Basic Anatomy
191
vitelline duct
cephalic limb of midgut loop
caudal limb of midgut loop
cecum
appendix
cecum
appendix
ascending colon
ileum
appendix
cecum
1
2
3
4
5
6
FIGURE 5.43
Stages in the development of the cecum and appendix. The final stages of development (stages 4, 5, and 6)
take place after birth.
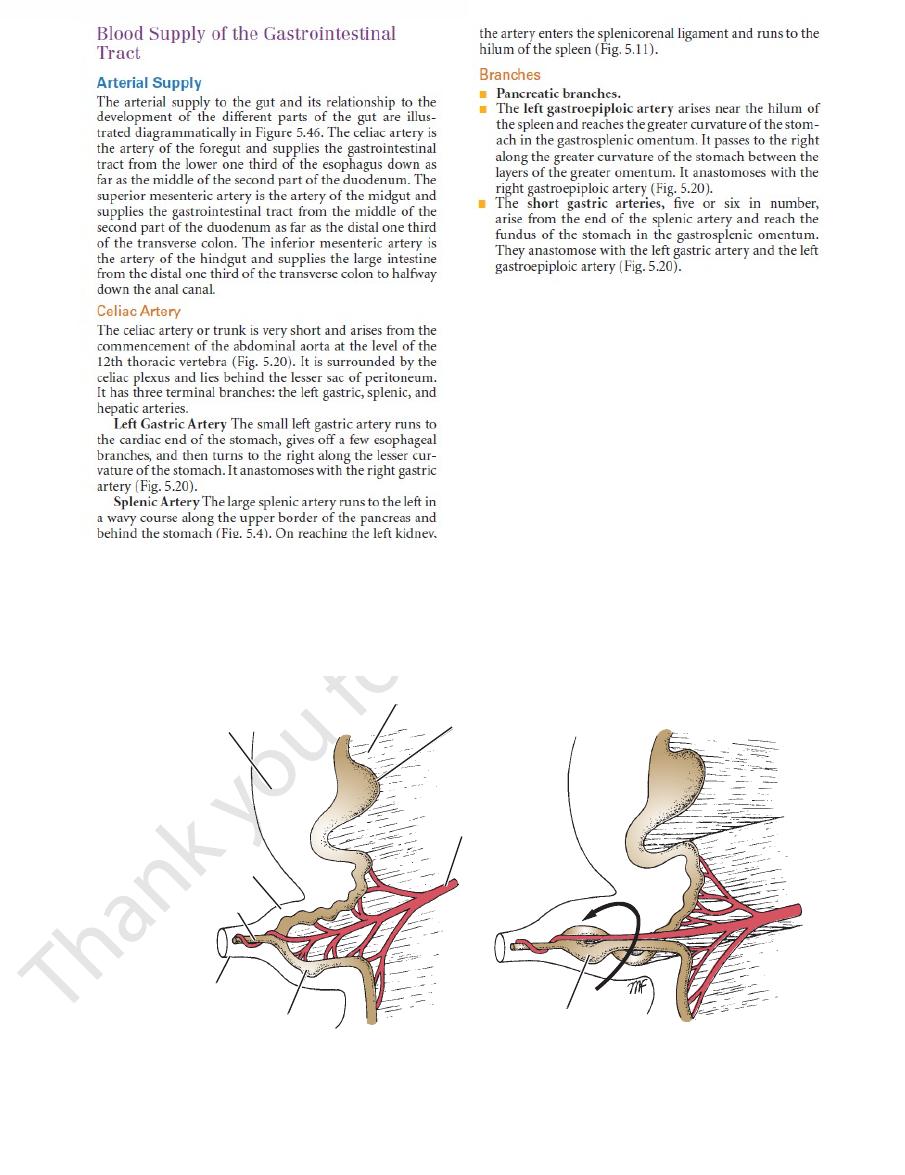
abdominal cavity
dorsal mesentery
greater curvature
of stomach
remains of
extraembryonic coelom
vitelline duct
umbilical cord
developing cecum
superior
mesenteric
artery
developing cecum
A
B
FIGURE 5.44
Left-side views of the counterclockwise 90° rotation of the midgut loop while it is in the extraembryonic coelom
gastroepiploic artery (Fig. 5.20).
They anastomose with the left gastric artery and the left
fundus of the stomach in the gastrosplenic omentum.
arise from the end of the splenic artery and reach the
five or six in number,
short gastric arteries,
The
right gastroepiploic artery (Fig. 5.20).
layers of the greater omentum. It anastomoses with the
along the greater curvature of the stomach between the
ach in the gastrosplenic omentum. It passes to the right
the spleen and reaches the greater curvature of the stom
arises near the hilum of
left gastroepiploic artery
The
Pancreatic branches.
Branches
hilum of the spleen (Fig. 5.11).
the artery enters the splenicorenal ligament and runs to the
in the umbilical cord.
■
■
■
■
-
■
■
192
CHAPTER 5
ach. It anastomoses with the left gastric artery (Fig. 5.20).
lesser omentum along the lesser curvature of the stom
the upper border of the pylorus and runs to the left in the
arises from the hepatic artery at
right gastric artery
The
Branches
ply the corresponding lobes of the liver.
porta hepatis, it divides into right and left branches to sup
left of the bile duct and in front of the portal vein. At the
front of the opening into the lesser sac and is placed to the
layers of the lesser omentum (Figs. 5.7 and 5.11). It lies in
forward and to the right and then ascends between the
The medium-size hepatic artery* runs
Hepatic Artery.
The Abdomen: Part II—The Abdominal Cavity
-
■
■
-
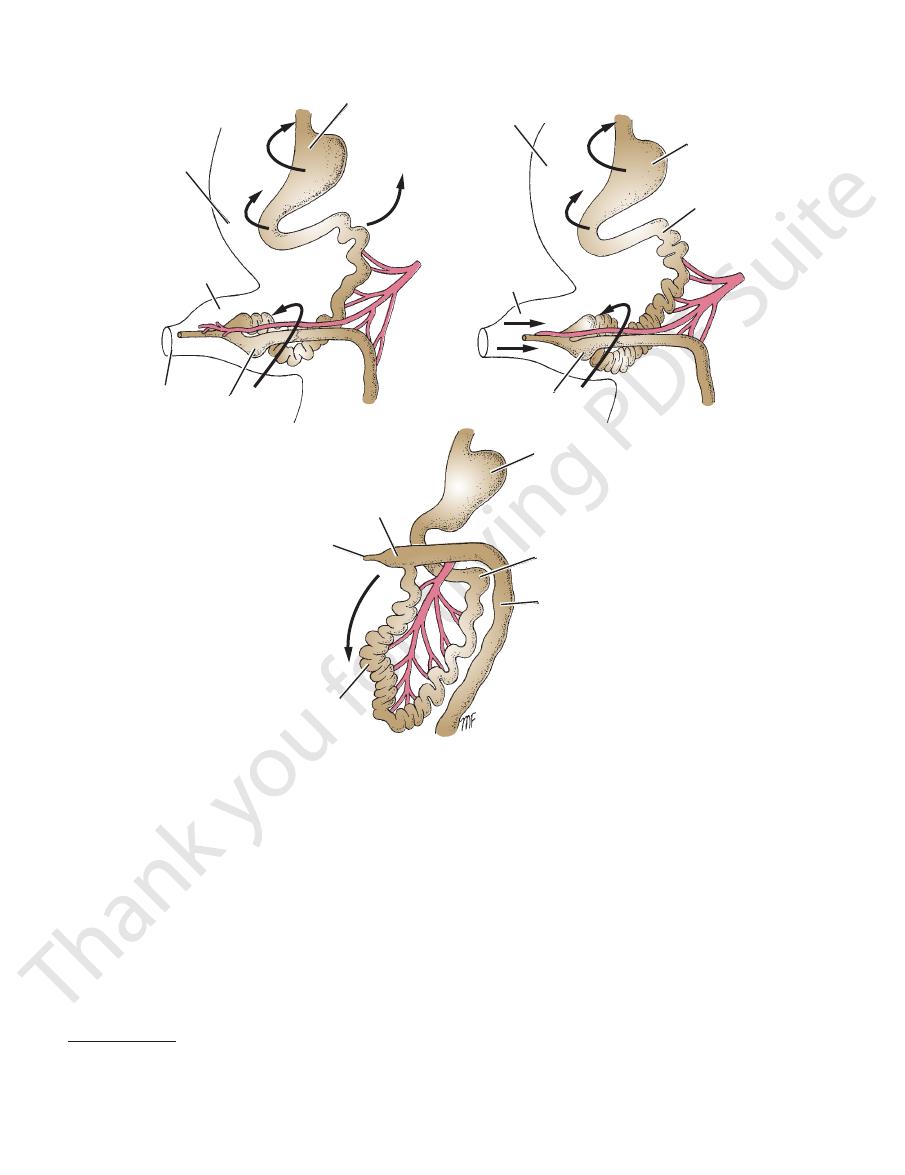
stomach
abdominal cavity
remains of
extraembryonic coelom
umbilical cord
cecum
superior
mesenteric
artery
abdominal cavity
extraembryonic
coelom
stomach
jejunum
superior
mesenteric
artery
cecum
stomach
cecum
developing appendix
ileum
jejunum
colon
descent of cecum
A
B
C
FIGURE 5.45
The descent of the cecum takes place later.
abdominal cavity.
Left-side views of the counterclockwise 180° rotation of the midgut loop as it is withdrawn into the
A, B:
C:
below the celiac artery (Fig. 5.32) and runs downward and
colon. It arises from the front of the abdominal aorta just
appendix, the ascending colon, and most of the transverse
the duodenum, the jejunum, the ileum, the cecum, the
The superior mesenteric artery supplies the distal part of
Superior Mesenteric Artery
which runs to the neck of the gallbladder (Fig. 5.47).
cystic artery,
The right hepatic artery usually gives off the
enter the porta hepatis.
left hepatic arteries
right
The
(Figs. 5.4 and 5.20).
ond part of the duodenum and the head of the pancreas
that descends between the sec
creaticoduodenal artery
superior pan
layers of the greater omentum and the
along the greater curvature of the stomach between the
that runs
right gastroepiploic artery
divides into the
descends behind the first part of the duodenum. It
is a large branch that
gastroduodenal artery
The
, which is the remainder of the artery.
proper
hepatic artery
its origin to the gastroduodenal branch, and the
, which extends from
common hepatic artery
divided into the
*For purposes of description, the hepatic artery is sometimes
■
■
-
-
■
■
and
Basic Anatomy
that anastomoses with
superior branch
It gives rise to a
passes downward and to the right.
ileocolic artery
The
and divides into ascending and descending branches.
artery. It passes to the right to supply the ascending colon
is often a branch of the ileocolic
right colic artery
The
into right and left branches.
mesocolon to supply the transverse colon and divides
runs forward in the transverse
middle colic artery
The
part of the duodenum.
the pancreas. It supplies the pancreas and the adjoining
der of the third part of the duodenum and the head of
right as a single or double branch along the upper bor
passes to the
inferior pancreaticoduodenal artery
The
Branches
its own ileocolic branch.
intestine and ends by anastomosing with the ileal branch of
the right between the layers of the mesentery of the small
the third part of the duodenum. It continues downward to
to the right behind the neck of the pancreas and in front of
193
■
■
-
■
■
■
■
■
■
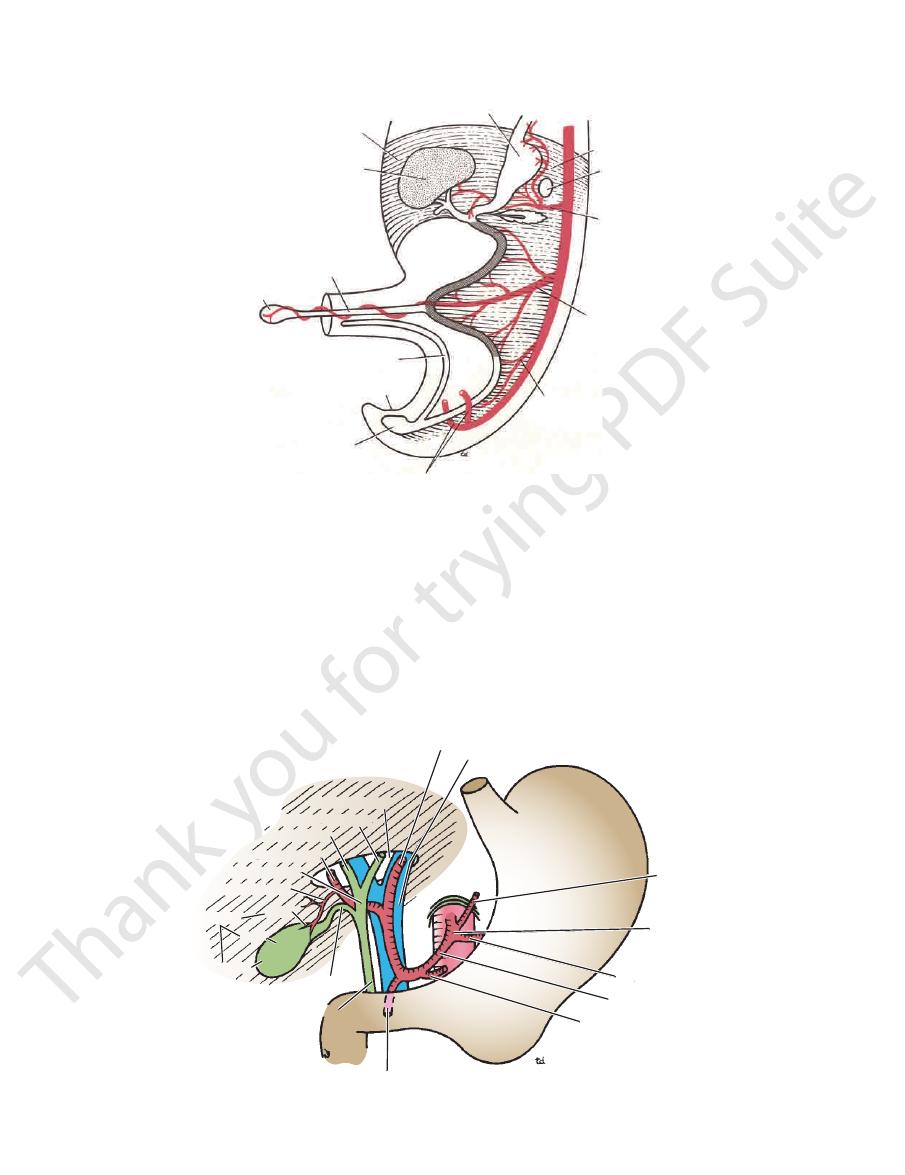
ventral mesentery
liver
vitelline duct
yolk sac
allantois
proctodeum
cloaca
umbilical arteries
stomach
dorsal mesentery
spleen
foregut artery
(celiac artery)
midgut artery
(superior mesenteric
artery)
hindgut artery (inferior
mesenteric artery)
FIGURE 5.46
Formation of the midgut loop (
axis for the future rotation of the midgut loop.
). Note how the superior mesenteric artery and the vitelline duct form an
shaded
left hepatic artery
gastroduodenal artery
portal vein
porta hepatis
left hepatic duct
right hepatic duct
common hepatic duct
neck
right hepatic artery
cystic artery
gallbladder
body
fundus
cystic duct
left gastric artery
celiac artery
splenic artery
hepatic artery
right gastric artery
bile duct
FIGURE 5.47
Structures entering and leaving the porta hepatis.

194
CHAPTER 5
moses less freely with the superior rectal artery (Fig. 5.36).
the superior mesenteric artery, and it ends where it anasto
junction, where it anastomoses with the ileal branches of
This begins at the ileocecal
marginal artery.
called the
margin of the large intestine forms a single arterial trunk
The anastomosis of the colic arteries around the concave
Marginal Artery
inferior rectal arteries.
anal canal and anastomoses with the middle rectal and
The artery supplies the rectum and upper half of the
artery. It descends into the pelvis behind the rectum.
rior mesenteric artery as it crosses the left common iliac
is a continuation of the infe
superior rectal artery
The
supply the descending and sigmoid colon.
are two or three in number and
sigmoid arteries
The
divides into ascending and descending branches.
flexure, and the upper part of the descending colon. It
plies the distal third of the transverse colon, the left colic
runs upward and to the left and sup
left colic artery
The
Branches
iliac artery. Here, it becomes the superior rectal artery.
runs downward and to the left and crosses the left common
1.5 in. (3.8 cm) above its bifurcation (Fig. 5.36). The artery
of the anal canal. It arises from the abdominal aorta about
colon, the sigmoid colon, the rectum, and the upper half
the transverse colon, the left colic flexure, the descending
The inferior mesenteric artery supplies the distal third of
Inferior Mesenteric Artery
minal arcades, small straight vessels supply the intestine.
supply the jejunum than supply the ileum. From the ter
second, third, and fourth series of arcades. Fewer arcades
Branches from the arcades divide and unite to form a
unite with adjacent branches to form a series of arcades.
(Fig. 5.32). Each artery divides into two vessels, which
arise from the left side of the superior mesenteric artery
are 12 to 15 in number and
jejunal and ileal branches
The
of the posterior cecal artery (Fig. 5.33).
is a branch
appendicular artery
rior cecal arteries;
poste
anterior
The inferior branch gives rise to the
tomoses with the end of the superior mesenteric artery.
that anas
inferior branch
the right colic artery and an
The Abdomen: Part II—The Abdominal Cavity
-
and
-
the
■
■
-
■
■
-
■
■
■
■
-
-
the foregut (which includes the distal third of the esophagus,
mesenteric, and pancreatic veins.
It receives the short gastric, left gastroepiploic, inferior
neck of the pancreas to form the portal vein (Fig. 5.48).
It unites with the superior mesenteric vein behind the
and passes to the right in the splenicorenal ligament.
This vein leaves the hilum of the spleen
Splenic vein:
tric vein, right gastric vein, and cystic veins.
vein are the splenic vein, superior mesenteric vein, left gas
The tributaries of the portal
Tributaries of the Portal Vein
tum, see Figures 5.7 and 5.11.
For the relations of the portal vein in the lesser omen
soids within the liver.
organs it drains and ends by emptying its blood into sinu
The portal circulation begins as a capillary plexus in the
where it divides into right and left terminal branches.
front of the opening into the lesser sac to the porta hepatis,
lesser omentum (Figs. 5.7 and 5.11). It then runs upward in
right, behind the first part of the duodenum, and enters the
rior mesenteric and splenic veins (Fig. 5.48). It ascends to the
behind the neck of the pancreas by the union of the supe
cava. The portal vein is about 2 in. (5 cm) long and is formed
blood passes into the hepatic veins that join the inferior vena
vein enters the liver and breaks up into sinusoids, from which
blood from the spleen, pancreas, and gallbladder. The portal
the esophagus to halfway down the anal canal; it also drains
nal part of the gastrointestinal tract from the lower third of
The portal vein (Fig. 5.22) drains blood from the abdomi
Portal Vein (Hepatic Portal Vein)
inferior mesenteric arteries.
to the branches of the celiac artery and the superior and
vein, but the veins forming the distal tributaries correspond
The proximal tributaries drain directly into the portal
portal venous system.
tinal tract and its accessory organs drains to the liver by the
The venous blood from the greater part of the gastrointes
Venous Drainage
which represents the fused pair of
the stomach, and the proximal half of the duodenum) is sup-
plied by a number of vessels that fuse to form a single trunk,
the celiac artery (Fig. 5.46). It is interesting to note that this
artery also supplies the liver and pancreas, which are glan-
dular derivatives of this part of the gut. The spleen is also
supplied by the same artery, which is not surprising, since
this organ develops in the dorsal mesentery of the foregut;
the artery to the spleen runs in the splenicorenal ligament.
Midgut Artery
The midgut, which extends from halfway along the second
part of the duodenum to the left colic flexure, is supplied by the
superior mesenteric artery,
vitelline arteries (Fig. 5.46).
Hindgut Artery
The hindgut, which extends from the left colic flexure to half-
way down the anal canal, is supplied by the inferior mesen-
teric artery (Fig. 5.46). This represents a number of ventral
branches of the aorta that fuse to form a single artery.
-
-
-
-
-
-
■
■
Explanation for the Blood Supply to the
and esophageal branches from the aorta. The caudal end of
and the cervical and thoracic portions of the esophagus are
Gastrointestinal Tract
Foregut Arteries
The cephalic end of the foregut (which includes the pharynx)
supplied by the ascending pharyngeal arteries, palatine arter-
ies, superior and inferior thyroid arteries, bronchial arteries,
E M B R Y O L O G I C N O T E S
(continued)
Basic Anatomy
(Fig. 5.22).
der directly into the liver or join the portal vein
These veins either drain the gallblad
Cystic veins:
into the portal vein (Fig. 5.22).
the lesser curvature of the stomach and drains directly
This vein drains the right portion of
Right gastric vein:
(Fig. 5.22).
of the esophagus. It opens directly into the portal vein
the lesser curvature of the stomach and the distal part
This vein drains the left portion of
Left gastric vein:
pancreaticoduodenal, and right gastroepiploic veins.
jejunal, ileal, ileocolic, right colic, middle colic, inferior
behind the neck of the pancreas (Fig. 5.48). It receives the
the third part of the duodenum and joins the splenic vein
of the mesentery of the small intestine. It passes in front of
This vein ascends in the root
Superior mesenteric vein:
rior rectal veins, the sigmoid veins, and the left colic vein.
the body of the pancreas (Fig. 5.48). It receives the supe
posterior abdominal wall and joins the splenic vein behind
This vein ascends on the
Inferior mesenteric vein:
195
■
■
-
■
■
■
■
■
■
■
■
-
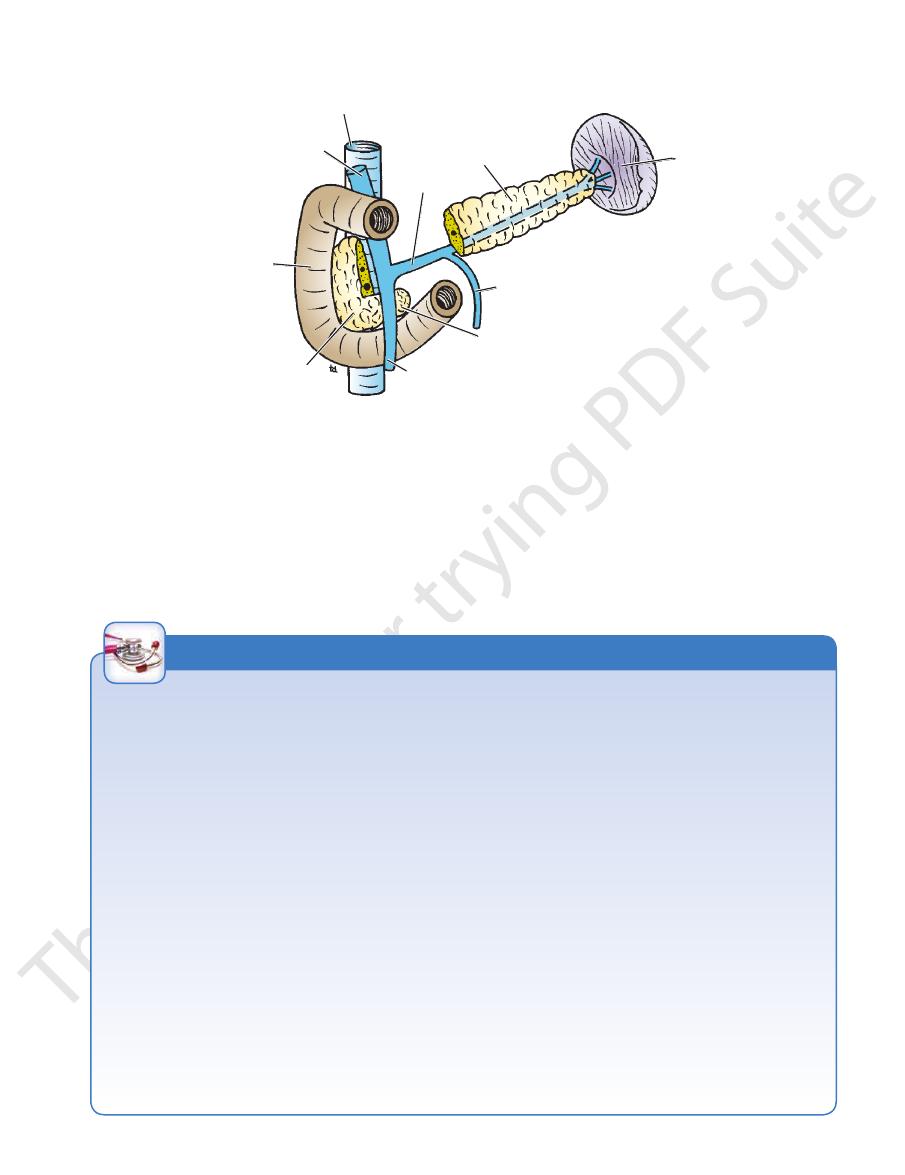
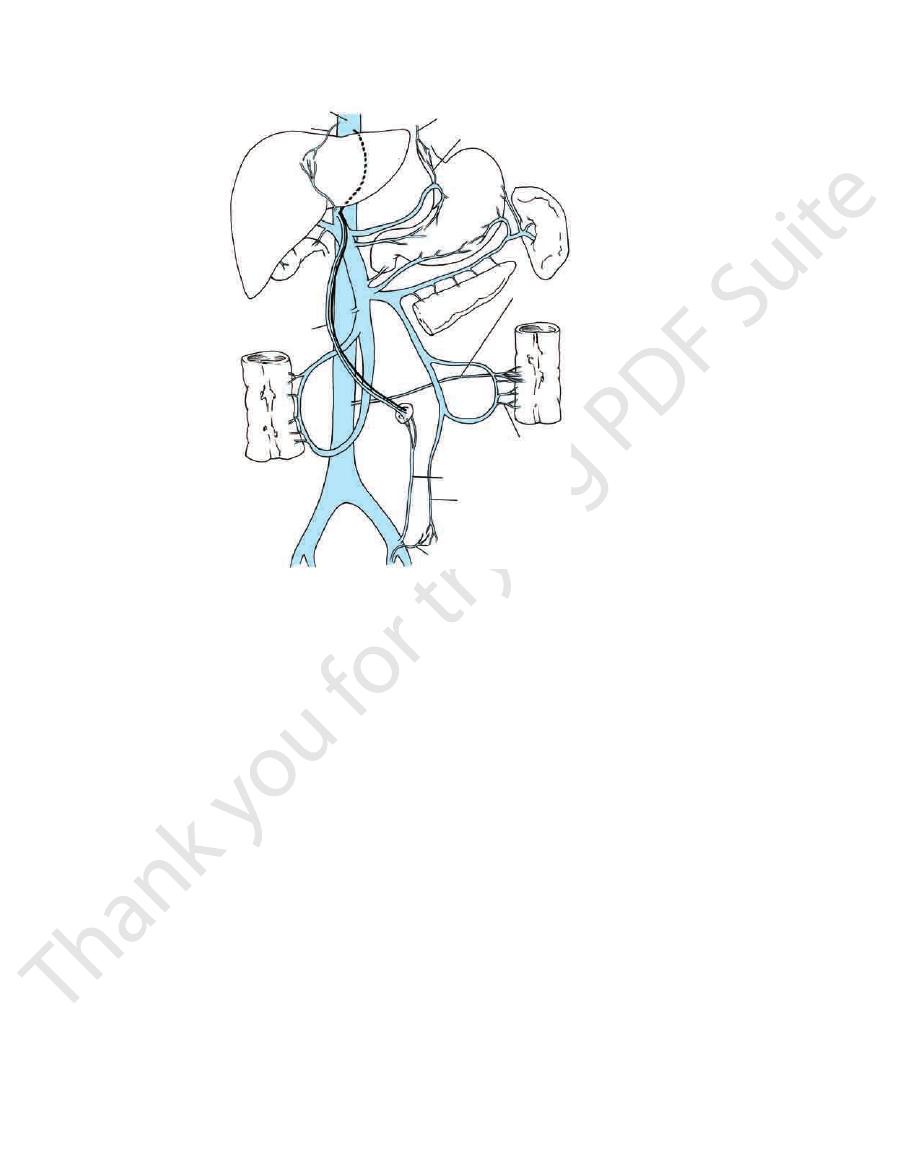
inferior vena cava
portal vein
duodenum
head of pancreas
superior mesenteric vein
uncinate process of pancreas
inferior mesenteric vein
spleen
body of pancreas
splenic vein
FIGURE 5.48
Formation of the portal vein behind the neck of the pancreas.
Portal–Systemic Anastomoses
whereas the left lobe plus the quadrate and caudate lobes
right lobe of the liver receives blood mainly from the intestine,
leads to streaming of the blood flow in the portal vein. The
vein with the superior mesenteric vein to form the portal vein
via the hepatic artery. The wide angle of union of the splenic
remaining 30% is oxygenated blood, which passes to the liver
The portal vein conveys about 70% of the blood to the liver. The
may be anastomosed to the left renal vein after removing the
cava behind the entrance into the lesser sac. The splenic vein
the lesser omentum, to the anterior wall of the inferior vena
involve the anastomosis of the portal vein, because it lies within
for the treatment of portal hypertension may
accompanied by congestive enlargement of the spleen.
Enlargement of the portal–systemic connections is frequently
list of portal–systemic anastomoses should be remembered.
Portal hypertension is a common clinical condition; thus, the
mose with the middle and inferior rectal veins (systemic trib
esophageal veins draining the middle third of the esophagus
At the lower third of the esophagus, the esophageal branches
the portal and systemic systems, and they become important
route. However, other, smaller communications exist between
Under normal conditions, the portal venous blood traverses
the liver and drains into the inferior vena cava of the systemic
venous circulation by way of the hepatic veins. This is the direct
when the direct route becomes blocked (Fig. 5.49).
These communications are as follows:
■
■
of the left gastric vein (portal tributary) anastomose with the
into the azygos veins (systemic tributary).
■
■
Halfway down the anal canal, the superior rectal veins (portal
tributary) draining the upper half of the anal canal anasto-
-
utaries), which are tributaries of the internal iliac and internal
pudendal veins, respectively.
■
■
The paraumbilical veins connect the left branch of the portal
vein with the superficial veins of the anterior abdominal wall
(systemic tributaries). The paraumbilical veins travel in the
falciform ligament and accompany the ligamentum teres.
■
■
The veins of the ascending colon, descending colon, duode-
num, pancreas, and liver (portal tributary) anastomose with
the renal, lumbar, and phrenic veins (systemic tributaries).
Portal Hypertension
Portacaval shunts
spleen.
Blood Flow in the Portal Vein and Malignant Disease
receive blood from the stomach and the spleen. This distribu-
tion of blood may explain the distribution of secondary malig-
nant deposits in the liver.
C L I N I C A L N O T E S
196
CHAPTER 5
extends to the left to reach the left hemidiaphragm. The
it from the pleura, lungs, pericardium, and heart. The liver
right costal margin, and the right hemidiaphragm separates
The greater part of the liver is situated under cover of the
the abdominal cavity just beneath the diaphragm (Fig. 5.1).
The liver is soft and pliable and occupies the upper part of
conveyed to the duodenum by the biliary ducts.
blood corpuscles and secretes bile salts; these together are
duces bile pigments from the hemoglobin of worn-out red
stance, and has an important detoxicating function. It pro
The liver synthesizes heparin, an anticoagulant sub
the intestine.
that have gained entrance to the blood from the lumen of
of the blood, removing bacteria and other foreign particles
to carbohydrate, fat, and protein metabolism; and filtration
tinal tract; involvement in many metabolic activities related
duction and secretion of bile, which is passed into the intes
variety of functions. Three of its basic functions are pro
The liver is the largest gland in the body and has a wide
Location and Description
Gastrointestinal Tract
tine; these are absent in the large intestine (Fig. 5.50).
are found in the mucous membrane of the small intes
Peyer’s patches
Aggregations of lymphoid tissue called
which are absent in the large intestine.
The mucous membrane of the small intestine has villi,
in the large intestine.
which are absent
plicae circulares,
manent folds, called
The mucous membrane of the small intestine has per
Internal Differences
the large intestine is sacculated (Fig. 5.50).
The wall of the small intestine is smooth, whereas that of
epiploicae.
appendices
The large intestine has fatty tags, called the
The small intestine has no fatty tags attached to its wall.
(Fig. 5.50).
muscle is collected into three bands, the teniae coli
(with the exception of the appendix), the longitudinal
continuous layer around the gut. In the large intestine
The longitudinal muscle of the small intestine forms a
midline into the right iliac fossa.
num) has a mesentery that passes downward across the
The small intestine (with the exception of the duode
of the filled large intestine.
The caliber of the full small intestine is smaller than that
parts of the colon are fixed.
num) is mobile, whereas the ascending and descending
The small intestine (with the exception of the duode
External Differences
The Abdomen: Part II—The Abdominal Cavity
Differences Between the Small and
Large Intestine
■
■
-
■
■
■
■
-
■
■
■
■
■
■
■
■
-
■
■
■
■
-
Accessory Organs of the
Liver
-
-
-
-
inferior vena cava
phrenic veins
tributaries of azygos veins
esophageal tributaries of left gastric vein
veins on posterior
abdominal wall
colic veins
superficial veins of anterior abdominal wall
superior rectal vein
middle and inferior rectal veins
umbilicus
paraumbilical veins
liver
1
2
3
4
5
FIGURE 5.49
Important portal–systemic anastomoses.