Basic Anatomy
683
C H A P T E R O U T L I N E
(continued)
Splenius 695
Muscular Triangles of the
Back 695
Deep Fascia of the Back
(Thoracolumbar Fascia) 695
Blood Supply of the Back 695
Arteries 695
Veins 695
Lymph Drainage of the Back 695
Nerve Supply of the Back 695
Spinal Cord 697
Roots of the Spinal Nerves 698
Blood Supply of the Spinal
Cord 699
Meninges of the Spinal Cord 699
Cerebrospinal Fluid 707
Radiographic Anatomy 710
Radiographic Appearances of the
Vertebral Column 710
Spinal Subarachnoid Space 710
Computed Tomography and
Magnetic Resonance Imaging
Studies 715
Surface Anatomy 717
Midline Structures 717
External Occipital
Protuberance 717
Cervical Vertebrae 717
Thoracic and Lumbar
Vertebrae 717
Sacrum 717
Coccyx 718
Upper Lateral Part of the Thorax 718
Scapula 718
Lower Lateral Part of the Back 718
Iliac Crests 718
Spinal Cord and Subarachnoid
Space 719
Symmetry of the Back 719
C H A P T E R O B J E C T I V E S
The physician’s task is to identify the likely source of the pain
Back injuries range from a simple muscular or ligamentous back
■
■
strain to a catastrophic injury of the spinal cord or cauda equina.
■
■
Automobile accidents, motorcycle accidents, gunshot wounds,
and sports injuries are just some of the common causes of back
injuries found in practice.
■
■
Because of the anatomic configuration of this region, unpro-
tected movement of the damaged vertebral column during initial
medical care at the site of the accident can result in irreversible
injury to the delicate spinal cord.
■
■
Back pain provides the practicing physician with a challenge.
and the pathologic process causing it.
■
■
The purpose of this chapter is to review the basic anatomy of
the vertebral column and related soft nervous tissue structures
so that the physician will feel reasonably confident to institute
the appropriate treatment.
natomy
asic
B
a
The back, which extends from the skull to the tip of the
monly fused). Because it is segmented and made up of verte
to form the sacrum), and 4 coccygeal (the lower 3 are com
vertebrae—7 cervical, 12 thoracic, 5 lumbar, 5 sacral (fused
The vertebral column (Figs. 12.1 and 12.2) is composed of 33
Composition of the Vertebral Column
ges, to which the vertebral column gives great protection.
cord, the roots of the spinal nerves, and the covering menin
weight to the lower limbs. Within its cavity lie the spinal
racic cage and, by way of the pelvic girdle, transmits body
It supports the skull, pectoral girdle, upper limbs, and tho
The vertebral column is the central bony pillar of the body.
The Vertebral Column
the scapulae to the trunk.
the thorax are the scapulae and the muscles that connect
Superimposed on the upper part of the posterior surface of
coccyx, can be defined as the posterior surface of the trunk.
-
-
-
-
brae, joints, and pads of fibrocartilage called intervertebral
discs, it is a flexible structure. The
ertebral discs form
interv
about one quarter the length of the column.
processes are directed laterally from the junction of the
from the junction of the two laminae. The transverse
is directed posteriorly
or
spinous process,
The
spinous, two transverse, and four articular (Fig. 12.2).
The vertebral arch gives rise to seven processes: one
posteriorly.
which complete the arch
and a pair of flattened
which form the sides of the arch,
pedicles,
of cylindrical
cord and its coverings. The vertebral arch consists of a pair
through which run the spinal
vertebral foramen,
called the
posteriorly. These enclose a space
vertebral arch
orly and a
anteri
body
consists of a rounded
typical vertebra
sess a common pattern (Fig. 12.2).
Although vertebrae show regional differences, they all pos
General Characteristics of a Vertebra
-
A
-
laminae,
spine,

684
CHAPTER 12
are vertically arranged and
articular processes
The
and ligaments.
processes serve as levers and receive attachments of muscles
laminae and the pedicles. Both the spinous and transverse
The Back
consist of two superior and two inferior processes. They
The pedicles are notched on their superior and
the arch above, forming two synovial joints.
arch articulate with the two inferior articular processes of
The two superior articular processes of one vertebral
their articular surfaces are covered with hyaline cartilage.
arise from the junction of the laminae and the pedicles, and
inferior borders, forming the
inferior
superior and
vertebral notches.
of one vertebra and the inferior notch of an adjacent
On each side, the superior notch
vertebra together form an
rior and posterior nerve roots of a spinal nerve unite
transmit the spinal nerves and blood vessels. The ante
These foramina, in an articulated skeleton, serve to
intervertebral foramen.
-
within these foramina with their
rings of dura to
cove
form the segmental spinal nerves.
mastoid process
trapezius muscle
superior angle of scapula
acromion
spine of scapula
inferior angle of scapula
latissimus dorsi muscle
twelfth rib
iliac crest
iliac tubercle
ischial tuberosity
tip of coccyx
fold of buttock
natal cleft
greater trochanter
posterosuperior iliac spine
erector spinae muscle
spine of seventh
thoracic vertebra
spine of
third thoracic vertebra
head of humerus
spine of seventh cervical vertebra
spine of first thoracic vertebra
ligamentum nuchae
external occipital protuberance
FIGURE 12.1
Posterior view of the skeleton showing the surface markings on the back.

Basic Anatomy
685
atlas
axis
cervical curve
cervical
vertebrae
(7)
thoracic
vertebrae
(12)
lumbar
vertebrae
(5)
sacral
vertebrae
(5)
coccygeal vertebrae
(4)
sacral curve
lumbar curve
thoracic
curve
lamina
pedicle
transverse
process
body
anterior tubercle
foramen
transversarium
posterior tubercle
superior articular
facet
vertebral foramen
facet for
rib tubercle
vertebral foramen
body
demifacet for rib head
pedicle
superior articular
facet
transverse
process
spine
lamina
superior articular
process
transverse process
pedicle
body
vertebral foramen
inferior articular process
promontory
superior articular process
lateral mass
anterior sacral
foramina
transverse process
of coccyx
A
B
spine (bifid)
lamina
spine
C4
T6
L3
S1
2
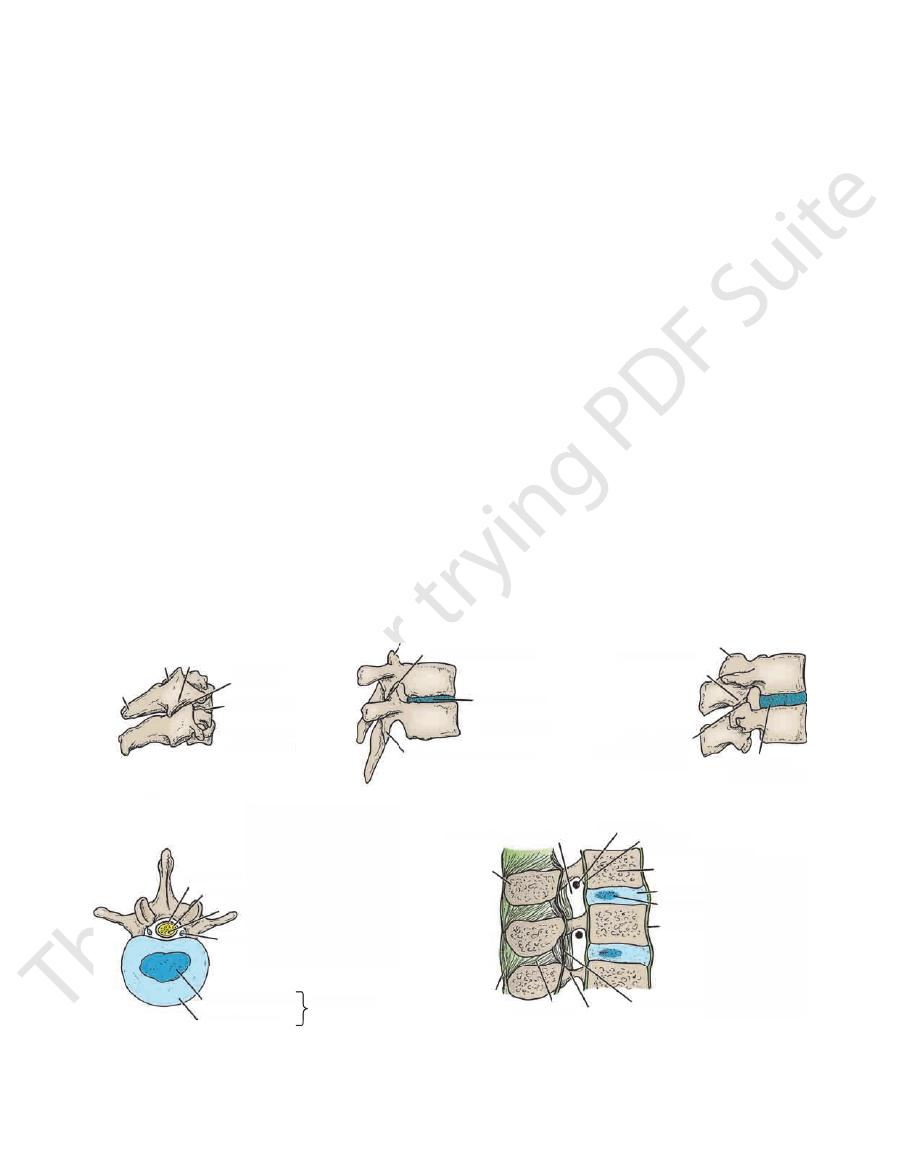
FIGURE 12.2
General features of different kinds of vertebrae.
Lateral view of the vertebral column.
A.
B.

686
CHAPTER 12
The Back
Examination of the Back
Lateral rotation, however, is limited by the interlocking of the
normally be tilted 45° to each shoulder. It is important that the
between the atlas and the axis. In lateral flexion, the head can
nearly in line with the shoulder. Half of lateral rotation occurs
lateral rotation, the patient should be able to place the chin
extension he or she should be able to look directly upward. In
should be able to touch his or her chest with the chin, and in
is carried out at the atlanto-occipital joints. In flexion, the patient
Remember that about half of the movement referred to as flexion
ion, extension, lateral rotation, and lateral flexion are possible.
The normal range of movements of the different parts of the
vexity develops on the opposite side, with a compensatory thoracic
tion room so that the normal tilting movement of the pelvis can be
of the hip joints can lead to abnormal curvatures of the vertebral col
and that the shoes be removed. Unequal length of the legs or disease
It is important that the whole area of the back and legs be examined
-
umn. The patient should be asked to walk up and down the examina-
observed. As one side of the pelvis is raised, a coronal lumbar con-
convexity on the same side. When a person assumes the sitting posi-
tion, it will be noted that the normal lumbar curvature becomes flat-
tened, with an increase in the interval between the lumbar spines.
vertebral column should be tested. In the cervical region, flex-
shoulder is not raised when this movement is being tested.
In the thoracic region, the movements are limited by the pres-
ence of the ribs and sternum. When testing for rotation, make
sure that the patient does not rotate the pelvis.
In the lumbar region, flexion, extension, lateral rotation, and
lateral flexion are possible. Flexion and extension are fairly free.
articular processes. Lateral flexion in the thoracic and lumbar
regions is tested by asking the patient to slide, in turn, each hand
down the lateral side of the thigh.
C L I N I C A L N O T E S
Characteristics of a Typical Cervical Vertebra
veins (note that the vertebral artery passes through the
for the passage of the vertebral artery and
versarium
foramen trans
The transverse processes possess a
(Fig. 12.3):
A typical cervical vertebra has the following characteristics
■
■
-
transverse processes C1 to 6 and not through C7).
The vertebral foramen is large and triangular.
The body is small and broad from side to side.
The spines are small and bifid.
■
■
■
■
■
■
spine
vertebral foramen
superior articular facet
transverse
process
body
foramen transversarium
anterior tubercle
posterior
tubercle
posterior tubercle
vertebral foramen
transverse
process
anterior
tubercle
anterior arch
superior articular facet
foramen transversarium
posterior arch
spine
vertebral foramen
foramen transversarium
transverse process
body
odontoid process
spine
body
A
B
C
D
C4
C4
C7
superior articular
process
FIGURE 12.3
passage for the vertebral vein but not for the vertebral artery.
7th cervical vertebra, superior aspect; the foramen transversarium forms a
cervical vertebra, from above and behind.
Axis, or 2nd
Atlas, or 1st cervical vertebra, superior aspect.
Typical cervical vertebra, superior aspect.
A.
B.
C.
D.

Basic Anatomy
material. It also contains the lower part of the subarach
coccygeal spinal nerves, the filum terminale, and fibrofatty
contains the anterior and posterior roots of the sacral and
(see Fig. 6.8). The sacral canal
sacral hiatus
forming the
times those of the 4th also, fail to meet in the midline,
The laminae of the 5th sacral vertebra, and some
sacral
The vertebral foramina are present and form the
importance and is used when measuring the size of the pelvis.
sacral promontory in the female is of considerable obstetric
The
sacral promontory.
the pelvic inlet and is known as the
first sacral vertebra bulges forward as the posterior margin of
joints (see Fig. 6.1). The anterior and upper margin of the
articulates with the two iliac bones to form the sacroiliac
rior border articulates with the coccyx. Laterally, the sacrum
articulates with the 5th lumbar vertebra. The narrow infe
concave anteriorly. The upper border, or base, of the bone
brae fused together to form a wedge-shaped bone, which is
The sacrum (Fig. 12.2) consists of five rudimentary verte
tion with ribs and no foramina in the transverse processes.
Note that the lumbar vertebrae have no facets for articula
cesses face laterally.
face medially, and those of the inferior articular pro
The articular surfaces of the superior articular processes
and project posteriorly.
The spinous processes are short, flat, and quadrangular
The transverse processes are long and slender.
The vertebral foramina are triangular.
tant when performing a spinal tap. See page 704).
The laminae are short in a vertical dimension (impor
The pedicles are strong and directed backward.
The body is large and kidney shaped.
(Fig. 12.2):
A typical lumbar vertebra has the following characteristics
Characteristics of a Typical Lumbar Vertebra
erally, as do those of the lumbar vertebrae.
inferior articular processes of the 12th vertebra face lat
rior articular processes face anteriorly and medially. The
posteriorly and laterally, whereas the facets on the infe
The superior articular processes bear facets that face
12 have no facets on the transverse processes).
for articulation with the tubercles of the ribs (T11 and
Costal facets are present on the transverse processes
articulation with the heads of the ribs.
Costal facets are present on the sides of the bodies for
The spines are long and inclined downward.
The vertebral foramen is small and circular.
The body is medium size and heart shaped.
(Fig. 12.2):
A typical thoracic vertebra has the following characteristics
Characteristics of a Typical Thoracic Vertebra
the vertebral vein or veins.
is large, but the foramen transversarium is small and transmits
process, and the process is not bifid. The transverse process
(Fig. 12.3), is so named because it has the longest spinous
vertebra prominens
or
7th cervical vertebra,
The
atlas that has fused with the body of the axis).
superior surface of the body (representing the body of the
that projects from the
odontoid process (dens)
peglike
(Fig. 12.3), has a
or
2nd cervical vertebra,
The
(atlantoaxial joints).
surfaces on its inferior surface for articulation with the axis
and articular
(atlanto-occipital joints)
occipital condyles
lar surfaces on its upper surface for articulation with the
posterior arch. It has a lateral mass on each side with articu
possess a body or a spinous process. It has an anterior and
(Fig. 12.3), does not
or
1st cervical vertebra,
The
The 1st, 2nd, and 7th cervical vertebrae are atypical.
Characteristics of the Atypical Cervical Vertebrae
facets that face inferiorly and anteriorly.
posteriorly and superiorly; the inferior processes have
The superior articular processes have facets that face
687
■
■
atlas
-
axis
■
■
■
■
■
■
■
■
■
■
■
■
-
-
■
■
■
■
■
■
-
■
■
■
■
■
■
■
■
-
-
Sacrum
-
-
canal.
-
-
sacrum; this is usually incomplete and may be limited to
rib. The 5th lumbar vertebra may be incorporated into the
the addition of the 1st lumbar vertebra, which may have a
37). The thoracic vertebrae may be increased in number by
(see page
cervical rib
enth cervical vertebra may possess a
The number of cervical vertebrae is constant, but the sev
Important Variations in the Vertebrae
tures relative to soft tissue injury.
and when noting the precise sites of bony pathologic fea
tebral column is important when interpreting radiographs
Knowledge of the preceding basic anatomy of the ver
fused with the second vertebra.
coccygeal vertebra is usually not fused or is incompletely
base with the lower end of the sacrum (Fig. 12.2). The first
form a single, small triangular bone that articulates at its
The coccyx consists of four vertebrae fused together to
rior and posterior rami of the upper four sacral nerves.
have four foramina on each side for the passage of the ante
The anterior and posterior surfaces of the sacrum each
sacral vertebra.
noid space down as far as the lower border of the second
-
Coccyx
-
-
-
one side. The 1st sacral vertebra may remain
y or
partiall
inferiorly (Fig. 12.4). They are enclosed by a capsule.
ets on the superior surfaces of the lateral masses of the atlas
either side of the foramen magnum superiorly and the fac
formed between the occipital condyles, which are found on
The atlanto-occipital joints are synovial joints that are
Atlanto-Occipital Joints
Joints of the Vertebral Column
apex of the sacrum.
tebra usually projects downward and anteriorly from the
vertebra may be separate. In this condition, the free ver
brae, may have three or five vertebrae. The 1st coccygeal
The coccyx, which usually consists of four fused verte
fail to develop.
sacral canal may be absent because the laminae and spines
lumbar vertebra. A large extent of the posterior wall of the
completely separate from the sacrum and resemble a 6th
-
-
-

688
CHAPTER 12
The Back
basilar part
of occipital bone
anterior
atlanto-occipital
membrane
occipital bone
external occipital protuberance
capsule of
atlanto-occipital
joint
capsule of
atlantoaxial
joint
vertebral artery
anterior
longitudinal
ligament
posterior arch of atlas
vertebral artery
ligamentum flavum
spine of axis
superior band of
cruciate ligament
vertebral artery
transverse
band of
cruciate
ligament
posterior arch of atlas
inferior band of
cruciate ligament
spine of axis
body of axis
odontoid
process of axis
anterior
arch of atlas
apical
ligament
anterior
atlanto-occipital
membrane
basilar part of occipital bone
membrana tectoria
dorsum sellae
membrana tectoria (cut)
superior band of
cruciate ligament (cut)
apical ligament
alar ligament
transverse
process of atlas
accessory
atlantoaxial
ligament
transverse process of axis
membrana tectoria (cut)
inferior band of
cruciate ligament
A
B
C
D
posterior
atlanto-occipital
membrane
transverse band of
cruciate ligament
posterior
atlanto-occipital
membrane
FIGURE 12.4
Anterior view
Flexion, extension, and lateral flexion. No rotation is
Movements
margin of the foramen magnum.
connects the posterior arch of the atlas to the posterior
is similar to the ligamentum flavum (see page 690) and
This membrane
Posterior atlanto-occipital membrane:
atlas to the anterior margin of the foramen magnum.
umn. The membrane connects the anterior arch of the
as a band down the anterior surface of the vertebral col
uation of the anterior longitudinal ligament, which runs
This is a contin
Anterior atlanto-occipital membrane:
Ligaments
of the atlantoaxial joints. Note that the posterior arch of the atlas and the laminae and spine of the axis have been removed.
and posterior view
of the atlanto-occipital joints. Sagittal section
and posterior view
(A)
(B)
(C)
(D)
■
■
-
-
■
■
possible.
Alar ligaments:
margin of the foramen magnum.
nects the apex of the odontoid process to the anterior
This median-placed structure con
Apical ligament:
Ligaments
by capsules.
masses of the bones (Fig. 12.4). The joints are enclosed
of the atlas, and the other two are between the lateral
is between the odontoid process and the anterior arch
The atlantoaxial joints are three synovial joints: one
Atlantoaxial Joints
■
■
-
■
■
These lie one on each side of the apical
sides of the occipital condyles.
ligament and connect the odontoid process to the medial
Basic Anatomy
is composed of fibrocartilage, in
anulus fibrosus
The
sus, and a central part, the nucleus pulposus (Fig. 12.5).
Each disc consists of a peripheral part, the anulus fibro
resilience is gradually lost with advancing age.
vertebrae to move one on the other. Unfortunately, their
is jumping from a height. Their elasticity allows the rigid
the vertebral column is suddenly increased, as when one
permit them to serve as shock absorbers when the load on
adjacent vertebrae (Fig. 12.5). Their physical characteristics
as semielastic discs, which lie between the rigid bodies of
of the vertebral column are greatest. They may be regarded
in the cervical and lumbar regions, where the movements
column below the level of C2 (Fig. 12.5). They are thickest
responsible for one quarter of the length of the vertebral
to the sacrum (C1 has no vertebral body). The discs are
together the vertebral bodies, and they extend from C2
The intervertebral discs are the main structures that bind
Intervertebral Discs
the upper and lower surfaces of the bodies of the vertebrae.
present at the lateral sides of the intervertebral disc between
In the lower cervical region, small synovial joints are
the disc strongly unite the bodies of the two vertebrae.
tebral disc of fibrocartilage (Fig. 12.5). The collagen fibers of
wiched between the plates of hyaline cartilage is an interver
vertebrae are covered by thin plates of hyaline cartilage. Sand
The superior and inferior surfaces of the bodies of adjacent
Joints between Two Vertebral Bodies
(Fig. 12.5).
ies and by synovial joints between their articular processes
other by means of cartilaginous joints between their bod
remainder of the mobile vertebrae articulates with each
With the exception of the first two cervical vertebrae, the
Joints of the Vertebral Column below the Axis
head on the axis.
There can be extensive rotation of the atlas and thus of the
Movements
and the apical, alar, and cruciate ligaments.
It covers the posterior surface of the odontoid process
to the occipital bone just within the foramen magnum.
the posterior longitudinal ligament. It is attached above
This is an upward continuation of
Membrana tectoria:
margin of the foramen magnum.
posterior surface of the body of the axis to the anterior
anterior arch of the atlas. The vertical part runs from the
mass of the atlas and binds the odontoid process to the
attached on each side to the inner aspect of the lateral
verse part and a vertical part. The transverse part is
This ligament consists of a trans
Cruciate ligament:
689
■
■
-
■
■
-
-
-
-
which the collagen fibers are arranged in
ntric lay
conce
attached to the anterior and posterior longitudinal
in alternate sheets. The more peripheral fibers are strongly
adjacent vertebral bodies, and their inclination is reversed
ers or sheets. The collagen bundles pass obliquely between
-
ligaments of the vertebral column.
an ovoid mass of gelatinous material containing a large
in children and adolescents is
nucleus pulposus
The
thoracic
superior
articular
process
inferior
articular
process
joint between
bodies
(cartilaginous)
superior articular
process
inferior articular
process
joint between
articular processes
(synovial)
joint between
bodies (cartilaginous)
lumbar
dura mater
arachnoid mater
cauda equina
internal vertebral
veins
nucleus pulposus
anulus fibrosus
intervertebral
disc
spine
intervertebral foramen
spinal nerve
posterior
longitudinal ligament
body
anulus fibrosus
nucleus pulposus
anterior longitudinal ligament
ligamentum flavum
pedicle
interspinous
ligament
A
B
C
joint between
bodies
(cartilaginous
and synovial)
joint between
articular
processes
(synovial)
spine
cervical
joint between articular
processes (synovial)
inferior articular process
superior articular
process
articular
process
articular
process
joint between
bodies
(cartilaginous)
process
thoracic
inferior articular
process
joint between
articular processes
(synovial)
joint between
bodies (cartilagi
lumbar
dura mater
arachnoid mater
cauda equina
internal vertebral
veins
nucleus pulposus
anulus fibrosus
intervertebral
disc
spine
intervertebral foramen
spinal nerve
posterior
longitudinal ligament
body
anulus fibrosus
nucleus pulposus
anterior longitudinal ligame
ligamentum flavum
pedicle
interspinous
A
B
C
joint between
bodies
(cartilaginous
and synovial)
j
articular
processes
(synovial)
spine
cervical
joint between articular
processes (synovial)
inferior articular process
supraspinous
ligament
FIGURE 12.5
A.
intervertebral foramen and the intervertebral disc.
vertebrae showing ligaments and intervertebral discs. Note the relationship between the emerging spinal nerve in an
Sagittal section through three lumbar
from above showing the relationship between intervertebral disc and cauda equina.
Third lumbar vertebra seen
Joints in the cervical, thoracic, and lumbar regions of the vertebral column. B.
C.

690
CHAPTER 12
With advancing age, the water content of the nucleus
nerve, or even the spinal cord (see page 701).
where it may press on the spinal nerve roots, the spinal
pulposus to herniate and protrude into the vertebral canal,
the anulus fibrosus and it ruptures, allowing the nucleus
lus fibrosus. Sometimes, the outward thrust is too great for
accommodated by the resilience of the surrounding anu
become flattened. The outward thrust of the nucleus is
tebral column causes the semifluid nucleus pulposus to
A sudden increase in the compression load on the ver
vertebral column.
or posteriorly on another, as in flexion and extension of the
change shape and permits one vertebra to rock anteriorly
The semifluid nature of the nucleus pulposus allows it to
Function of the Intervertebral Discs
first two cervical vertebrae or in the sacrum or coccyx.
plates of hyaline cartilage. No discs are found between the
cent vertebrae that abut onto the disc are covered with thin
The superior and inferior surfaces of the bodies of adja
margin of the disc.
ated slightly nearer to the posterior than to the anterior
few cartilage cells. It is normally under pressure and situ
amount of water, a small number of collagen fibers, and a
The Back
-
-
-
-
pulposus diminishes and is replaced by fibrocartilage. The
pinous ligaments are greatly thickened to form the strong
In the cervical region, the supraspinous and inters
inae of adjacent vertebrae.
(Fig. 12.5): This connects the lam
Ligamentum flavum
transverse processes.
These run between adjacent
Intertransverse ligaments:
cent spines.
(Fig. 12.5): This connects adja
Interspinous ligament
the tips of adjacent spines.
(Fig. 12.5): This runs between
Supraspinous ligament
Ligaments
rounded by a capsular ligament.
are covered with hyaline cartilage, and the joints are sur
cesses of adjacent vertebrae (Fig. 12.5). The articular facets
vial joints between the superior and inferior articular pro
The joints between two vertebral arches consist of syno
Joints between Two Vertebral Arches
of movement to take place between them.
firmly together but at the same time permit a small amount
borders of the discs. These ligaments hold the vertebrae
ment is weak and narrow and is attached to the posterior
bodies and to the intervertebral discs. The posterior liga
is strongly attached to the front and sides of the vertebral
(Figs. 12.5 and 12.14). The anterior ligament is wide and
faces of the vertebral column from the skull to the sacrum
as continuous bands down the anterior and posterior sur
run
posterior longitudinal ligaments
anterior
The
Ligaments
longer possible to distinguish the nucleus from the anulus.
stress. In old age, the discs are thin and less elastic, and it is no
anulus cannot always contain the nucleus pulposus under
collagen fibers of the anulus degenerate and, as a result, the
and
-
-
-
-
-
■
■
■
■
-
■
■
■
■
-
-
by the small meningeal branches of each spinal nerve
The joints between the vertebral bodies are innervated
Nerve Supply of Vertebral Joints
attached to the cervical spines in between.
ance of the skull, with its anterior border being strongly
the 7th cervical vertebra to the external occipital protuber
The latter extends from the spine of
ligamentum nuchae.
-
(Fig. 12.6). The nerve arises from the spinal nerve as it exits
between the articular processes are innervated by branches
the meninges, ligaments, and intervertebral discs. The joints
bral canal through the intervertebral foramen and supplies
from the intervertebral foramen. It then re-enters the verte-
from the posterior rami of the spinal nerves (Fig. 12.6).
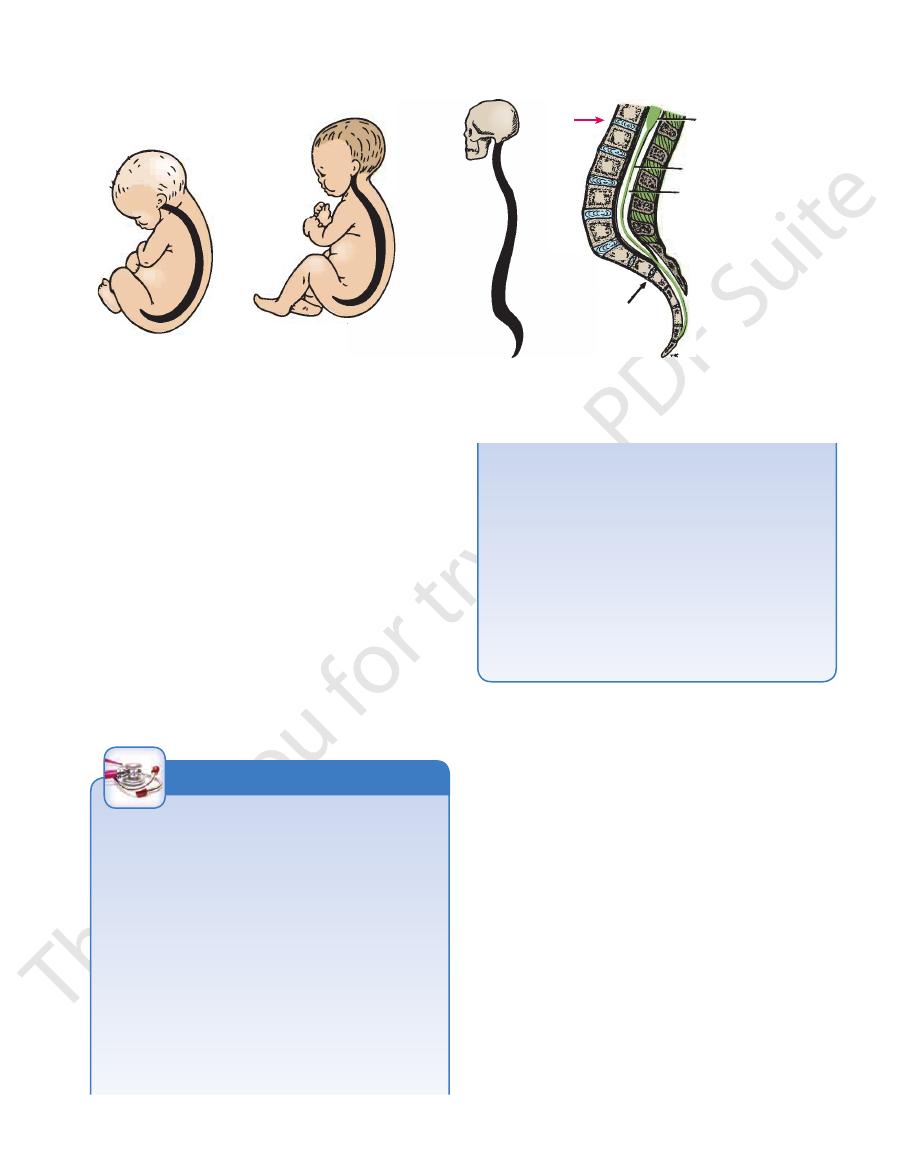
following regional curves: cervical, posterior concavity;
tebral column therefore exhibits in the sagittal plane the
In the adult in the standing position (Fig. 12.7), the ver
shape of the vertebral bodies and the intervertebral discs.
of these secondary curves results in a modification in the
column becomes concave posteriorly. The development
result of muscular activity, the lumbar part of the vertebral
the first year, when the child begins to stand upright as the
becomes concave posteriorly (Fig. 12.7). Toward the end of
muscular activity, the cervical part of the vertebral column
or her head and keep it poised on the vertebral column by
angle appears. After birth, when the child is able to raise his
rior concavity. As development proceeds, the lumbosacral
In the fetus, the vertebral column has one continuous ante
Curves in the Sagittal Plane
Curves of the Vertebral Column
receive nerve fibers from two adjacent spinal nerves.
It should be noted that the joints of any particular level
-
-
articular branch
spinous
process
thoracic
spinal
nerve
posterior ramus
of spinal nerve
anterior ramus
of spinal nerve
gray ramus
communicans
white ramus
communicans
sympathetic
trunk
meningeal
branch of
spinal nerve
anterior ramus
of spinal nerve
posterior
ramus of
spinal nerve
T4
FIGURE 12.6
The innervation of vertebral joints. At any
two adjacent spinal nerves.
particular vertebral level, the joints receive nerve fibers from
Basic Anatomy
691
newborn infant
baby holds head up steadily
(3–4 months)
spinal cord
filum terminale
subarachnoid space
filled with cerebrospinal fluid
adult
A
B
C
D
L1
2
3
4
5
S1
2
3
4
5
FIGURE 12.7
A–C.
present superior and inferior to such a curvature.
thoracic convexity. Slight compensatory curves are always
right-handed persons will often have a slight right-sided
predominant use of one of the upper limbs. For example,
tebral column. This is normal and is usually caused by the
of minor lateral curves in the thoracic region of the ver
In late childhood, it is common to find the development
Curves in the Coronal Plane
anterior concavity.
a gradual return of the vertebral column to a continuous
intervertebral discs atrophy, resulting in a loss of height and
an attempt to preserve their center of gravity. In old age, the
women tend to increase the posterior lumbar concavity in
pregnancy, with the increase in size and weight of the fetus,
and sacral, posterior convexity. During the later months of
thoracic, posterior convexity; lumbar, posterior concavity;
bottom arrow
border of the body of the second sacral vertebra (
), and the subarachnoid space ends at the lower
top arrow
level of the lower border of the body of the first lumbar vertebra (
In the adult, the lower end of the spinal cord lies at the
Curves of the vertebral column at different ages. D.
).
-
increase in the weight of the abdominal contents, as with the
degree of movement possible between adjacent vertebrae.
one another by strong ligaments that severely limit the
bral discs. The vertebrae are held in position relative to
positioned one on the other and separated by interverte
column consists of several separate vertebrae accurately
As has been seen in the previous sections, the vertebral
Movements of the Vertebral Column
by disease of the vertebral column such as spondylolisthesis
gravid uterus or a large ovarian tumor, or it may be caused
(see page 693). The possibility that it is a postural compensa-
tion for a kyphosis in the thoracic region or a disease of the
hip joint (congenital dislocation) must not be overlooked.
Scoliosis is a lateral deviation of the vertebral column.
This is most commonly found in the thoracic region and may
be caused by muscular or vertebral defects. Paralysis of
muscles caused by poliomyelitis can cause severe scoliosis.
The presence of a congenital hemivertebra can cause scolio-
sis. Often, scoliosis is compensatory and may be caused by a
short leg or hip disease.
-
Nevertheless, the
f all these movements gives
summation o
is a combination of all these movements.
Circumduction
least extensive in the lumbar region.
is a twisting of the vertebral column. This is
Rotation
regions but restricted in the thoracic region.
the other side. It is extensive in the cervical and lumbar
is the bending of the body to one or
Lateral flexion
region.
cal and lumbar regions but restricted in the thoracic
posterior movement. Both are extensive in the cervi
is a
extension
is an anterior movement, and
Flexion
sion, lateral flexion, rotation, and circumduction.
The following movements are possible: flexion, exten
mobility.
the vertebral column as a whole a remarkable degree of
-
■
■
-
■
■
■
■
■
■
Abnormal Curves of the Vertebral Column
kyphosis of the upper thoracic region. The person is said to be
study or work over a low desk can lead to a gently curved
Kyphosis is an exaggeration in the sagittal curvature present
in the thoracic part of the vertebral column. It can be caused
by muscular weakness or by structural changes in the verte-
bral bodies or by intervertebral discs. In sickly adolescents,
for example, where the muscle tone is poor, long hours of
“round-shouldered.” Crush fractures or tuberculous destruc-
tion of the vertebral bodies leads to acute angular kyphosis
of the vertebral column. In the aged, osteoporosis (abnormal
rarefaction of bone) and/or degeneration of the intervertebral
discs leads to senile kyphosis, involving the cervical, tho-
racic, and lumbar regions of the column.
Lordosis is an exaggeration in the sagittal curvature
present in the lumbar region. Lordosis may be caused by an
C L I N I C A L N O T E S
(continued)
692
CHAPTER 12
the scalenus anterior and medius and the trapezius and
The Back
sternocleidomastoid muscles. Rotation is produced by
rotation is produced by the
thoracic region,
In the
the other side.
the sternocleidomastoid on one side and the splenius on
unilateral contraction of the semispinalis and rotatores
muscles and the oblique muscles of the anterolateral
in this movement. Rotation is produced by the rotatores
lateral abdominal wall. The psoas may also play a part
tus lumborum, and the oblique muscles of the antero
is produced by the postvertebral muscles, the quadra
produced by the postvertebral muscles. Lateral flexion
rectus abdominis and the psoas muscles. Extension is
flexion is produced by the
lumbar region,
In the
eral abdominal wall.
muscles, assisted by the oblique muscles of the anterolat-
-
-
abdominal wall.
muscles (see page 693). Lateral flexion is produced by
toid muscles. Extension is produced by the postvertebral
longus cervicis, scalenus anterior, and sternocleidomas
flexion is produced by the
cervical region,
In the
ribs or fasciae.
abdominal wall muscles, are attached to the skull or to the
whereas others, such as the sternocleidomastoid and the
cles, many of which are attached directly to the vertebrae,
The vertebral column is moved by numerous mus
range of rotation of the atlas and thus of the head on the axis.
allow a wide
atlantoaxial joints
extension of the head. The
permit extensive flexion and
atlanto-occipital joints
The
and the sternum severely restrict the range of movement.
cesses. In the thoracic region, the ribs, the costal cartilages,
tebral discs and the shape and direction of the articular pro
the column largely depend on the thickness of the interver
The type and range of movements possible in each region of
-
-
-
-
Dislocations of the Vertebral Column
It is possible for nontraumatic compression fractures to
body. Pieces of the vertebral body are commonly forced back into
ruption of the intervertebral disc and breakup of the vertebral
If the neck is slightly flexed, the
the atlas to be disrupted and the lateral masses to be displaced
excessive vertical force applied from above will cause the ring of
umn (Fig. 12.8). In the cervical region, with the neck straight, an
Vertical compression fractures occur in the cervical and lumbar
vertebrae involved are unstable, and the spinal cord is usually
the site is usually where maximum mobility occurs, as in the
sively flexed and twisted on the lower vertebra. Here again,
Fracture dislocations are usually caused by a combination of a
lateral flexion in addition to excessive flexion, the lateral part of
bral ligaments remain intact so that vertebral displacement and
Bilateral cervical dislocations are almost always associated
size of the vertebral canal allows the spinal cord to escape dam
the processes. In the thoracic and lumbar regions, dislocations
Dislocations without fracture occur only in the cervical region
because the inclination of the articular processes of the cervical
vertebrae permits dislocation to take place without fracture of
can occur only if the vertically placed articular processes are
fractured.
Dislocations commonly occur between the 4th and 5th or 5th
and 6th cervical vertebrae, where mobility is greatest. In unilat-
eral dislocations, the inferior articular process of one vertebra is
forced forward over the anterior margin of the superior articular
process of the vertebra below. Because the articular processes
normally overlap, they become locked in the dislocated position.
The spinal nerve on the same side is usually nipped in the inter-
vertebral foramen, producing severe pain. Fortunately, the large
-
age in most cases.
with severe injury to the spinal cord. Death occurs immediately
if the upper cervical vertebrae are involved because the respira-
tory muscles, including the diaphragm (phrenic nerves C3 to 5),
are paralyzed.
Fractures of the Vertebral Column
Fractures of the Spinous Processes, Transverse
Processes, or Laminae
Fractures of the spinous processes, transverse processes, or
laminae are caused by direct injury or, in rare cases, by severe
muscular activity.
Anterior and Lateral Compression Fractures
Anterior compression fractures of the vertebral bodies are usu-
ally caused by an excessive flexion compression type of injury
and take place at the sites of maximum mobility or at the junction
of the mobile and fixed regions of the column. It is interesting to
note that the body of a vertebra in such a fracture is crushed,
whereas the strong posterior longitudinal ligament remains
intact. The vertebral arches remain unbroken and the interverte-
spinal cord injury do not occur. When injury causes excessive
the body is also crushed.
Fracture Dislocations
flexion and rotation type of injury; the upper vertebra is exces-
lumbar region, or at the junction of the mobile and fixed region
of the column, as in the lower lumbar vertebrae. Because the
articular processes are fractured and the ligaments are torn, the
severely damaged or severed, with accompanying paraplegia.
Vertical Compression Fractures
regions, where it is possible to fully straighten the vertebral col-
laterally (Jefferson’s fracture).
lower cervical vertebrae remain in a straight line and the com-
pression load is transmitted to the lower vertebrae, causing dis-
the spinal cord.
occur in severe cases of osteoporosis and for pathologic frac-
tures to take place.
In the straightened lumbar region, an excessive force from
below can cause the vertebral body to break up, with protrusion
of fragments posteriorly into the spinal canal.
C L I N I C A L N O T E S
(continued)