natomy
asic
B
a
The abdomen is the region of the trunk that lies between
femoral artery.
the superficial external pudendal arteries, branches of the
superficial epigastric, the superficial circumflex iliac, and
tion, the skin in the inguinal region is supplied by the
and deep circumflex iliac arteries (see Fig. 4.15). In addi
flanks is supplied by branches of the intercostal, lumbar,
superior and inferior epigastric arteries. The skin of the
The skin near the midline is supplied by branches of the
Arteries
Figure 4.16.
omes and distribution of cutaneous nerves are shown in
inguinal ligament and the symphysis pubis. The dermat
includes the umbilicus and that of L1 lies just above the
over the xiphoid process. The dermatome of T10
The dermatome of T7 is located in the epigastrium
pogastric and the ilioinguinal nerves.
nerves; the 1st lumbar nerve is represented by the iliohy
racic nerves are the lower five intercostal and the subcostal
racic and the 1st lumbar nerves (see Fig. 4.16). The tho
wall is derived from the anterior rami of the lower six tho
The cutaneous nerve supply to the anterior abdominal
Nerve Supply
situated in the linea alba (see below).
site of attachment of the umbilical cord in the fetus; it is
is a scar representing the
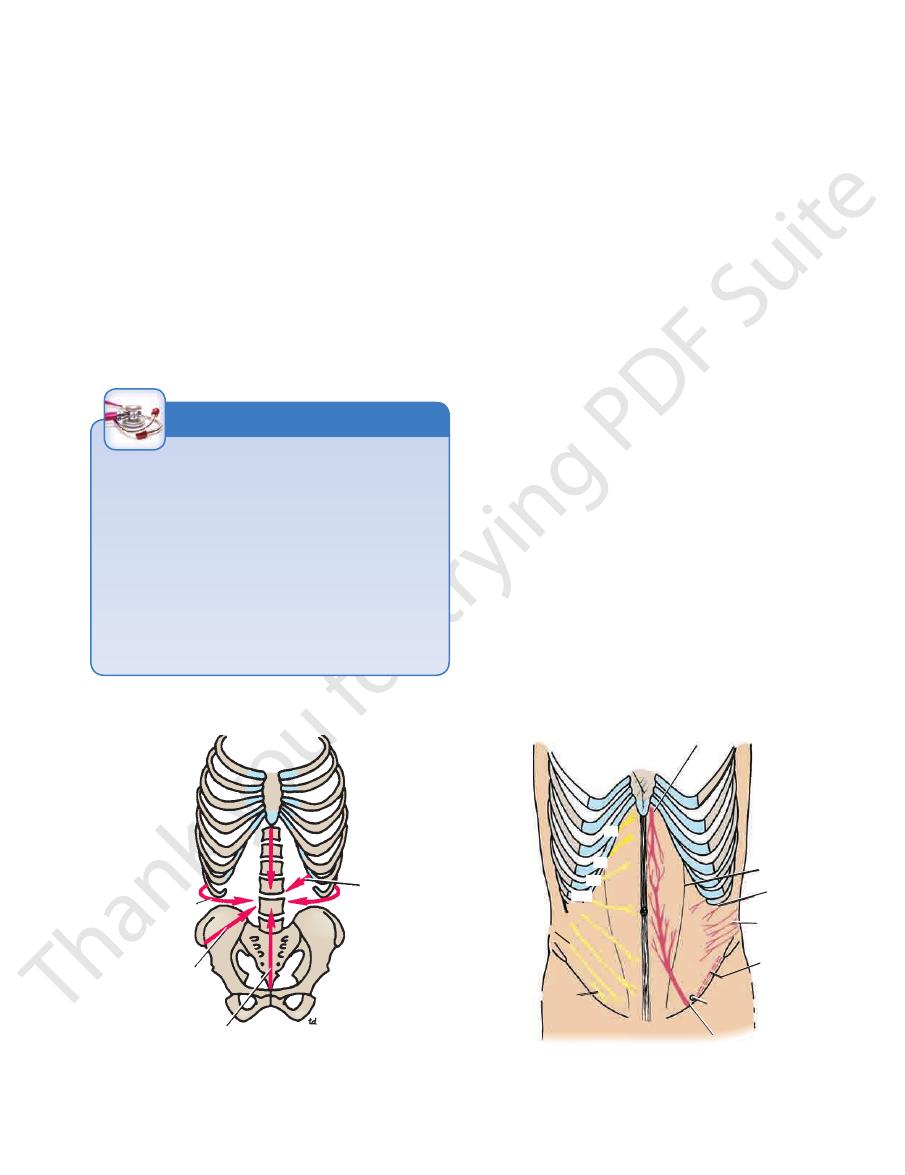
around the trunk. The
stant and run downward and forward almost horizontally
in the skin are con
lines of cleavage
tissue. The natural
except at the umbilicus, where it is tethered to the scar
The skin is loosely attached to the underlying structures
etal peritoneum.
fascia, deep fascia, muscles, extraperitoneal fascia, and pari
The anterior abdominal wall is made up of skin, superficial
Abdominal Wall
the diaphragm above and the inlet of the pelvis below.
Structure of the Anterior
-
Skin
-
umbilicus
-
-
-
-
Blood Supply
-
C H A P T E R O U T L I N E
(continued)
C H A P T E R O B J E C T I V E S
the physician can often feel diseased organs that lie within
The abdominal wall is a flexible structure through which
■
■
Acute abdominal pain, abdominal swellings, and blunt and
penetrating trauma to the abdominal wall are common problems
facing the physician. The problems are complicated by the fact
that the abdomen contains multiple organ systems, and knowing
the spatial relationships of these organs to one another and to
the anterior abdominal wall is essential before an accurate and
complete diagnosis can be made.
■
■
the abdominal cavity. An intact abdominal wall is essential
for the support of the abdominal contents. A defect or
malfunction of the wall can allow the abdominal contents
provides the surgeon with a site for access to deep-lying
to bulge forward and form a hernia. The abdominal wall
diseased structures.
■
■
For the above reasons, the anatomy of the anterior abdominal
wall must be learned in detail. Because of its great clinical
importance, examiners ask many questions in this area.
Spleen 152
Pancreas 153
Kidneys 153
Stomach 154
Duodenum (First Part) 154
Cecum 155
Appendix 155
Ascending Colon 155
Transverse Colon 155
Descending Colon 155
Urinary Bladder and
Pregnant Uterus 155
Aorta 155
External Iliac Artery 155
Surgical Incisions
as a narrow scar, whereas one that crosses the lines will heal
If possible, all surgical incisions should be made in the lines of
cleavage where the bundles of collagen fibers in the dermis
run in parallel rows. An incision along a cleavage line will heal
as wide or heaped-up scars.
C L I N I C A L N O T E S
Infection of the Umbilicus
In the adult, the umbilicus often receives scant attention in the
shower and is consequently a common site of infection.
C L I N I C A L N O T E S
Basic Anatomy
pyramidalis.
the rectus sheath might contain a small muscle called the
abdominis to form the rectus sheath. The lower part of
of the three sheets pass forward, they enclose the rectus
cle, the rectus abdominis (Fig. 4.3). As the aponeuroses
midline anteriorly is, in addition, a wide vertical mus
oblique, and transversus (Fig. 4.2). On either side of the
exterior to interior they are the external oblique, internal
three broad thin sheets that are aponeurotic in front; from
The muscles of the anterior abdominal wall consist of
Muscles of the Anterior Abdominal Wall
ately deep to the membranous layer of superficial fascia.
layer of connective tissue covering the muscles; it lies immedi
The deep fascia in the anterior abdominal wall is merely a thin
Deep Fascia
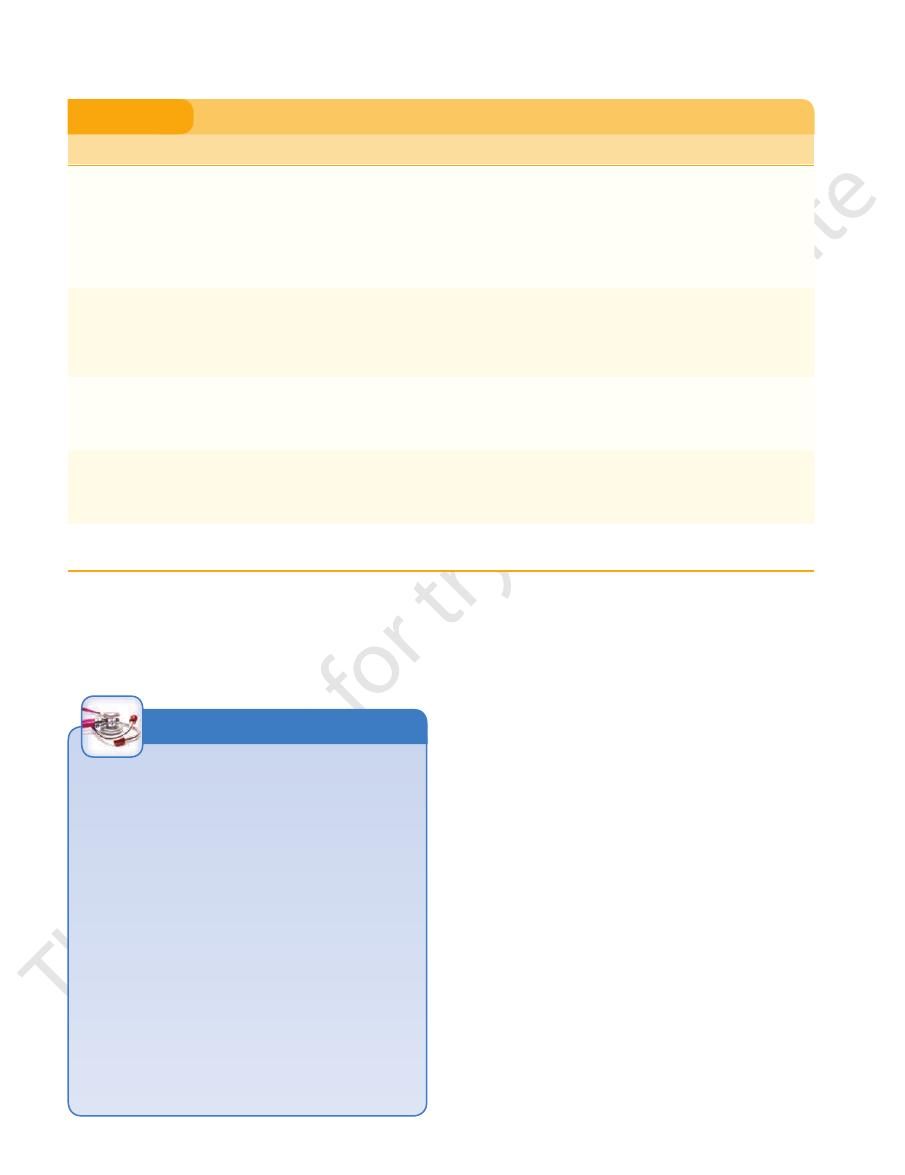
persists as a separate layer.
The membranous layer of the superficial fascia
tos muscle.
is represented as a thin layer of smooth muscle, the
In the scrotum, the fatty layer of the superficial fascia
margin of the perineal membrane (see Fig. 4.1B).
Posteriorly, it fuses with the perineal body and the posterior
Colles’ fascia.
gins of the pubic arch; it is here referred to as
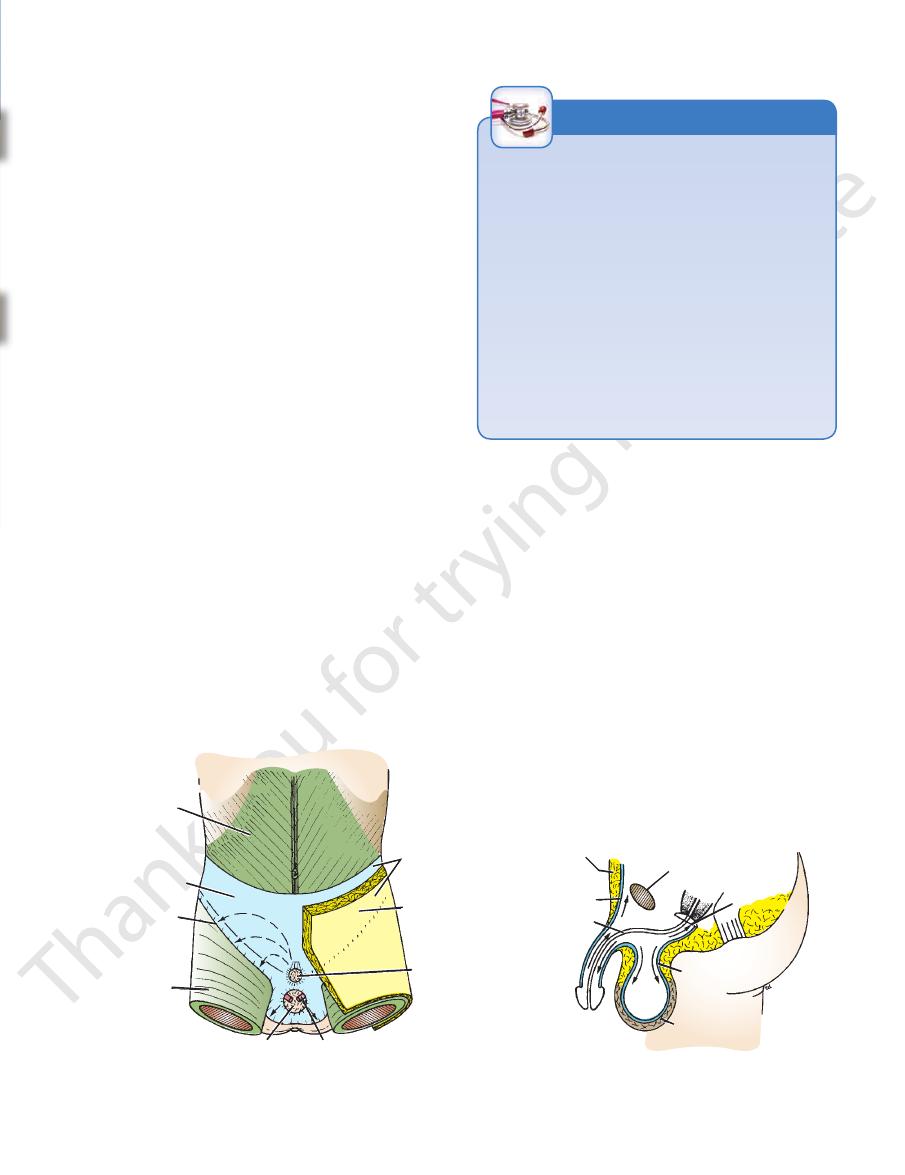
From there, it passes to be attached on each side to the mar
neum, it enters the wall of the scrotum (or labia majora).
tubular sheath for the penis (or clitoris). Below in the peri
nous layer of fascia is not attached to the pubis but forms a
inguinal ligament. In the midline inferiorly, the membra
it fuses with the deep fascia one fingerbreadth below the
membranous layer passes onto the front of the thigh, where
fascia of the back and the thorax, respectively. Inferiorly, the
above, where it becomes continuous with the superficial
The membranous layer is thin and fades out laterally and
be extremely thick (3 in. [8 cm] or more in obese patients).
with the superficial fat over the rest of the body and may
(Fig. 4.1). The fatty layer is continuous
(Scarpa’s fascia)
membranous layer
(fascia of Camper) and a deep
layer
fatty
The superficial fascia is divided into a superficial
Superficial Fascia
veins (see Fig. 4.18).
ral vein via the superficial epigastric and the great saphenous
vein via the lateral thoracic vein and below into the femo
The venous drainage passes above mainly into the axillary
Veins
115
-
-
-
-
dar-
-
-
membranous layer
(Scarpa's fascia)
line of fusion
fascia lata
position of scrotum spermatic cord
position of penis
fatty layer
(Camper's fascia)
superficial fascia
pubis
Colles' fascia
dartos muscle
urethra
membranous layer
(Scarpa's fascia)
fatty layer
(Camper's fascia)
A
B
perineal membrane
aponeurosis
of external
oblique muscle
FIGURE 4.1
taken by urine in cases of ruptured urethra.
Note the attachment of the membranous layer to the posterior margin of the perineal membrane. Arrows indicate paths
anterior abdominal wall. Note the line of fusion between the membranous layer and the deep fascia of the thigh (fascia lata).
Arrangement of the fatty layer and the membranous layer of the superficial fascia in the lower part of the
A.
B.
Membranous Layer of Superficial Fascia
When closing abdominal wounds, it is usual for a surgeon
and the Extravasation of Urine
The membranous layer of the superficial fascia is important
clinically because beneath it is a potential closed space that
does not open into the thigh but is continuous with the super-
ficial perineal pouch via the penis and scrotum. Rupture of the
penile urethra may be followed by extravasation of urine into
the scrotum, perineum, and penis and then up into the lower
part of the anterior abdominal wall deep to the membranous
layer of fascia. The urine is excluded from the thigh because
of the attachment of the fascia to the fascia lata (see Fig. 4.1).
to put in a continuous suture uniting the divided membra-
nous layer of superficial fascia. This strengthens the healing
wound, prevents stretching of the skin scar, and makes for a
more cosmetically acceptable result.
C L I N I C A L N O T E S
116
CHAPTeR 4
(see Fig. 4.1).
thigh, the
of the inguinal ligament is attached the deep fascia of the
versus abdominis muscles. To the inferior rounded border
ament gives origin to part of the internal oblique and trans
The lateral part of the posterior edge of the inguinal lig
(see Fig. 4.6).
pectineal ligament
the periosteum called the
lacunar ligament becomes continuous with a thickening of
(see page 460). On reaching the pectineal line, the
ral ring
femo
free crescentic edge forms the medial margin of the
on the superior ramus of the pubis (see Fig. 4.6). Its sharp,
extends backward and upward to the pectineal line
ment
lacunar liga
4.6). From the medial end of the ligament, the
(Figs. 4.2 and
inguinal ligament
ward on itself, forming the
tubercle, the lower border of the aponeurosis is folded back
Between the anterior superior iliac spine and the pubic
(Figs. 4.4 and 4.5).
round ligament of the uterus) from the margins of the ring
(or the external covering of the
external spermatic fascia
of the uterus) passes through this opening and carries the
Figs. 4.2 and 4.3). The spermatic cord (or round ligament
(see
superficial inguinal ring
tubercle. This is known as the
aponeurosis lies immediately above and medial to the pubic
A triangular-shaped defect in the external oblique
posterior free border.
most posterior fibers passing down to the iliac crest form a
are inserted by means of a broad aponeurosis. Note that the
rior half of the iliac crest (see Fig. 4.2). Most of the fibers
linea alba, the pubic crest, the pubic tubercle, and the ante
ribs and fans out to be inserted into the xiphoid process, the
sheet that arises from the outer surfaces of the lower eight
The external oblique muscle is a broad, thin, muscular
The Abdomen: Part I—The Abdominal Wall
External Oblique
-
-
-
-
-
-
fascia lata
General Appearances of the Abdominal Wall
The normal abdominal wall is soft and pliable and undergoes
inward and outward excursion with respiration. The contour is
subject to considerable variation and depends on the tone of
its muscles and the amount of fat in the subcutaneous tissue.
Well-developed muscles or an abundance of fat can prove to
be a severe obstacle to the palpation of the abdominal viscera.
C L I N I C A L N O T E S
external oblique muscle
internal oblique muscle
iliac crest
inguinal
ligament
lumbar fascia
superficial
inguinal ring
pubic
tubercle
transversus
muscle
lumbar fascia
inguinal ligament
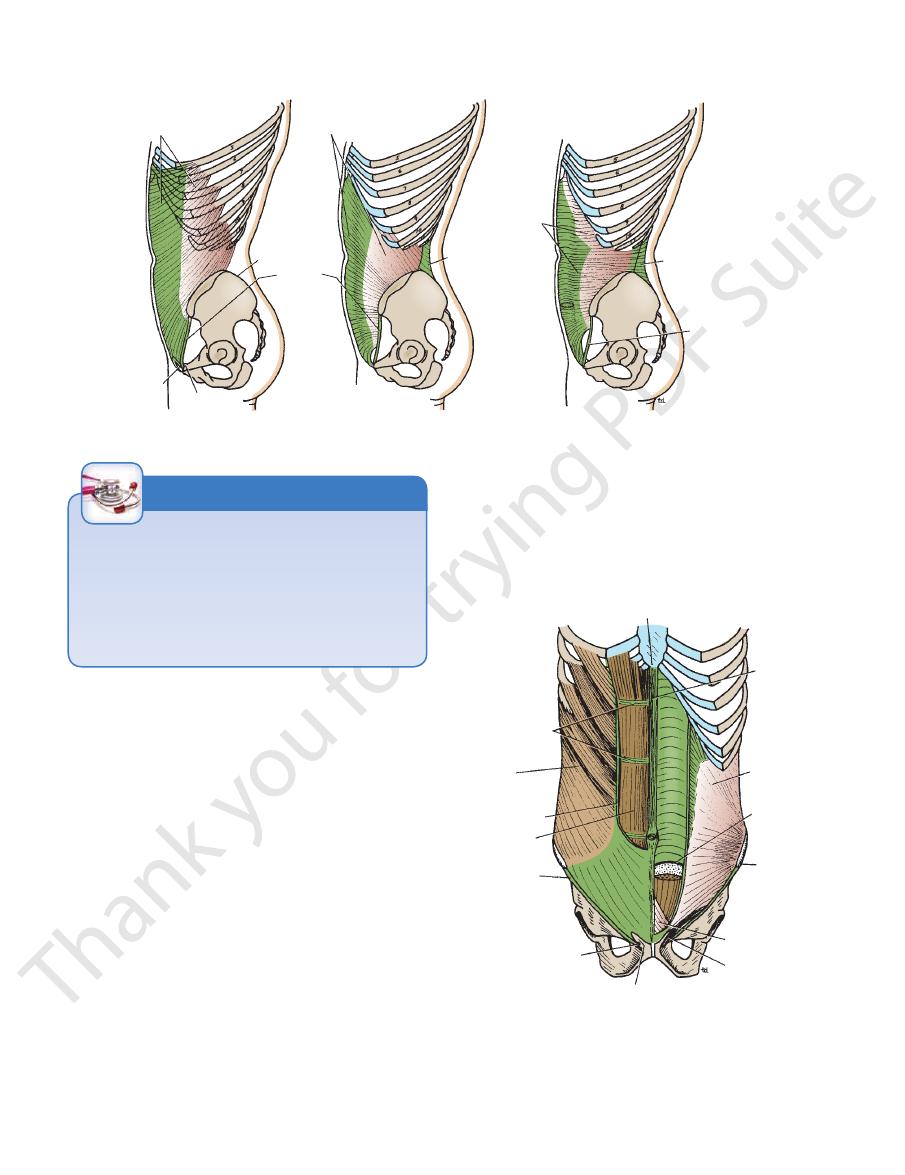
FIGURE 4.2
External oblique, internal oblique, and transversus muscles of the anterior abdominal wall.
xiphoid process
tendinous
intersections
external
oblique
muscle
rectus muscle
inguinal
ligament
pubic tubercle
superficial inguinal ring
spermatic cord
pyramidalis
anterior
superior
iliac spine
arcuate line
internal
oblique
muscle
linea alba
linea semilunaris
FIGURE 4.3
Anterior view of the rectus abdominis muscle
shown at the level of the anterior superior iliac spine.
rectus sheath is shown. The edge of the arcuate line is
The posterior wall of the
has been partly removed, revealing the rectus muscle with
The anterior wall of the sheath
and the rectus sheath. Left.
its tendinous intersections. Right.
Basic Anatomy
upward and forward. The muscle is inserted into the lower
inguinal ligament. The muscle fibers radiate as they pass
two thirds of the iliac crest, and the lateral two thirds of the
(see Fig. 4.2). It arises from the lumbar fascia, the anterior
fibers run at right angles to those of the external oblique
lar sheet that lies deep to the external oblique; most of its
The internal oblique muscle is also a broad, thin, muscu
117
Internal Oblique
-
borders of the lower three ribs and their costal cartilages,
the xiphoid process, the linea alba, and the
sis pubis.
symphy
The internal oblique has a lower free border that arches
over the spermatic cord (or round ligament of the uterus)
crest and the pectineal line. Near their insertion, the low
and then descends behind it to be attached to the pubic
-
est tendinous fibers are joined by similar fibers from the
cremaster
with it some of the muscle fibers that are called the
passes under the lower border of the internal oblique, it carries
As the spermatic cord (or round ligament of the uterus)
the linea alba, but it has a lateral free border.
is attached medially to
conjoint tendon
4.7 and 4.8). The
transversus abdominis to form the conjoint tendon (Figs.
fascia transversalis
transversus
internal oblique
external oblique
remains of
processus vaginalis
vas deferens
external spermatic fascia
cremasteric fascia
internal spermatic fascia
testis
superficial inguinal ring
conjoint tendon
urachus
extraperitoneal fat
peritoneum
obliterated umbilical artery
inferior epigastric vessels
deep inguinal ring
fatty layer of
superficial fascia
(fascia of Camper)
membranous layer of superficial fascia
skin of scrotum
dartos muscle
external spermatic fascia
cremasteric fascia
internal spermatic fascia
tunica vaginalis
conjoint tendon
skin
A
B
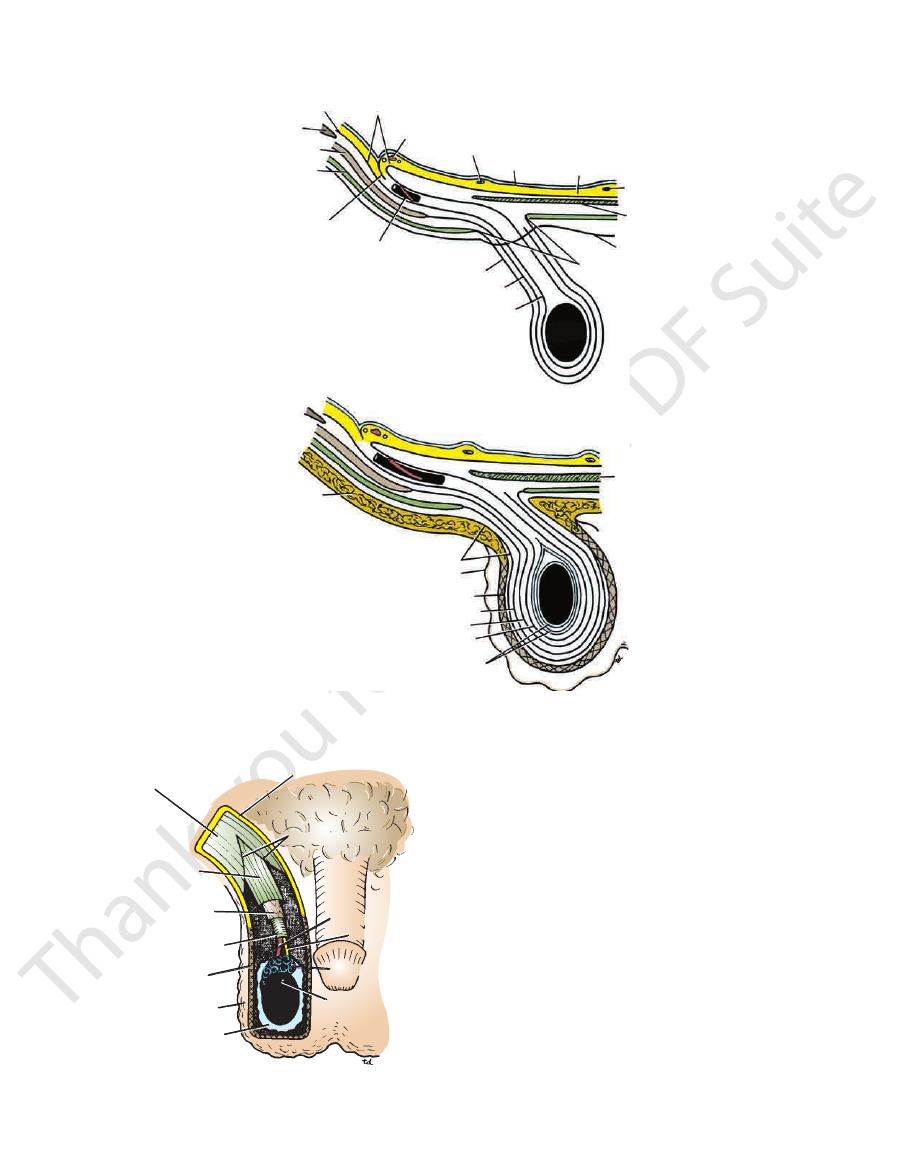
FIGURE 4.4
skin and superficial fascia of the abdominal wall and scrotum have been included, and the tunica vaginalis is shown.
The
Continuity of the different layers of the anterior abdominal wall with coverings of the spermatic cord.
A.
B.
superficial inguinal ring
aponeurosis of
external oblique
external
spermatic fascia
cremasteric fascia
internal
spermatic fascia
dartos muscle
skin of scrotum
tunica vaginalis
superficial fascia
appendix of testis
epididymis
vas deferens
testicular artery
FIGURE 4.5
Scrotum dissected from in front. Note the
spermatic cord and its coverings.
118
CHAPTeR 4
The Abdomen: Part I—The Abdominal Wall
rectus muscle
lacunar ligament
inguinal ligament
pectineal ligament
internal
oblique
muscle
external
oblique
muscle
transversus
muscle
quadratus lumborum
muscle
iliolumbar ligament
posterior superior
iliac spine
crest of ilium
anterior superior
iliac spine
pubic tubercle
symphysis pubis
sacrum
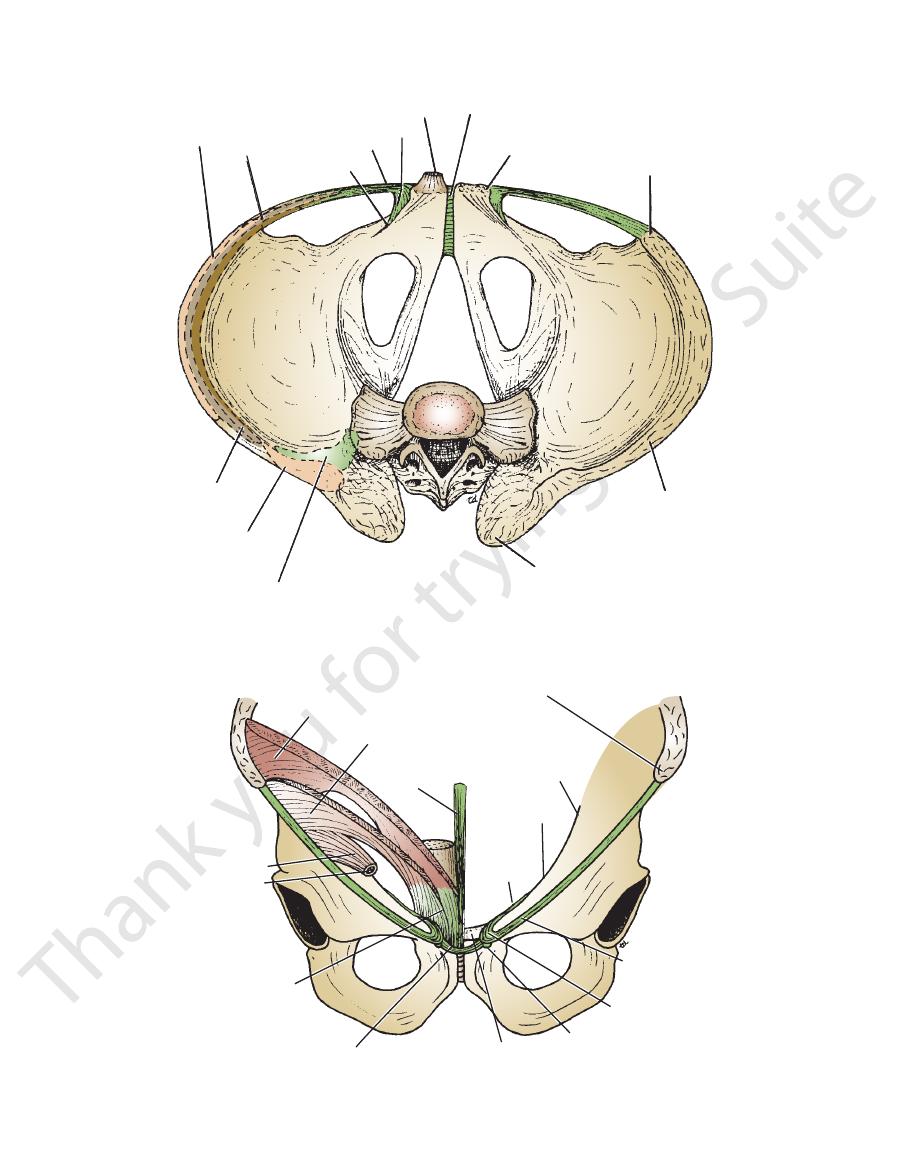
FIGURE 4.6
Bony pelvis viewed from above. Note the attachments of the inguinal, lacunar, and pectineal ligaments.
cremaster muscle
conjoint tendon
aponeurosis of external oblique muscle
pubic crest
pubic tubercle
lacunar ligament
inguinal ligament
anterior superior iliac spine
iliopectineal line
pectineal line
pectineal
ligament
linea alba
internal oblique muscle
transversus muscle
spermatic cord
FIGURE 4.7
achment of the conjoint tendon to the pubic crest and the adjoining
Anterior view of the pelvis showing the att
part of the pectineal line.

Basic Anatomy
119
A
external
oblique
femoral sheath
femoral artery
lymphatic vessels
ilioinguinal nerve
pubic tubercle
spermatic cord
symphysis
pubis
superficial
inguinal
ring
linea alba
iliohypogastric nerve
inferior epigastric
artery
C
deep inguinal
ring
fascia transversalis
conjoint
tendon
B
internal
oblique
ilioinguinal
nerve
cremaster
muscle
femoral vein
pectineal
line
pubic crest
transversus muscle
fascia transversalis
D
inferior
epigastric
artery
pubic tubercle
spermatic cord
FIGURE 4.8
Inguinal canal showing the arrangement of the external oblique muscle
inguinal ring lies lateral to the inferior epigastric artery.
oblique and the internal oblique and the posterior wall is formed by the fascia transversalis and the conjoint tendon. The deep
Note that the anterior wall of the canal is formed by the external
and the fascia transversalis
transversus muscle
(A), the internal oblique muscle (B), the
(C),
(D).
120
CHAPTeR 4
the lumbar fascia, the anterior two thirds of the iliac crest,
six costal cartilages (interdigitating with the diaphragm),
ward (see Fig. 4.2). It arises from the deep surface of the lower
to the internal oblique, and its fibers run horizontally for
The transversus muscle is a thin sheet of muscle that lies deep
Transversus
term used to describe the cremaster muscle and its fascia.
is the
cremasteric fascia
(see Figs. 4.7 and 4.8). The
muscle
The Abdomen: Part I—The Abdominal Wall
-
and the lateral third of the inguinal ligament. It is inserted
the front of the symphysis pubis and from the pubic crest
The rectus abdominis muscle arises by two heads, from
from its fellow by the linea alba.
broader above and lies close to the midline, being separated
along the whole length of the anterior abdominal wall. It is
The rectus abdominis is a long strap muscle that extends
Rectus Abdominis
lumbar vertebrae by the lumbar fascia (Figs. 4.2 and 4.9).
nal oblique and the transversus muscles are attached to the
muscle is free, whereas the posterior borders of the inter
Note that the posterior border of the external oblique
to the pubic crest and the pectineal line (see Figs. 4.7 and 4.8).
internal oblique to form the conjoint tendon, which is fixed
pubis. The lowest tendinous fibers join similar fibers from the
into the xiphoid process, the linea alba, and the symphysis
-
(Figs.
rted into the 5th, 6th, and 7th
4.6 and 4.10). It is inse
the umbilicus, and one halfway between these two (see
one at the level of the xiphoid process, one at the level of
tendinous intersections:
segments by three transverse
The rectus abdominis muscle is divided into distinct
the ninth costal cartilage to the pubic tubercle.
(Figs. 4.3, 4.11, and 4.12). This extends from the tip of
naris
linea semilu
be palpated and often seen and is termed the
it contracts, its lateral margin forms a curved ridge that can
costal cartilages and the xiphoid process (see Fig. 4.3). When
-
Fig. 4.3). These intersections are strongly attached to the
present) and contains the anterior rami of the lower six
the rectus abdominis muscle and pyramidalis muscle (if
The rectus sheath is a long fibrous sheath that encloses
Rectus Sheath
of the rectus abdominis.
the linea alba (see Fig. 4.3). It lies in front of the lower part
from the anterior surface of the pubis and is inserted into
The pyramidalis muscle is often absent. It arises by its base
versus, which form the rectus sheath.
roses of the external oblique, internal oblique, and trans
The rectus abdominis is enclosed between the aponeu
(see below).
rectus sheath
anterior wall of the
-
-
Pyramidalis
posterior cutaneous nerves
sacrospinalis
T7–12
peritoneal
branch
posterior ramus
quadratus lumborum
lateral
cutaneous
nerve
lateral
cutaneous
nerve
anterior cutaneous nerve
L1
external oblique
psoas
internal oblique
transversus
rectus muscles
FIGURE 4.9
ves.
Cross section of the abdomen showing the courses of the lower thoracic and first lumbar ner
Basic Anatomy
121
thoracic nerves and the superior and inferior epigastric ves
rior superior iliac spine, the aponeurosis of the internal
Between the costal margin and the level of the ante
and 7th costal cartilages and the intercostal spaces.
wall is formed by the thoracic wall—that is, the 5th, 6th
the aponeurosis of the external oblique. The posterior
Above the costal margin, the anterior wall is formed by
three levels (Fig. 4.13).
For ease of description, the rectus sheath is considered at
4.3, and 4.10).
roses of the three lateral abdominal muscles (see Figs. 4.2,
sels and lymph vessels. It is formed mainly by the aponeu
-
-
■
■
■
■
-
arcuate line
superficial
linea alba
transversus muscle
inferior
epigastric artery
conjoint tendon
fascia
transversalis
arcuate line
rectus muscle
external oblique
aponeurosis
tendinous
intersections
fascia
skin
xiphoid process
anterior layer of
internal oblique aponeurosis
posterior layer of
spermatic cord
internal oblique aponeurosis
transversus aponeurosis
fascia transversalis
extraperitoneal fat
inferior epigastric artery
peritoneum
pubis
A
B
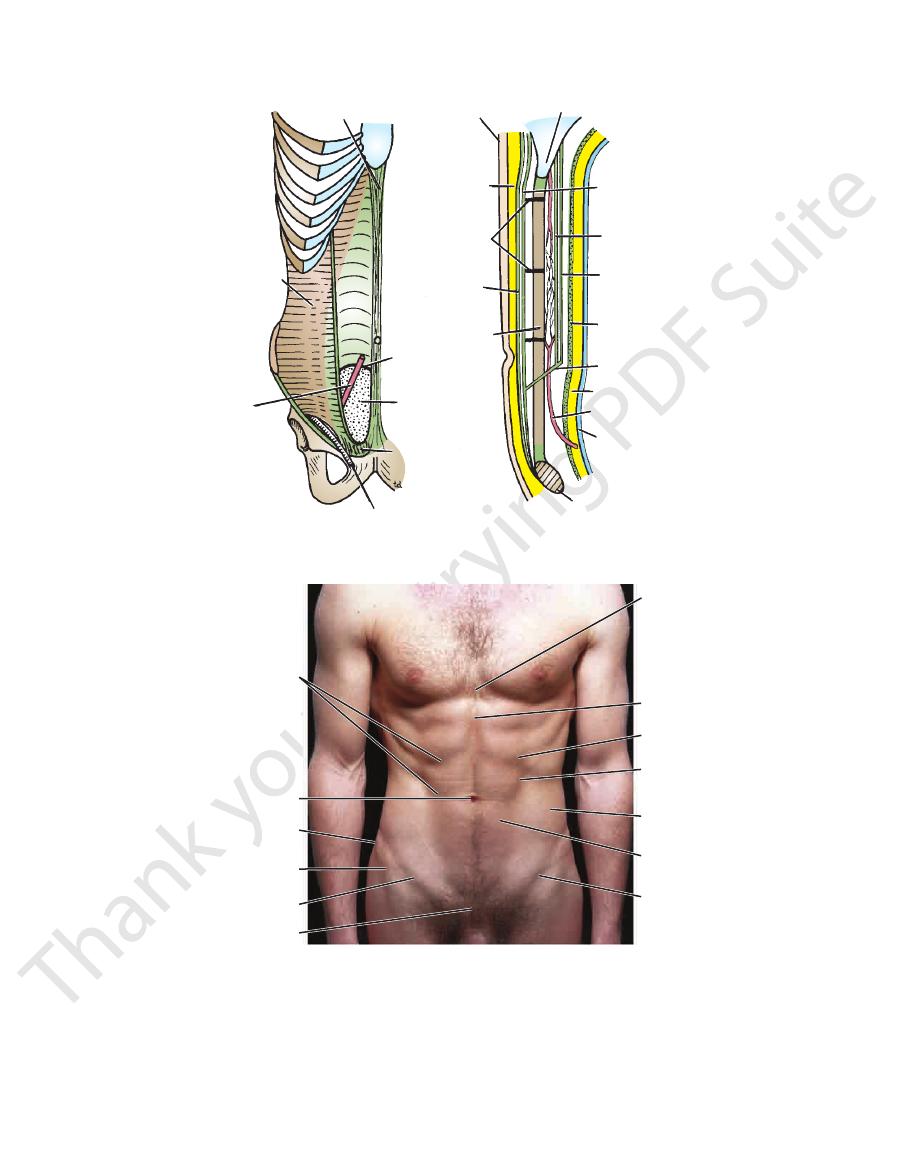
FIGURE 4.10
Rectus sheath in anterior view
the rectus sheath.
Note the arrangement of the aponeuroses forming
and in sagittal section
(A)
(B).
tendinous
intersections
of rectus abdominis
umbilicus
iliac crest
anterior superior
iliac spine
inguinal canal
symphysis pubis
crease overlying
inguinal ligament
rectus abdominis
external oblique
linea semilunaris
costal margin
xiphoid process
xiphisternal joint
FIGURE 4.11
Anterior abdominal wall of a 27-year-old man.
122
CHAPTeR 4
anterior superior iliac spine, the posterior wall has a free,
posterior wall pass in front of the rectus at the level of the
It should be noted that where the aponeuroses forming the
muscle lies in contact with the fascia transversalis.
anterior wall. The posterior wall is absent, and the rectus
the pubis, the aponeuroses of all three muscles form the
Between the level of the anterosuperior iliac spine and
the transversus aponeurosis is directed behind the muscle.
oblique aponeurosis is directed in front of the muscle, and
oblique splits to enclose the rectus muscle; the external
The Abdomen: Part I—The Abdominal Wall
■
■
xiphisternal junction
xiphoid process
infrasternal angle
costal margin
median groove
tubercle of crest
anterior superior
iliac spine
right vertical line
scrotum
pubic
tubercle
superficial inguinal ring
linea
semilunaris
intertubercular
plane
subcostal
plane
transpyloric
plane
tip of ninth
costal cartilage
right
upper
quadrant
right
lower
quadrant
right
iliac
left iliac
left lower
quadrant
umbilical
region
left upper
quadrant
epigastrium
hypogastrium
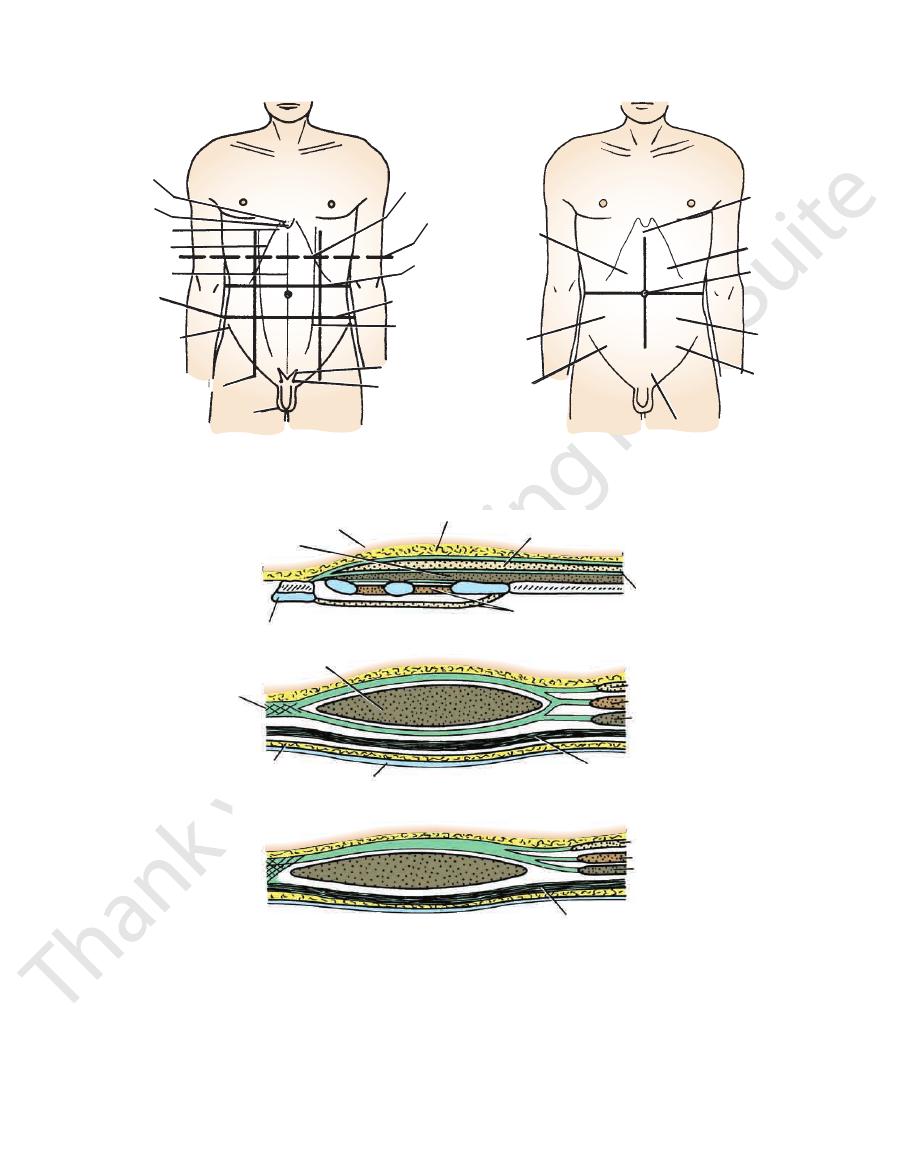
FIGURE 4.12
Surface landmarks and regions of the anterior abdominal wall.
skin
rectus muscle
A
xiphoid process
7
6
5
intercostal muscles
aponeurosis of
external oblique
pectoralis major muscle
superficial fascia
rectus muscle
linea alba
B
extraperitoneal fat
peritoneum
fascia transversalis
transversus
internal oblique
external oblique
C
external oblique
internal oblique
transversus
fascia transversalis
FIGURE 4.13
Transverse sections of the rectus sheath seen at three levels.
Below the level of the anterior superior iliac spine and above the pubis.
margin and the level of the anterior superior iliac spine.
Between the costal
Above the costal margin.
A.
B.
C.
Basic Anatomy
Figs. 4.3 and 4.10).
attached to it by the muscle’s tendinous intersections (see
to the rectus abdominis muscle. The anterior wall is firmly
The posterior wall of the rectus sheath is not attached
pubis.
below the umbilicus to be attached to the symphysis
two sides. Wider above the umbilicus, it narrows down
the fusion of the aponeuroses of the lateral muscles of the
process down to the symphysis pubis and is formed by
Figs. 4.3, 4.7, and 4.13). This extends from the xiphoid
(see
linea alba
opposite side by a fibrous band called the
The rectus sheath is separated from its fellow on the
superior epigastric vessels.
the rectus sheath and pass upward to anastomose with the
and 4.10). At this site, the inferior epigastric vessels enter
(see Figs. 4.3
arcuate line
curved lower border called the
123
The symptoms that follow the trauma include midline abdomi
side below the level of the umbilicus. The source of the bleed
Hematoma of the Rectus Sheath
Hematoma of the rectus sheath is uncommon but important,
since it is often overlooked. It occurs most often on the right
-
ing is the inferior epigastric vein or, more rarely, the inferior
epigastric artery. These vessels may be stretched during a
severe bout of coughing or in the later months of pregnancy,
which may predispose to the condition. The cause is usually
blunt trauma to the abdominal wall, such as a fall or a kick.
-
nal pain. An acutely tender mass confined to one rectus
sheath is diagnostic.
C L I N I C A L N O T E S
transversus muscle
internal oblique
muscle
rectus muscle
external oblique
muscle
FIGURE 4.14
Action of the muscles of the anterior and
lateral abdominal walls. Arrows indicate line of pull of
different muscles.
xiphoid process
iliohypogastric
nerve
ilioinguinal nerve
inferior epigastric artery
position of deep
inguinal ring
deep
circumflex
iliac artery
lumbar
arteries
intercostal
arteries
superior epigastric artery
T9
T10
T11
T12
L1
T8
T7
lateral margin
of rectus
sheath
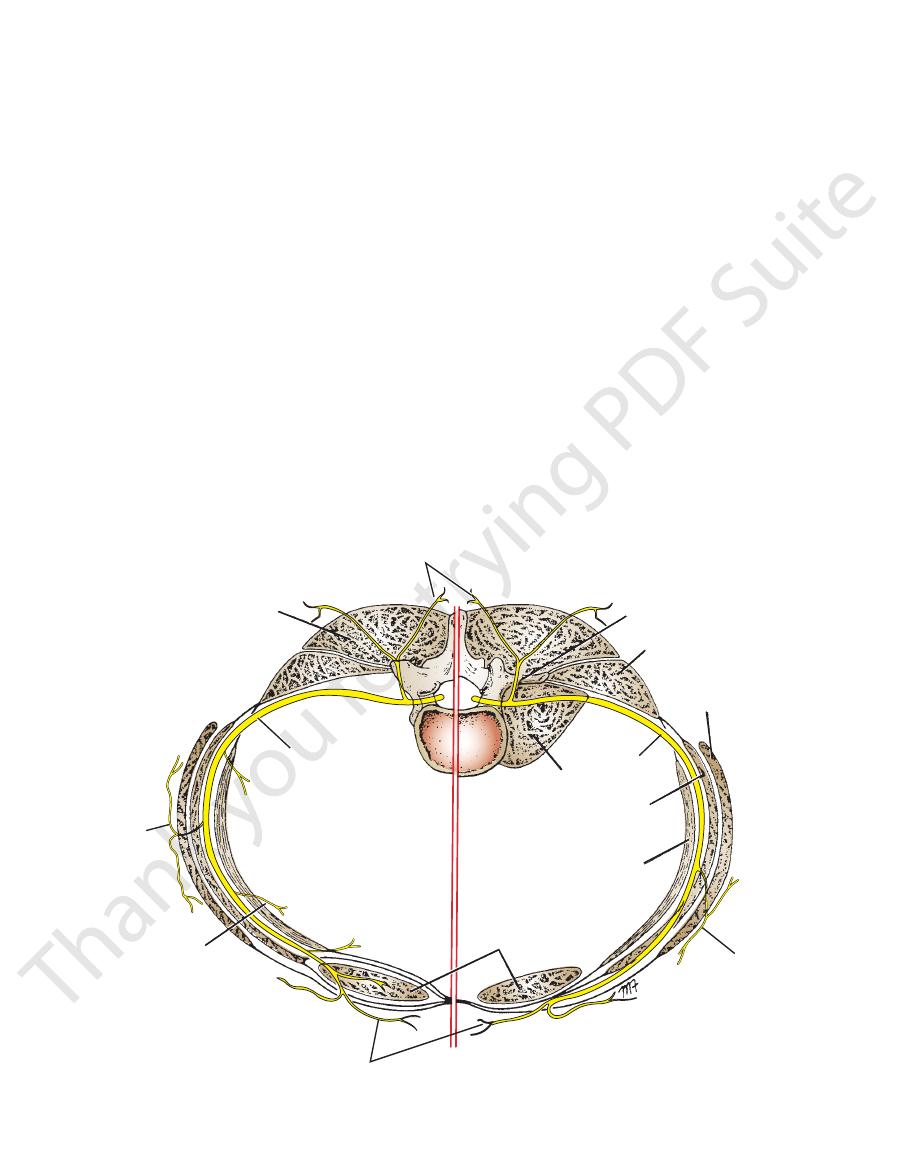
FIGURE 4.15
Segmental innervation of the anterior abdomi
A summary of the muscles of the anterior abdominal
pyramidalis is supplied by the 12th thoracic nerve.
by the lower six thoracic nerves (Figs. 4.9 and 4.15). The
and ilioinguinal nerves (L1). The rectus muscle is supplied
plied by the lower six thoracic nerves and the iliohypogastric
The oblique and transversus abdominis muscles are sup
Nerve Supply of Anterior Abdominal Wall
help in micturition, defecation, vomiting, and parturition.
larynx closed, they increase the intra-abdominal pressure and
simultaneously with the diaphragm, with the glottis of the
porting and protecting the abdominal viscera. By contracting
ribs and sternum. Their tone plays an important part in sup
occurs during coughing and sneezing by pulling down the
The muscles assist in the act of forced expiration that
accommodated.
diaphragm descends so that the abdominal viscera can be
assist the diaphragm during inspiration by relaxing as the
The muscles of the anterior and lateral abdominal walls
during the process.
the pelvis, and the pyramidalis keeps the linea alba taut
4.14). The rectus abdominis flexes the trunk and stabilizes
The oblique muscles laterally flex and rotate the trunk (Fig.
Function of the Anterior Abdominal Wall Muscles
wall
nal wall
-
(left) and arterial supply to the anterior abdominal
(right).
-
Muscles
-
wall, their nerve supply, and their action is given in Table 4.1.
iliaca that covers the iliacus muscle (see page 460).
limbs is formed from the fascia transversalis and the fascia
The femoral sheath for the femoral vessels in the lower
(see Fig. 4.10).
a similar layer lining the diaphragm and the iliacus muscle
the transversus abdominis muscle and is continuous with
The fascia transversalis is a thin layer of fascia that lines
Fascia Transversalis
Table 4.1
124
CHAPTeR 4
transversalis and the parietal peritoneum (see Fig. 4.10).
contains a variable amount of fat and lies between the fascia
The extraperitoneal fat is a thin layer of connective tissue that
Extraperitoneal Fat
The Abdomen: Part I—The Abdominal Wall
sive accumulation of fat in the fatty layer of the superficial
tone of its muscles. A middle-aged woman with poor abdomi
chest expands, the anterior abdominal wall also moves for
Normally,
Abdominal Muscles, Abdominothoracic Rhythm,
and Visceroptosis
The abdominal muscles contract and relax with respiration,
and the abdominal wall conforms to the volume of the abdomi-
nal viscera. There is an abdominothoracic rhythm.
during inspiration, when the sternum moves forward and the
-
ward. If, when the chest expands, the anterior abdominal wall
remains stationary or contracts inward, it is highly probable
that the parietal peritoneum is inflamed and has caused a
reflex contraction of the abdominal muscles.
The shape of the anterior abdominal wall depends on the
-
nal muscles who has had multiple pregnancies is often inca-
pable of supporting her abdominal viscera. The lower part of
the anterior abdominal wall protrudes forward, a condition
known as visceroptosis. This should not be confused with an
abdominal tumor such as an ovarian cyst or with the exces-
fascia.
C L I N I C A L N O T E S
Parietal Peritoneum
the inguinal ligament and symphysis pubis.
through the ring. They end by supplying the skin just above
inguinal ring, and by the ilioinguinal nerve, which emerges
the external oblique aponeurosis above the superficial
is represented by the iliohypogastric nerve, which pierces
not enter the rectus sheath (see Figs. 4.9, 4.15, and 4.16). It
The 1st lumbar nerve has a similar course, but it does
and supplying the skin.
They terminate by piercing the anterior wall of the sheath
supply the rectus muscle and the pyramidalis (T12 only).
nerves pierce the posterior wall of the rectus sheath to
intercostal muscles; see page 41). The lower six thoracic
spaces between the internal intercostal and the innermost
intercostal nerves, which run forward in the intercostal
cles, and the parietal peritoneum. (Compare with the
supply the skin of the anterior abdominal wall, the mus
ilioinguinal nerves, branches of the lumbar plexus. They
lumbar nerve is represented by the iliohypogastric and
intercostal nerves and the subcostal nerves, and the 1st
versus muscles. The thoracic nerves are the lower five
the interval between the internal oblique and the trans
nerves (Figs. 4.9, 4.15, and 4.16). They pass forward in
rior rami of the lower six thoracic and the 1st lumbar
The nerves of the anterior abdominal wall are the ante
Nerves of the Anterior Abdominal Wall
pelvis (see pages 278 and 296).
continuous below with the parietal peritoneum lining the
neum (see Fig. 4.10). This is a thin serous membrane and is
The walls of the abdomen are lined with parietal perito-
-
-
-
Muscles of the Anterior Abdominal Wall
T A B L E 4 . 1
Name of Muscle Origin
Insertion
Nerve Supply
Action
external oblique
Lower eight ribs
Xiphoid process, linea
alba, pubic crest,
pubic tubercle, iliac
crest
Lower six thoracic nerves
and iliohypogastric and
ilioinguinal nerves (L1)
Supports abdominal contents;
compresses abdominal
contents; assists in flex-
ing and rotation of trunk;
assists in forced expiration,
micturition, defecation,
parturition, and vomiting
Internal oblique
Lumbar fascia, iliac crest,
lateral two thirds of
inguinal ligament
Lower three ribs and
costal cartilages,
xiphoid process,
linea alba,
symphysis pubis
Tenses the linea alba
Transversus
Lower six thoracic nerves
and iliohypogastric and
ilioinguinal nerves (L1)
As above
Lower six costal carti-
lages, lumbar fascia,
iliac crest, lateral third
of inguinal ligament
Xiphoid process, linea
alba, symphysis
pubis
Lower six thoracic nerves
and iliohypogastric and
ilioinguinal nerves (L1)
Compresses abdominal
contents
Rectus
abdominis
Symphysis pubis and
pubic crest
5th, 6th and 7th costal
cartilages and
xiphoid process
Lower six thoracic nerves
Compresses abdominal con-
tents and flexes vertebral
column; accessory muscle
of expiration
Pyramidalis
(if present)
Anterior surface of pubis
Linea alba
12th thoracic nerve
Basic Anatomy
125
anterior branch of
seventh thoracic
nerve
lateral branch of
seventh thoracic
nerve
rectus
abdominis
muscle
lateral branch of
10th thoracic nerve
lateral branch
of iliohypogastric
nerve (L1)
superficial
inguinal ring
ilioinguinal
nerve
T8
T10
T12
L1
T7
T9
T11
FIGURE 4.16
Dermatomes and distribution of cutaneous
nerves on the anterior abdominal wall.
Abdominal Pain
pain in the overlying skin that may radiate down into the abdo
A pleurisy involving the lower costal parietal pleura causes
table, to rest the arms by the sides and draw up the knees to
muscles of the anterior abdominal wall of a patient are rigid
See also page 224.
Muscle Rigidity and Referred Pain
Sometimes, it is difficult for a physician to decide whether the
because of underlying inflammation of the parietal peritoneum
or whether the patient is voluntarily contracting the muscles
because he or she resents being examined or because the
physician’s hand is cold. This problem is usually easily solved
by asking the patient, who is lying supine on the examination
flex the hip joints. It is practically impossible for a patient to keep
the abdominal musculature tensed when the thighs are flexed.
Needless to say, the examiner’s hand should be warm.
-
men. Although it is unlikely to cause rigidity of the abdominal
muscles, it may cause confusion in making a diagnosis unless
these anatomic facts are remembered.
It is useful to remember the following:
Dermatomes over:
■
■
The xiphoid process: T7
■
■
The umbilicus: T10
■
■
The pubis: L1
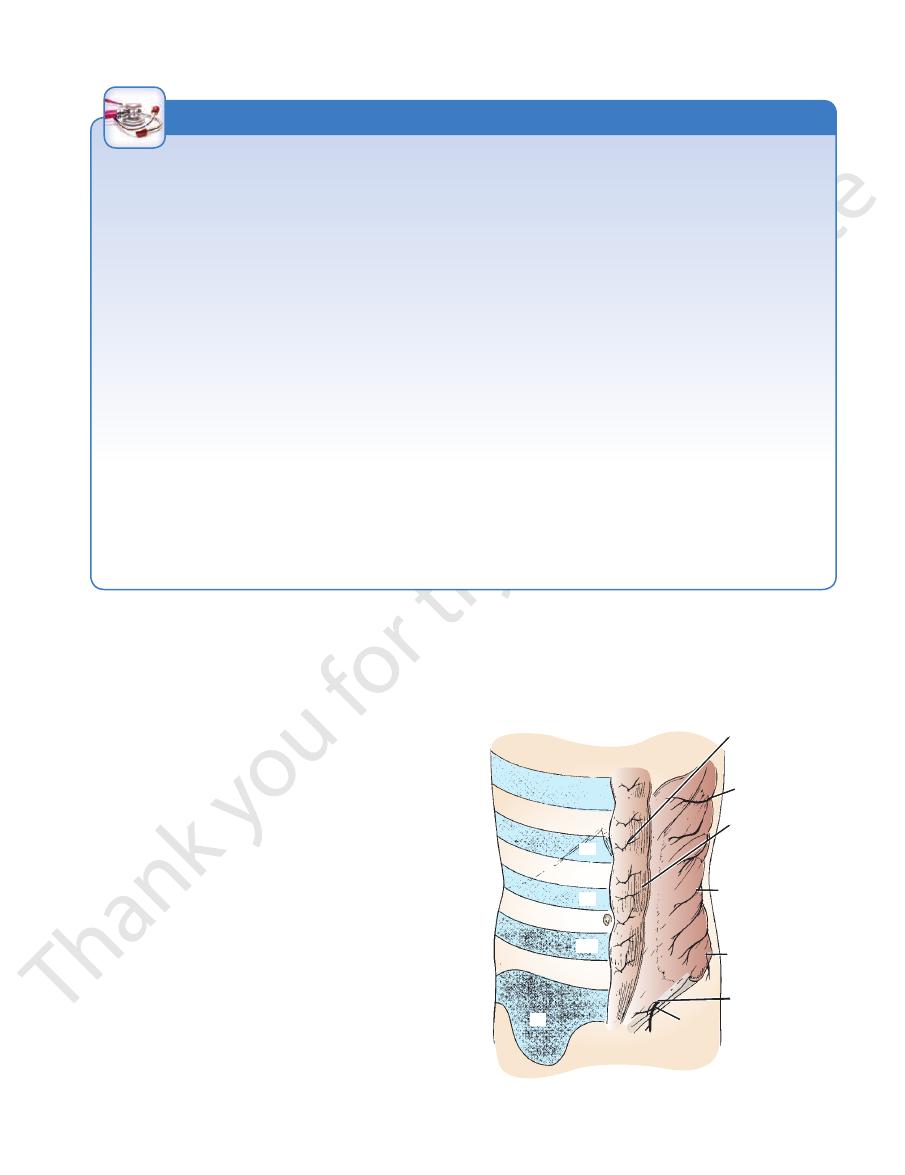
Anterior Abdominal Nerve Block
Area of Anesthesia
The area of anesthesia is the skin of the anterior abdominal wall.
The nerves of the anterior and lateral abdominal walls are the
anterior rami of the 7th through the 12th thoracic nerves and the
1st lumbar nerve (ilioinguinal and iliohypogastric nerves).
Indications
An anterior abdominal nerve block is performed to repair
lacerations of the anterior abdominal wall.
gastric nerve passes forward around the abdominal wall and
and emerges through the superficial inguinal ring. The iliohypo
along the lower border of the costal margin and then infiltrating
(Fig. 4.16). An abdominal field block is most easily carried out
Procedure
The anterior ends of intercostal nerves T7 through T11 enter
the abdominal wall by passing posterior to the costal cartilages
the nerves as they emerge between the xiphoid process and the
10th or 11th rib along the costal margin.
The ilioinguinal nerve passes forward in the inguinal canal
-
pierces the external oblique aponeurosis above the superficial
inguinal ring. The two nerves are easily blocked by inserting the
anesthetic needle 1 in. (2.5 cm) above the anterior superior iliac
spine on the spinoumbilical line (see Fig. 4.17).
C L I N I C A L N O T E S
The dermatome of T7 is located in the epigastrium over
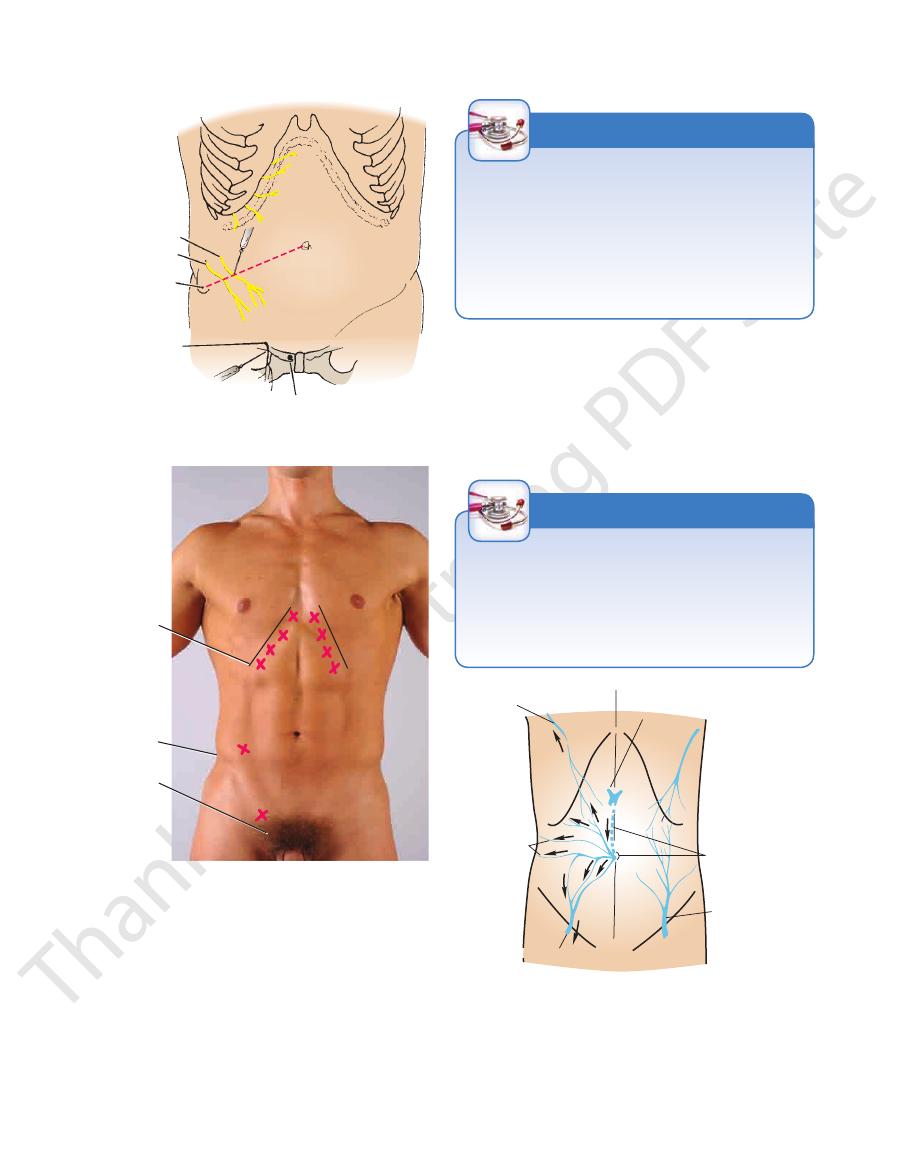
into the axillary vein via the lateral thoracic vein and, below,
the umbilicus (see Fig. 4.18). Above, the network is drained
The superficial veins form a network that radiates out from
Superficial Veins
Veins of the Anterior Abdominal Wall
wall (see Fig. 4.15).
muscle layers and supply the lateral part of the abdominal
branches of the abdominal aorta, pass forward between the
the descending thoracic aorta, and the four lumbar arteries,
The lower two posterior intercostal arteries, branches of
supplies the lower lateral part of the abdominal wall.
rior iliac spine and then continues along the iliac crest. It
4.15). It runs upward and laterally toward the anterosupe
nal iliac artery just above the inguinal ligament (see Fig.
The deep circumflex iliac artery is a branch of the exter
anastomoses with the superior epigastric artery.
the lower central part of the anterior abdominal wall, and
Fig. 4.10). It ascends behind the rectus muscle, supplying
lis to enter the rectus sheath anterior to the arcuate line (see
(see Figs. 4.4, 4.8, and 4.15). It pierces the fascia transversa
and medially along the medial side of the deep inguinal ring
iliac artery just above the inguinal ligament. It runs upward
The inferior epigastric artery is a branch of the external
nal wall, and anastomoses with the inferior epigastric artery.
cle, supplying the upper central part of the anterior abdomi
diaphragm (see Fig. 4.15). It descends behind the rectus mus
rectus sheath between the sternal and costal origins of the
of the internal thoracic artery, enters the upper part of the
one of the terminal branches
superior epigastric artery,
The
Arteries of the Anterior Abdominal Wall
abdominal wall, see Figure 4.16.
the symphysis pubis. For the dermatomes of the anterior
and that of L1 lies just above the inguinal ligament and
the xiphoid process, that of T10 includes the umbilicus,
-
-
-
-
-
126
CHAPTeR 4
into the femoral vein via the superficial epigastric and great
The Abdomen: Part I—The Abdominal Wall
saphenous veins. A few small veins, the
an important portal–systemic venous anastomosis.
along the ligamentum teres to the portal vein. This forms
connect the network through the umbilicus and
veins,
paraumbilical
iliohypogastric nerve
genitofemoral nerve
ilioinguinal nerve
pubic tubercle
costal margin
anterior superior
iliac spine
T7
anterior superior
iliac spine
pubic tubercle
T8
T9
T10
A
B
FIGURE 4.17
ks. T7
Anterior abdominal wall nerve bloc
to the pubic tubercle and infiltrating the subcutaneous tis
blocked by inserting the needle through the skin just lateral
(X). The terminal branches of the genitofemoral nerve are
blocked by inserting the needle about 1 in. (2.5 cm) above
the costal margin. The iliohypogastric ilioinguinal nerves are
though T11 are blocked (X) as they emerge from beneath
the anterior superior iliac spine on the spinoumbilical line
-
sue with anesthetic solution (X).
lateral thoracic vein
portal vein in porta hepatis
lumbar veins
superficial epigastric vein
paraumbilical veins
varicosed vein
FIGURE 4.18
Superficial veins of the anterior abdominal
epigastric vein. This occurs if either the superior or the
between the lateral thoracic vein and the superficial
is obstructed. On the
the direction taken by venous blood when the portal vein
Arrows
and the portal vein via paraumbilical veins.
are anastomoses between systemic veins
left
wall. On the
indicate
right is an enlarged anastomosis
interior vena cava is obstructed.
ses with the superficial epigastric vein, a tributary of the great
If the superior or inferior vena cava is obstructed, the venous
Caval Obstruction
blood causes distention of the veins running from the anterior
chest wall to the thigh. The lateral thoracic vein anastomo-
saphenous vein of the leg. In these circumstances, a tortuous
varicose vein may extend from the axilla to the lower abdomen
(see Fig. 4.18).
C L I N I C A L N O T E S
Deep Veins
bar veins drain into the inferior vena cava.
intercostal veins drain into the azygos veins, and the lum
internal thoracic and external iliac veins. The posterior
follow the arteries of the same name and drain into the
gastric, inferior epigastric, and deep circumflex iliac veins,
The deep veins of the abdominal wall, the superior epi-
-
Portal Vein Obstruction
In cases of portal vein obstruction (see Fig. 4.19), the super-
ficial veins around the umbilicus and the paraumbilical veins
become grossly distended. The distended subcutaneous veins
radiate out from the umbilicus, producing in severe cases the
clinical picture referred to as caput medusae.
C L I N I C A L N O T E S
Basic Anatomy
ward to the superficial inguinal nodes (see Fig. 4.19).
the axilla; below the level of the iliac crests, it drains down
axillary group of nodes, palpated on the posterior wall of
level of the iliac crests is drained upward to the posterior
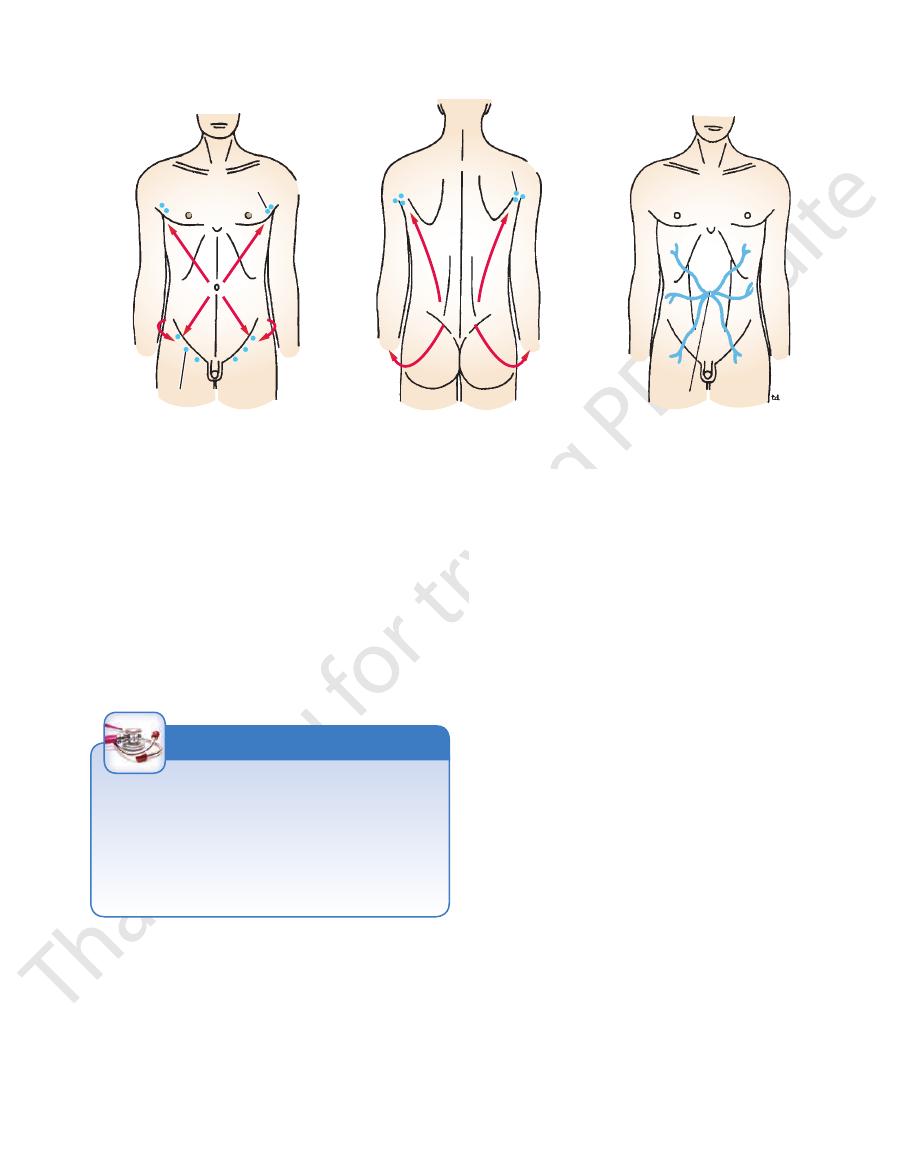
(Fig. 4.19). The lymph of the skin of the back above the
downward and laterally to the superficial inguinal nodes
muscle. Below the level of the umbilicus, the lymph drains
pated just beneath the lower border of the pectoralis major
rior axillary (pectoral) group of nodes, which can be pal
wall above the level of the umbilicus is upward to the ante
The lymph drainage of the skin of the anterior abdominal
Superficial Lymph Vessels
Lymph Drainage of the Anterior Abdominal Wall
127
-
-
-
inguinal node) caused by an infection or malignant tumor of
group of lymph nodes is clinically important. For example, it is
Skin and its Regional Lymph Nodes
Knowledge of the areas of the skin that drain into a particular
possible to find a swelling in the groin (enlarged superficial
the skin of the lower part of the anterior abdominal wall or that
of the buttock.
C L I N I C A L N O T E S
Deep Lymph Vessels
part of the posterior wall, namely, the deep inguinal ring.
therefore strongest where it lies opposite the weakest
inguinal ligament (see Figs. 4.3 and 4.8). This wall is
laterally by the origin of the internal oblique from the
External oblique aponeurosis, reinforced
Anterior wall.
Walls of the Inguinal Canal
external spermatic fascia.
give attachment to the
crura,
4.3, 4.5, and 4.8). The margins of the ring, sometimes called
immediately above and medial to the pubic tubercle (see Figs.
in the aponeurosis of the external oblique muscle and lies
is a triangular-shaped defect
superficial inguinal ring
The
the internal covering of the round ligament of the uterus).
(or
internal spermatic fascia
ring give attachment to the
upward from the external iliac vessels. The margins of the
it medially are the inferior epigastric vessels, which pass
and the symphysis pubis (see Figs. 4.4 and 4.8). Related to
ligament midway between the anterior superior iliac spine
transversalis, lies about 0.5 in. (1.3 cm) above the inguinal
* an oval opening in the fascia
deep inguinal ring,
The
Later, as the result of growth, the deep ring moves laterally.
ficial ring so that the canal is considerably shorter at this age.
child, the deep ring lies almost directly posterior to the super
immediately above the inguinal ligament. In the newborn
oblique muscle (see Figs. 4.3 and 4.8). It lies parallel to and
ficial inguinal ring, a hole in the aponeurosis of the external
versalis (see page 137), downward and medially to the super
extends from the deep inguinal ring, a hole in the fascia trans
The canal is about 1.5 in. (4 cm) long in the adult and
from the uterus to the labium majus.
females, it allows the round ligament of the uterus to pass
structures to pass to and from the testis to the abdomen. In
part of the anterior abdominal wall. In the males, it allows
The inguinal canal is an oblique passage through the lower
and para-aortic (lumbar) nodes.
the internal thoracic, external iliac, posterior mediastinal,
The deep lymph vessels follow the arteries and drain into
Inguinal Canal
-
-
-
*
the
caput medusae
anterior axillary lymph nodes
superficial inguinal nodes
posterior axillary lymph nodes
FIGURE 4.19
Lymph drainage of the skin of the anterior and posterior abdominal walls. Also shown is an example of caput
medusae in a case of portal obstruction caused by cirrhosis of the liver.
openings for the fingers when the glove is viewed from the outside.
with the openings for the fingers seen inside a glove with the absence of
edges of the rings cannot be observed externally. Compare this arrangement
fascia is attached to the margins of the superficial inguinal ring so that the
attached to the margins of the deep inguinal ring and the external spermatic
rings as openings. One must remember that the internal spermatic fascia is
*A common frustration for medical students is the inability to observe these