Lecture 1 - Surgical infection
57
Surgical infection has always been a major complication of
surgery& trauma & has been documented for 4000-5000 year
The Egyptians had some concepts about infection as they were
able to prevent putrefaction, testified by mummification skills.
The Hippocratic teaching described the use of anti-
microbials such as wine and vinegar.
Ignac puerperals sepsis could be reduced from over 10% to
under 2% by the simple act of hand-washing between cases
Koch laid down the first definition of infective disease by
microbes.
Koch postulates proving of an infective organism:
It must be found in considerable numbers is the septic
focus
It should be possible to culture it in a pure form from that
septic focus
It should be able to produce similar lesions when injected
into another host
Advances in the control infection in surgery:
1) Aseptic operating theatre techniques have replaced toxic
antiseptic techniques
2) Antibiotics have reduced postoperative infection rates
after elective and emergency surgery
3) Delayed primary, or secondary, closure remains useful in
contaminated.
Wound infection
Protective factors:
1) Intact epithelial surfaces.
2) Chemical.
3) Humeral.
4) Cellular phagocyte, macrophages, W.B.C.
Factors for increase risk of wound infection:
Malnutrition
Obesity
Weight loss (D.M. ,uremia, jundice)
Immunosuppression cancer, AIDS, steroid
Colonisation & translocation in the gastronintestinal tract
Poor perfusion.
F .b. material.
Poor surgical technique.
Factors that determine whether a wound will
become infected:
1) Host response
2) Virulence and inoculum of infected agent
3) Vascularity and health of tissue being invaded
including local ischaemia as well as systemic shock
4) Presence of dead or foreign tissue
5) Presence of antibiotics during the decisive period.
Classification of sources of infection:
Primary: acquired from a community or endogenous
source (such as that following a perforated peptic ulcer)
Secondary or exogenous (HAI): acquired from the
operating theatre (such as inadequate air filtration) or the
ward (e.g. poor hand –washing compliance) or from
contamination at or after surgery (such as an anastomotic
leak).
Local and systemic manifestation :
Infection is invasion of m.o. through tissues foloowing a
breakdown of local and systemic host defences.
Sepsis: is the systemic manifestation of a documented
infection include:
hyperthermia > 38c
Hypothermia <36c
Tachycardia or tachypnia
Increase WBC >12* 10^9/L
Sever sepsis or sepsis syndrom is sepsis with evidence
of one or more organ failure.
Infection may be 1-Endogenous. 2-Exogenous.
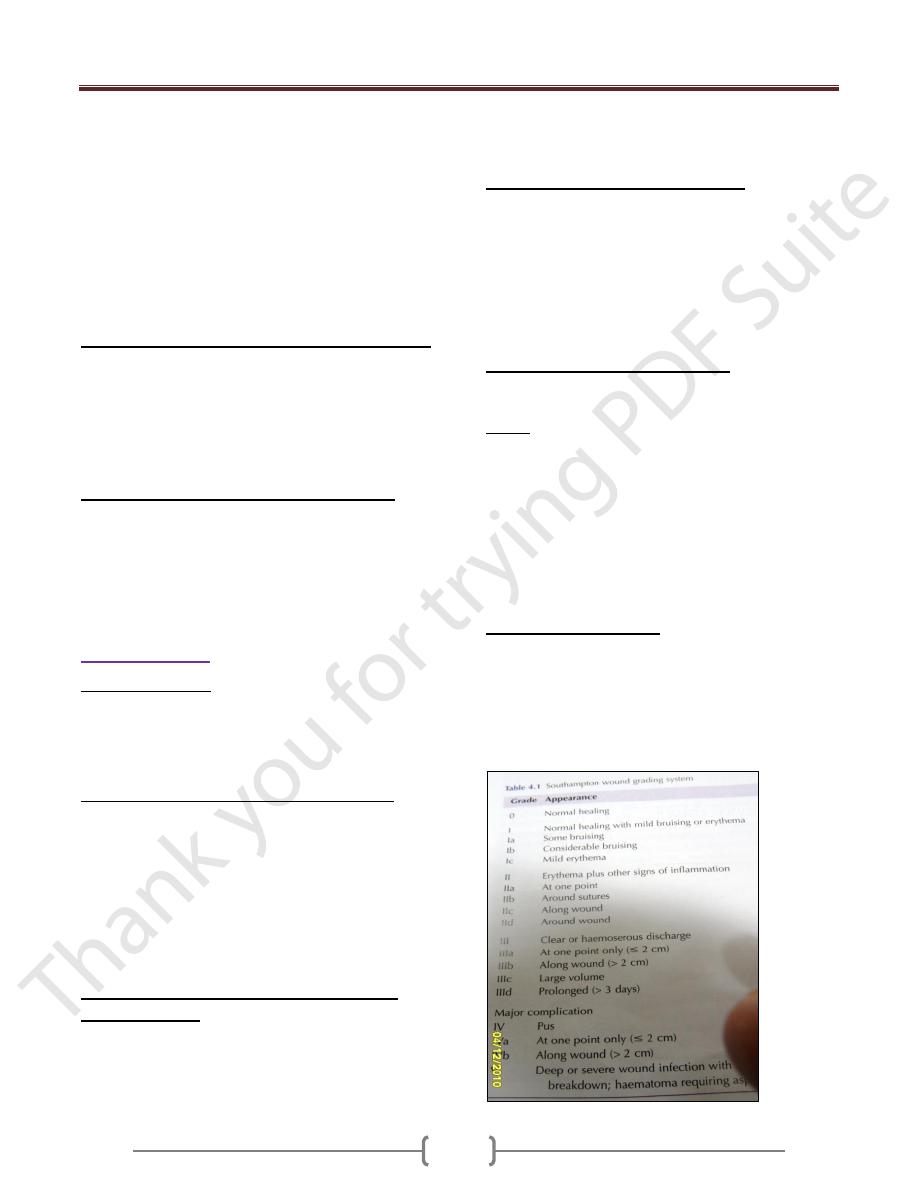
Major Wound Infection:
It discharge pus
Systemic manifestation of tachycardia, pyrexia and
increase WBC.
Minor Wound Infection
May discharge pus but should not be associated with
excessive discomfort,systemic signs or delay in return home.
Lecture 1 - Surgical infection
58
Types of infection
1) wound abscess:
It is characterized by heat, redness, pain, swelling, loss of
function.
M.o. is pyogenic staph. Aureus.
Consequence of abscess;
-May discharge spontaneously
1.May need debridment and curretage
2.Chronic abscess,fistula or sinus
3.Perianastomotic abscess.
4.Deep cavity abscess.
The role of antibiotic is controversial unless there is signs
of spreading infection (cellulitis or lymphangitis).
Surgical curretage and decompression must be adequate.
Delayed primary or secondery suture is safer than
primary.
2) Cellulitis and Lymphangitis:
It is non suppurative invasion infection of tissues.
There is sign of inflammation with poor localisation.
M.o. is B. haemolytic streptococcus , staph. Or
c.perfringene.
There is tissue destruction and ulceration.
Systemic signs of toxaemia are common.
Lymphangitis present as painful red streaks in affected
lymphatic and often accompanied by painful lymph node
in the related drainage area.
3) Gas Gangrene:
It is caused by C.perfringens
Usually found in nature ,soil and faeces
Military, traumatic, and colorectal operation.
Wound infection,sever local wound pain and crepitus with
gas in the tissue
Wound appear as thin brown sweet swelling exudate,
oedema, and spreading gangrene, systemic complication,
circulatory collapse and MSOF.
Prophylaxis is with large doses of I.V. penicillin and
debridement of affected tissue.
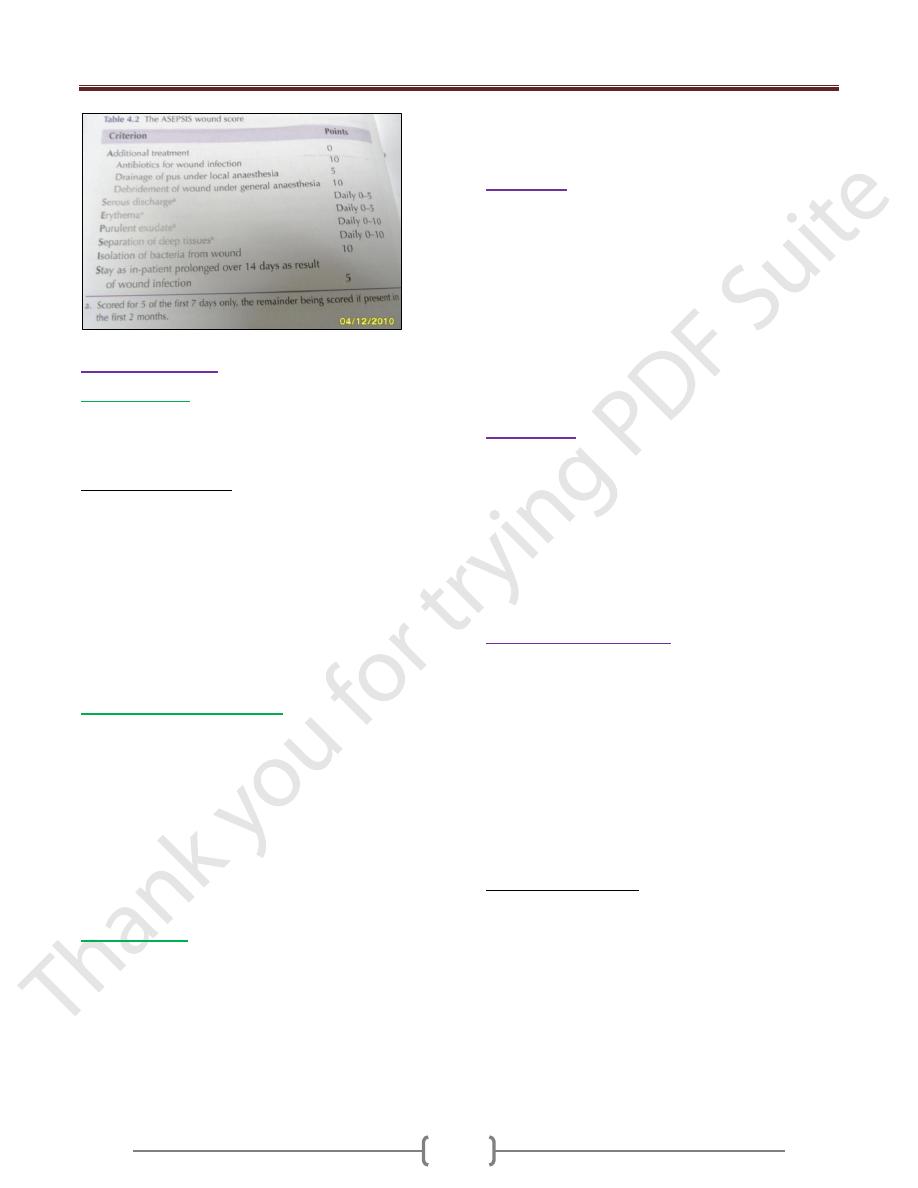
Treatment:
Suppurative wound infection take 7-10 days
Cellulitis appear in 3-4 days
Major wound infection or cellulitis need antibiotic either
impirical or based on culture and sensitivity
Change of antibiotic lead to resistance.
When wound is under tension and there suppuration so
removal of sutures and evacuation of pus.
In severely contaminated wound ,it is logic to leave the
skin layer open & delayed primary or secondary suture
Sample of pus is taken for culture and sensitivity.
Prophylaxis:
By I.V. antibiotic should be given at induction of
anasthesia when local wound defences are at their least
(decisive period) and before contamination occur.
Ex. Lower limb amputation, patient with known valvular
disease of the heart.
Amoxyl for dental surgery
Second generation cephalosporine for urology
In open viscus surgery metronidazol is added.
Preoperative preparation:
Short preoperative hospital stay
The value of personal hygiene
Shaving should be undertaken immediately before surgery
Scrubbing of operating hands
Skin preparation by hibiscrub ,betadine ,savlyon
Theatre technique
Operator skill in gentle manipulation and dissection with
avoidance of dead space and haematoma.
Similar wound surveillance is needed in postoperative
care.
Major wound infection:
significant quantity of pus
delayed return home
patient are systemically ill