,
Heart Murmurs Caused by Valvular Lesions
later in this chapter.
is more common, as is discussed
272
Unit IV
The Circulation
congenital stenosis
Systolic Murmur of Aortic Stenosis.
blood is ejected from the left ventricle through only a
a nozzle effect is created
with blood
jetting at tremendous velocity through the small
severe turbulence of
impinging against the aortic walls causes intense vibra-
occurs during systole and is transmitted throughout
the superior thoracic aorta and even into the large
stenosis may be so loud that it can be heard several
can often be felt with the hand on the upper chest and
Diastolic Murmur of Aortic Regurgitation.
In aortic regurgi-
but
blood flows backward from the
swishing quality heard maximally over the left ventri-
from turbulence of blood jetting backward into the
blood already in the low-pressure diastolic left
Systolic Murmur of Mitral Regurgitation.
In mitral regurgi-
into the left atrium
It is transmitted most strongly into the left atrium.
that it is difficult to hear this sound directly over the
is transmitted to the chest wall mainly through the left
ventricle to the apex of the heart.
Diastolic Murmur of Mitral Stenosis.
blood passes with difficulty through the stenosed
mitral valve from the left atrium into the left ventri-
forcing blood from the left atrium into the left ventri-
sounds heard in mitral stenosis (see recording E,
a stenotic mitral valve has so little blood in it and its
walls are so flabby that blood does not reverberate
Phonocardio-
idealized records obtained from patients with aortic
grams that the aortic stenotic lesion causes the loudest
sity of the murmurs varies during different portions of
murmurs of aortic stenosis and mitral regurgitation
aortic regurgitation and mitral stenosis occur only
understood.
In
the contracting left ventricle fails to
aortic regurgitation,
blood flows backward into the ventricle from the aorta
after the ventricle has just pumped the blood into the
net stroke volume
output of the heart is reduced.
Several important compensations take place that
In both aortic stenosis
ture hypertrophies because of the increased ventricu-
lar workload.
In regurgitation, the left ventricular chamber also
enlarges to hold all the regurgitant blood from the
large left side of the heart.
stenosed, the
hypertrophied muscle allows the left ventricle to
develop as much as 400 mm Hg intraventricular pres-
sure at systolic peak.
cardiac reserve
the patient’s
Even in mild to moderate cases of valvular disease,
as little as 10 minutes.
Also, in patients with mitral disease, exercise
aortic valvular lesions, exercise can cause acute left
during heavy exercise. For instance, in patients with
ognizable at rest, severe symptoms often develop
heart disease, in which the symptoms may be unrec-
tremendously exacerbated. Even in mild valvular
Therefore, all the dynamic abnormalities that occur in
During exercise, large quantities of venous blood are
in Patients with Valvular Lesions
right side of the heart, which partially compensates for
double normal. This, in turn, causes hypertrophy of the
times to as high as 60 mm Hg, which is more than
rial pressure and also right ventricular pressure, some-
lungs causes pulmonary arteriolar constriction. These
monary artery. In addition, incipient edema of the
up in the lungs, eventually all the way back to the pul-
As the left atrial pressure rises, blood begins to dam
sure is rising.
mitral valvular disease, even though the left atrial pres-
cardiac debility. Therefore, after compensation, cardiac
heart, thereby helping to overcome the effect of the
ished excretion of water and salt by the kidneys. This
congenital heart disease, the blood volume increases
Compensation in Early Mitral Valvular Disease.
and causes further cardiac debility.
mitral stenosis, atrial fibrillation usually occurs. This
in late stages of mitral valvular disease, especially in
as discussed in Chapter 13. Therefore,
movements,
tatory impulse must travel in the atrial wall. This
progressive enlargement of the left atrium, which
The high left
lung tissues extremely rapidly.
as 40 mm Hg, because the lung lymphatic vasculature
development of serious pulmonary edema. Ordinarily,
in left atrial pressure, and this eventually results in
The buildup
Pulmonary Edema in Mitral Valvular Disease.
ventricle.
aorta. Therefore, either of these conditions reduces net
tion, much of the blood that has flowed into the left
the left ventricle is impeded, and in mitral regurgita-
In mitral stenosis, blood flow from the left atrium into
Mitral Regurgitation
Dynamics of Mitral Stenosis and
to 40 mm Hg, serious edema appears in the lungs, as
gressively, and at mean left atrial pressures above 25
failing left ventricle. The left atrial pressure rises pro-
and cardiac output begins to fall; blood simultaneously
demand. As a consequence, the left ventricle dilates
Beyond a critical stage in these aortic valve lesions,
tricle. Therefore, considerable degrees of aortic steno-
in circulatory function in the person during rest, other
tation, the intrinsic ability of the left ventricle to adapt
Development of Pulmonary Edema
Eventual Failure of the Left Ventricle, and
overcome the abnormal pumping dynamics.
venous return to the heart. This, in turn, causes the left
The increase in blood volume tends to increase
the mean arterial pressure to return to normal. Also,
of urine, causing the blood volume to increase and
pressure induces. These together diminish renal output
(1) an initial slight decrease in arterial pressure, plus
ventricle is increased blood volume. This results from
Increase in Blood Volume.
flows through the aorta to the body.
to the ventricle during diastole, and only one fourth
stroke volume output as great as 250 milliliters,
In severe aortic regurgitation, sometimes the hyper-
Heart Valves and Heart Sounds; Dynamics of Valvular and Congenital Heart Defects
Chapter 23
273
trophied muscle allows the left ventricle to pump a
although as much as three fourths of this blood returns
Another effect that helps
compensate for the diminished net pumping by the left
(2) peripheral circulatory reflexes that the decrease in
red cell mass eventually increases because of a slight
degree of tissue hypoxia.
ventricle to pump with the extra power required to
In the early stages of aortic stenosis or aortic regurgi-
to increasing loads prevents significant abnormalities
than increased work output required of the left ven-
sis or aortic regurgitation often occur before the
person knows that he or she has serious heart disease
(such as a resting left ventricular systolic pressure as
high as 200 mm Hg in aortic stenosis or a left ventric-
ular stroke volume output as high as double normal in
aortic regurgitation).
the left ventricle finally cannot keep up with the work
dams up in the left atrium and in the lungs behind the
discussed in detail in Chapter 38.
ventricle during diastole leaks back into the left atrium
during systole rather than being pumped into the
movement of blood from the left atrium into the left
of blood in the left atrium causes progressive increase
lethal edema does not occur until the mean left atrial
pressure rises above 25 mm Hg and sometimes as high
enlarges manyfold and can carry fluid away from the
Enlarged Left Atrium and Atrial Fibrillation.
atrial pressure in mitral valvular disease also causes
increases the distance that the cardiac electrical exci-
pathway may eventually become so long that it pre-
disposes to development of excitatory signal circus
further reduces the pumping effectiveness of the heart
As also
occurs in aortic valvular disease and in many types of
in mitral valvular disease principally because of dimin-
increased blood volume increases venous return to the
output may fall only minimally until the late stages of
two effects together increase systolic pulmonary arte-
its increased workload.
Circulatory Dynamics During Exercise
returned to the heart from the peripheral circulation.
the different types of valvular heart disease become
ventricular failure followed by acute pulmonary
edema.
can cause so much damming of blood in the lungs that
serious or even lethal pulmonary edema may ensue in
diminishes in proportion
tion. But as the child grows older, the differential
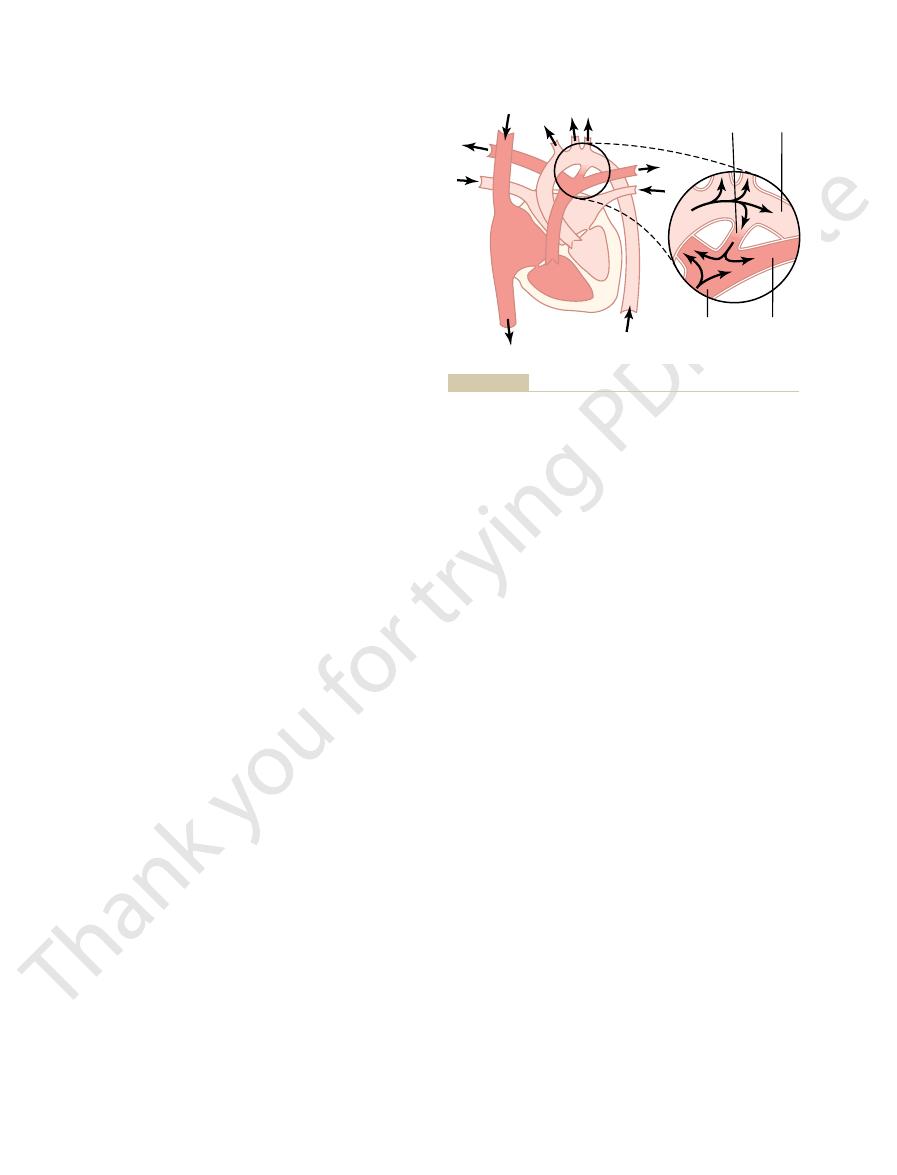
During the early months of an infant’s life, a patent
which is shown in Figure 23–4.
patent ductus arteriosus,
ductus does not close, causing the condition known as
Unfortunately, in about 1 of every 5500 babies, the
constricts the muscle in the ductus wall. This is dis-
the ductus during fetal life. The oxygen presumably
ductus does not persist. The ductus is believed to close
days in most babies, so that blood flow through the
from the aorta into the pulmonary artery. This new
fact, blood begins to flow backward through the ductus
the ductus arteriosus ceases suddenly at birth, and in
the aorta rises. As a result, forward blood flow through
pressure in the pulmonary artery falls, while that in
flow from the aorta through the placenta. Thus, the
arterial pressure to fall. Simultaneously, the aortic
tree decreases tremendously, allowing the pulmonary
not only do the alveoli fill with air, but also the resist-
baby is born and begins to breathe, the lungs inflate;
As soon as a
lungs. This lack of blood flow through the lungs is not
thus bypassing the lungs. This allows immediate
sus,
with the aorta (Figure 23–4), called the
in the pulmonary artery. This causes almost all the pul-
of the fetus is lower than normal—in fact, lower than
large vessels of the placenta, the pressure in the aorta
rial pressure is high in the fetus. Also, because of low
lapsed as well. Therefore, resistance to blood flow
During fetal life, the lungs are collapsed, and the
A Left-to-Right Shunt
Patent Ductus Arteriosus—
small collateral arteries, as discussed in Chapter 19.
flow through the coarctation to the lower body; part of
diaphragm. This causes the arterial pressure in the
tendency to develop serious pulmonary edema and a
stenosis caused by other valvular lesions, namely, a
understood. For instance,
The effects of the different stenotic lesions are easily
left side of the heart, thus failing to flow through the
right side of the heart or pulmonary artery, thus failing
blood vessel; (2) an anomaly that allows blood to flow
vessels: (1)
There are three major types of
congenital anomaly.
are malformed during fetal life; the defect is called a
Occasionally, the heart or its associated blood vessels
Heart Defects
Abnormal Circulatory
blood flow.
during exercise. Therefore, the muscles of the body
to the severity of the valvular dysfunction. That is, the
274
Unit IV
The Circulation
cardiac output does not increase as much as it should
fatigue rapidly because of too little increase in muscle
Dynamics in Congenital
congenital anomalies of the heart and its associated
stenosis of the channel of blood flow at
some point in the heart or in a closely allied major
backward from the left side of the heart or aorta to the
to flow through the systemic circulation—called a left-
to-right shunt; and (3) an anomaly that allows blood to
flow directly from the right side of the heart into the
lungs—called a right-to-left shunt.
congenital aortic valve steno-
sis results in the same dynamic effects as aortic valve
reduced cardiac output.
Another type of congenital stenosis is coarctation
of the aorta, often occurring near the level of the
upper part of the body (above the level of the coarc-
tation) to be much greater than the pressure in the
lower body because of the great resistance to blood
the blood must go around the coarctation through
elastic compression of the lungs that keeps the alveoli
collapsed keeps most of the lung blood vessels col-
through the lungs is so great that the pulmonary arte-
resistance to blood flow from the aorta through the
monary arterial blood to flow through a special artery
present in the fetus that connects the pulmonary artery
ductus arterio-
recirculation of the blood through the systemic arter-
ies of the fetus without the blood going through the
detrimental to the fetus because the blood is oxy-
genated by the placenta.
Closure of the Ductus Arteriosus After Birth.
ance to blood flow through the pulmonary vascular
pressure rises because of sudden cessation of blood
state of backward blood flow causes the ductus arte-
riosus to become occluded within a few hours to a few
because the oxygen concentration of the aortic blood
now flowing through it is about twice as high as that
of the blood flowing from the pulmonary artery into
cussed further in Chapter 83.
Dynamics of the Circulation with a Persistent Patent Ductus.
ductus usually does not cause severely abnormal func-
between the high pressure in the aorta and the lower
Head and upper
extremities
Trunk and lower
extremities
Right
lung
Left lung
Pulmonary
artery
Aorta
Ductus
arteriosus
Left
pulmonary
artery
through the lungs for a second time.
flow of blood from the aorta into the pulmonary artery and then
ent points in the circulation. The right-hand diagram shows
that dark venous blood changes into oxygenated blood at differ-
Patent ductus arteriosus, showing by the intensity of the pink color
Figure 23–4
back-
its becoming oxygenated. As much as 75 per cent of
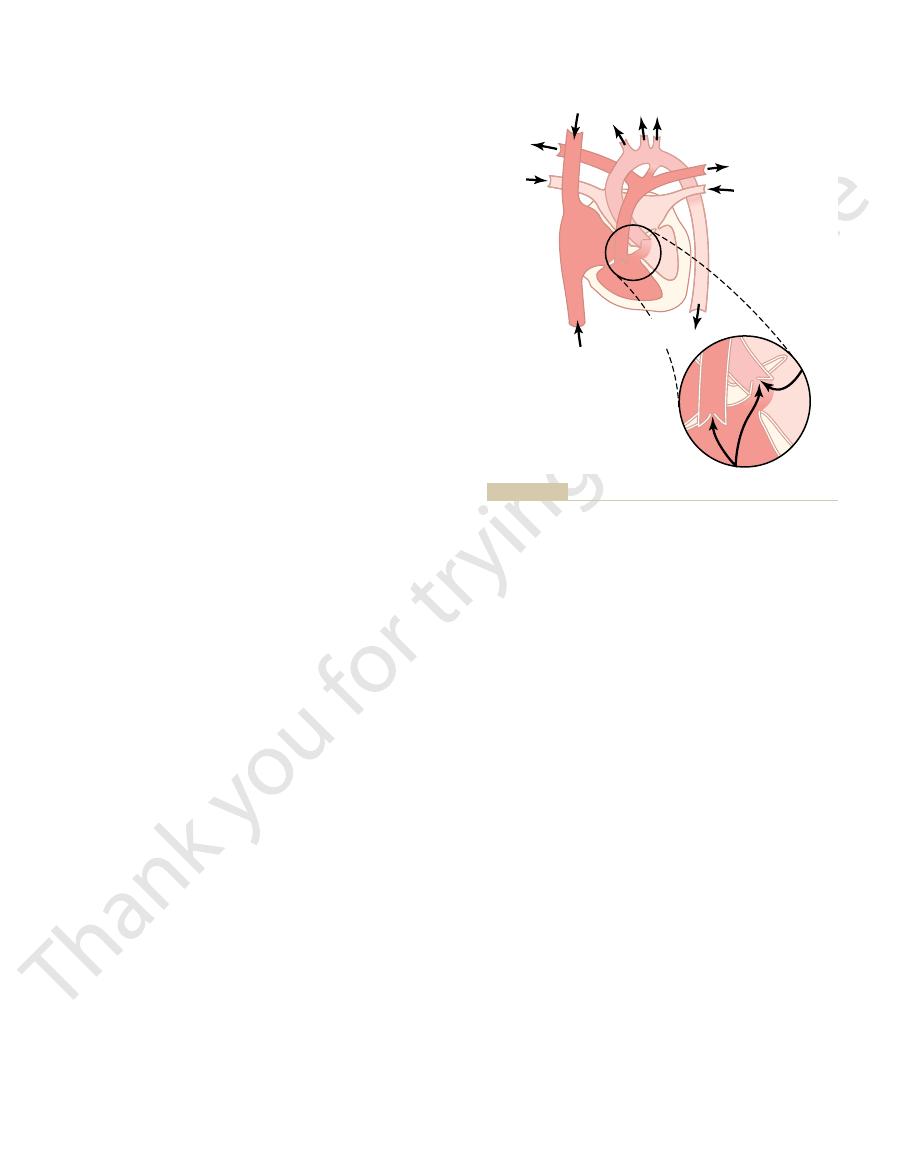
of Fallot is the shunting of blood past the lungs without
Abnormal Circulatory Dynamics.
causing an enlarged right ventricle.
in the aorta, its musculature is highly developed,
4. Because the right side of the heart must pump
that overrides this hole.
3. Blood from the left ventricle flows either through
bypassing the lungs.
the blood passes directly into the aorta, thus
the right ventricle into the lungs; instead, most of
2. The pulmonary artery is stenosed, so that much
from both ventricles.
septum, as shown in Figure 23–5, receiving blood
rather than the left, or it overrides a hole in the
1. The aorta originates from the right ventricle
genated venous blood. In this condition, four abnor-
bypasses the lungs, so the aortic blood is mainly unoxy-
most common cause of “blue baby.” Most of the blood
Tetralogy of Fallot is shown in Figure 23–5; it is the
A Right-to-Left Shunt
Tetralogy of Fallot—
In fact, this was one of the first successful heart sur-
patent ductus or divide it and then close the two ends.
arteriosus is extremely simple; one need only ligate the
Surgical Treatment.
machinery murmur.
the heart, creating the so-called
during diastole when the aortic pressure falls low, so
This sound is much more intense during systole when
area of the chest, as shown in recording F, Figure 23–3.
older, reaching age 1 to 3 years, a harsh, blowing
cient to cause a heart murmur. But as the baby grows
with patent ductus arteriosus, occasionally no abnor-
Heart Sounds: Machinery Murmur.
ages 20 and 40 years.
sively more severe with age, most patients with uncor-
of the excessive load on the heart, and especially
monary congestion and pulmonary edema. As a result
The high pressures in the pulmonary vessels caused
even faint from momentary heart failure.
exercise, the person is likely to become weak and may
strenuous activity. With even moderately strenuous
exercise, the net blood flow through the remainder of
about four to seven times normal. Therefore, during
normal cardiac output, and the maximum that it can
are decreased cardiac and respiratory reserve. The left
The
times it passes through the lungs.
Indeed, early in life, the arterial blood is often
in life, when the heart fails or the lungs become con-
do not show cyanosis until later
culation. These people
into the left ventricle and aorta, passing through the
monary artery, then through the lungs, and finally back
with a patent ductus, one half to two thirds of the aortic
time, making the condition even worse.
Also, the high aortic blood pressure usually causes the
of blood from the aorta into the pulmonary artery.
creases, with corresponding increase in backward flow
Heart Valves and Heart Sounds; Dynamics of Valvular and Congenital Heart Defects
Chapter 23
275
pressure in the pulmonary artery progressively in-
diameter of the partially open ductus to increase with
Recirculation Through the Lungs.
In an older child
blood flows backward through the ductus into the pul-
lungs and left side of the heart two or more times for
every one time that it passes through the systemic cir-
gested.
better oxygenated than normal because of the extra
Diminished Cardiac and Respiratory Reserve.
major effects of patent ductus arteriosus on the patient
ventricle is pumping about two or more times the
pump after hypertrophy of the heart has occurred is
the body can never increase to the levels required for
by excess flow through the lungs often lead to pul-
because the pulmonary congestion becomes progres-
rected patent ductus die from heart disease between
In a newborn infant
mal heart sounds are heard because the quantity of
reverse blood flow through the ductus may be insuffi-
murmur begins to be heard in the pulmonary artery
the aortic pressure is high and much less intense
that the murmur waxes and wanes with each beat of
Surgical treatment of patent ductus
geries ever performed.
malities of the heart occur simultaneously:
lower than normal amounts of blood pass from
a ventricular septal hole into the right ventricle
and then into the aorta or directly into the aorta
large quantities of blood against the high pressure
It is readily apparent that
the major physiological difficulty caused by tetralogy
the venous blood returning to the heart passes directly
Head and upper
extremities
Trunk and lower
extremities
Right
lung
Left lung
into the aorta without passing through the lungs.
most of the dark venous blood is shunted from the right ventricle
Tetralogy of Fallot, showing by the intensity of the pink color that
Figure 23–5
disease. J Am Coll Cardiol 39:1890, 2002.
Hoffman JI, Kaplan S: The incidence of congenital heart
Guidelines. Circulation 98:1949, 1998.
ology/American Heart Association Task Force on Practice
heart disease. A report of the American College of Cardi-
327:97, 2003.
Grech ED: Non-coronary percutaneous intervention. BMJ
advantages, and limitations. Curr Probl Cardiol 28:485,
Gottdiener JS: Overview of stress echocardiography: uses,
in adults: second of two parts. N Engl J Med 342:334, 2000.
Brickner ME, Hillis LD, Lange RA: Congenital heart disease
Circulation 106:1312, 2002.
uation and management of hypertrophic cardiomyopathy.
Braunwald E, Seidman CE, Sigwart U: Contemporary eval-
hypertrophic cardiomyopathy. Hum Mol Genet 11:2499,
Arad M, Seidman JG, Seidman CE: Phenotypic diversity in
great as 800 grams instead of the normal 300 grams.
genital disease, sometimes causing heart weights as
ventricle must work, with emphasis on pressure. Thus,
stimulus. Regardless of which of these is correct, one
causes the hypertrophy; others believe that the
must be pumped. Some physicians believe that the
increased workloads, whether these loads are caused
Heart Disease
in Valvular and Congenital
Hypertrophy of the Heart
hands of experts, patients can be kept alive on artifi-
cal procedure. Yet despite these difficulties, in the
coagulation in the extracorporeal system. Heparin also
oxygen, and necessity to use heparin to prevent blood
system, failure to exchange adequate quantities of
agent passing into the arteries of the patient, necessity
development of small clots in the blood, likelihood of
many difficulties, including hemolysis of the blood,
The different systems have all been fraught with
dioxide.
passing the blood over surfaces of rotating discs, or (4)
faces of plastic sheets in the presence of oxygen, (3)
patient, (2) dripping the blood downward over the sur-
blood seems to be suitable.
pally of a pump and an oxygenating device. Almost
The system consists princi-
during the course of operation. Such a system is called
heart-lung machines
surgically while the heart is still pumping. Therefore,
Cardiac Surgery
Circulation During
Use of Extracorporeal
body.
associated with other congenital defects of the baby’s
having congenital heart disease than other children do.
identical twins as well as in succeeding generations.
Some congenital defects of the heart are hereditary,
trimester.
pregnancy if German measles occurs in the first
measles; thus, obstetricians often advise termination of
formed. Defects are particularly prone to develop
trimester of pregnancy when the fetal heart is being
Causes of Congenital Anomalies
increases from only 3 to 4 years to 50 or more years.
surgery is successful, the average life expectancy
and reconstruct the flow pathway into the aorta. When
to open the pulmonary stenosis, close the septal defect,
treated successfully by surgery. The usual operation is
Tetralogy of Fallot can usually be
Surgical Treatment.
stenosed pulmonary artery.
the overriding aorta, but much less flow through the
heart, showing an enlarged right ventricle; and (4)
ventricle, recorded through a catheter; (3) charac-
(blue); (2)
(1) the fact that the baby’s skin is
A diagnosis of tetralogy of Fallot is usually based on
276
Unit IV
The Circulation
from the right ventricle into the aorta without becom-
ing oxygenated.
cyanotic
measurement of high systolic pressure in the right
teristic changes in the radiological silhouette of the
angiograms (x-ray pictures) showing abnormal blood
flow through the interventricular septal hole and into
One of the most common causes of congenital heart
defects is a viral infection in the mother during the first
when the expectant mother contracts German
because the same defect has been known to occur in
Children of patients surgically treated for congenital
heart disease have about a 10 times greater chance of
Congenital defects of the heart are also frequently
It is almost impossible to repair intracardiac defects
many types of artificial
have been
developed to take the place of the heart and lungs
extracorporeal circulation.
any type of pump that does not cause hemolysis of the
Methods used for oxygenating blood include (1)
bubbling oxygen through the blood and removing the
bubbles from the blood before passing it back into the
passing the blood between thin membranes or through
thin tubes that are permeable to oxygen and carbon
small bubbles of oxygen or small emboli of antifoam
for large quantities of blood to prime the entire
interferes with adequate hemostasis during the surgi-
cial heart-lung machines for many hours while opera-
tions are performed on the inside of the heart.
Hypertrophy of cardiac muscle is one of the most
important mechanisms by which the heart adapts to
by increased pressure against which the heart muscle
must contract or by increased cardiac output that
increased strength of contraction of the heart muscle
increased metabolic rate of the muscle is the primary
can calculate approximately how much hypertrophy
will occur in each chamber of the heart by multiplying
ventricular output by the pressure against which the
hypertrophy occurs in most types of valvular and con-
References
2002.
2003.
Guidelines for the management of patients with valvular
therapy. Rev Cardiovasc Med 4:199, 2003.
diomyopathy: mechanism of obstruction and response to
Yoerger DM, Weyman AE: Hypertrophic obstructive car-
109:942, 2004.
repair: from structure to function. Part II. Circulation
Yacoub MH, Cohn LH: Novel approaches to cardiac valve
therapeutic implications. Chest 124:1929, 2003.
in rheumatic mitral stenosis: methods of assessment and
Turgeman Y, Atar S, Rosenfeld T: The subvalvular apparatus
Med 343:611, 2000.
outcome in severe, asymptomatic aortic stenosis. N Engl J
Rosenhek R, Burder T, Pozenta G, et al: Predictors of
disease in pregnancy. N Engl J Med 349:52, 2003.
Reimold SC, Rutherford JD: Clinical practice: valvular heart
1320, 2004.
trophic obstructive cardiomyopathy. N Engl J Med 350:
Nishimura RA, Holmes DR Jr: Clinical practice: hyper-
throat? Lancet Infect Dis 4:240, 2004.
fever: a chink in the chain that links the heart to the
McDonald M, Currie BJ, Carapetis JR: Acute rheumatic
review. JAMA 287:1308, 2002.
Maron BJ: Hypertrophic cardiomyopathy: a systematic
diology in pediatrics. Curr Opin Cardiol 18:79, 2003.
Levi DS, Alejos JC, Moore JW: Future of interventional car-
Heart Valves and Heart Sounds; Dynamics of Valvular and Congenital Heart Defects
Chapter 23
277