1
Lec.5
Pediatrics
6
th
2016/9/3
Session notes
د.ربيع الدبوني
General notes :
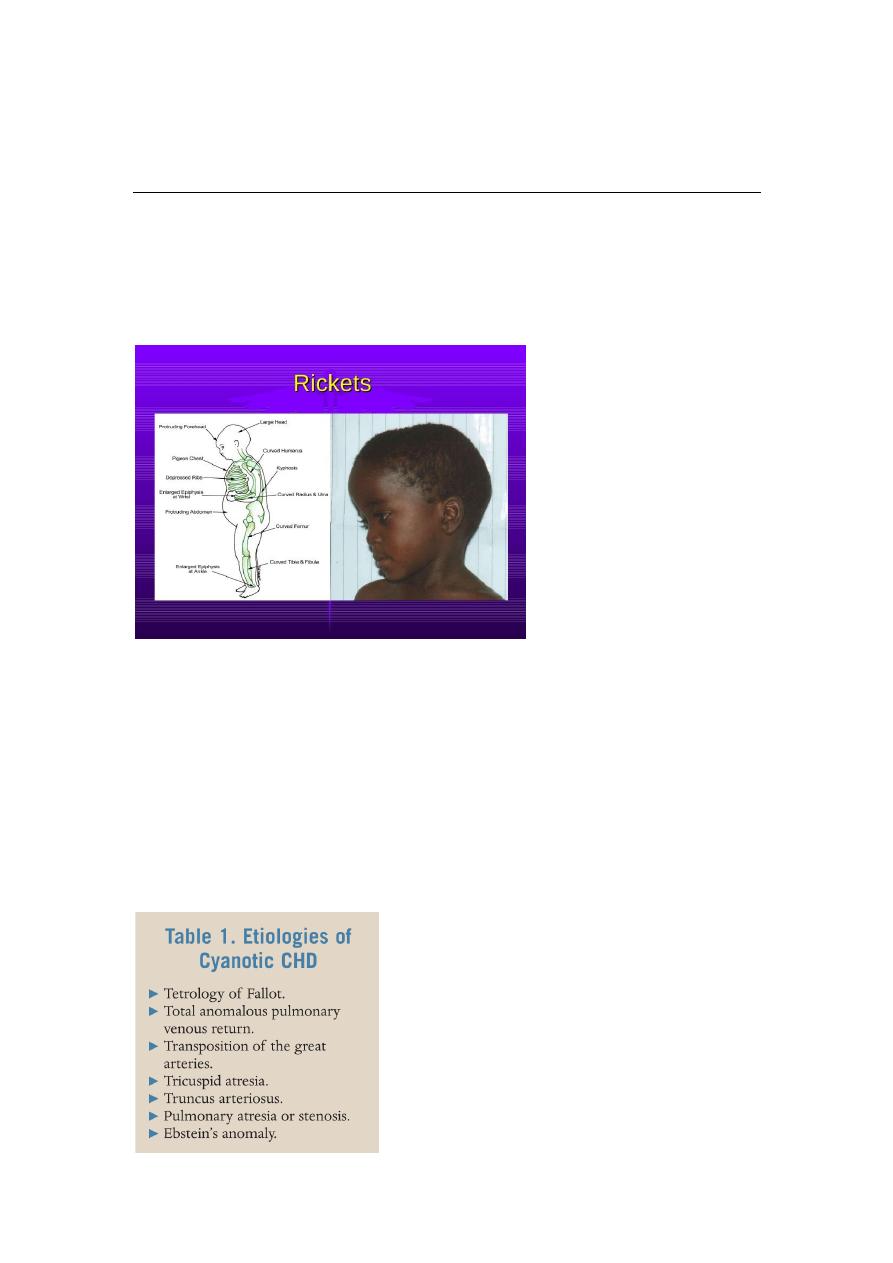
No rickets during marasmus due to calcium and minerals deficiency
-caput quadratum caused by rickets
Clubbing most obvious site big toe
Cyanotic heart disease :
During history presentation try to avoid using definitive diagnose try to
give differential diagnose
DDx of cyanotic heart disease :
2
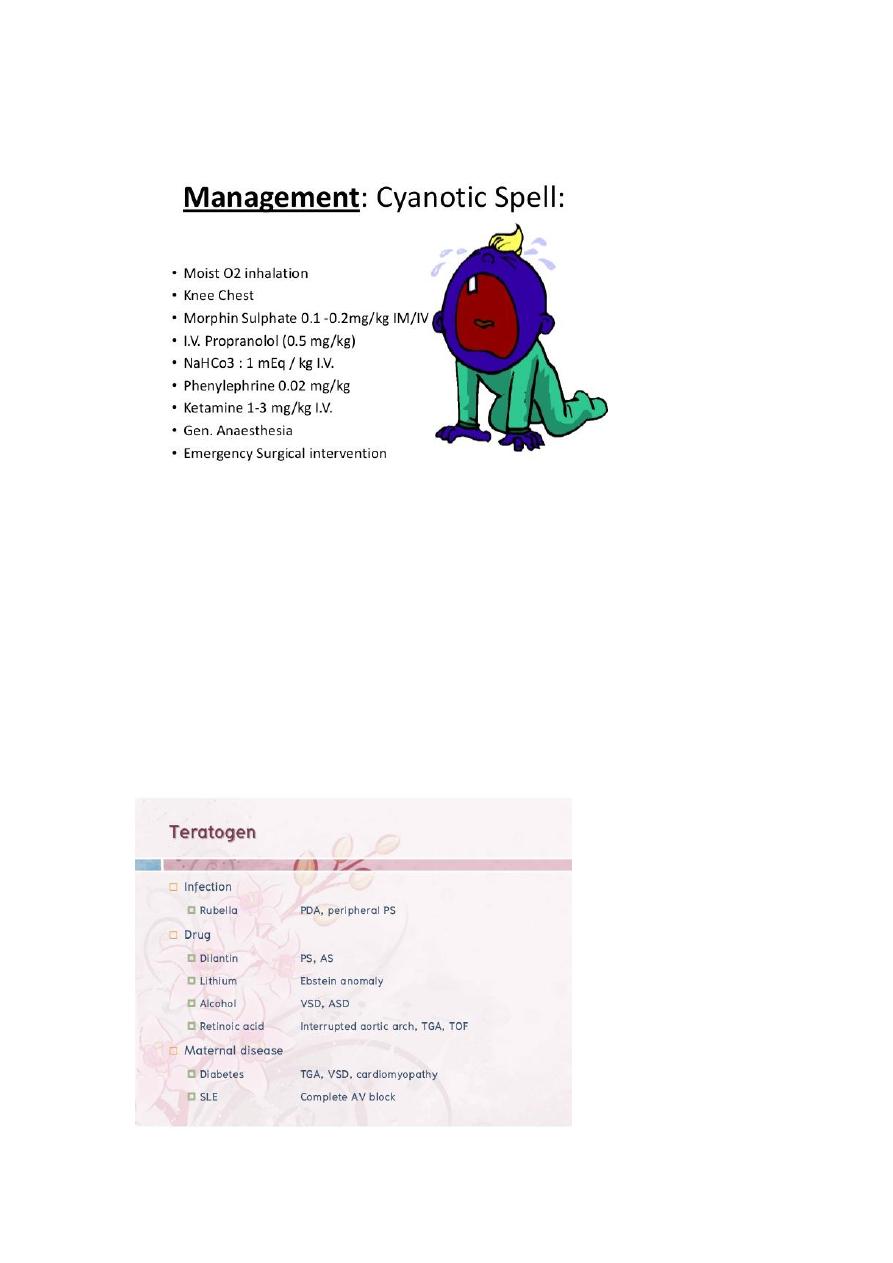
Hypercyanotic spell
Recurrent chest infection occurs in right to left shunt
Infection also reach to brain brain abcess
This infection can be rise from valve affected by infective endocarditis
Drugs cause Congenital heart disease
:
3
Circumsicion can result in bleeding due to secondary polycythemia
Child with snoring adenoid hypertrophy
In a newborn which is centrally cyanosed at birth what is your DDx ?
1-CNS : convlsions , coma , abnormal breathing , acidotic respiration
gasping breathing , pupillary diltation , spastic
2-haematological : rare may be due to methaemglobinemia
3-respiratory
4- cardiac
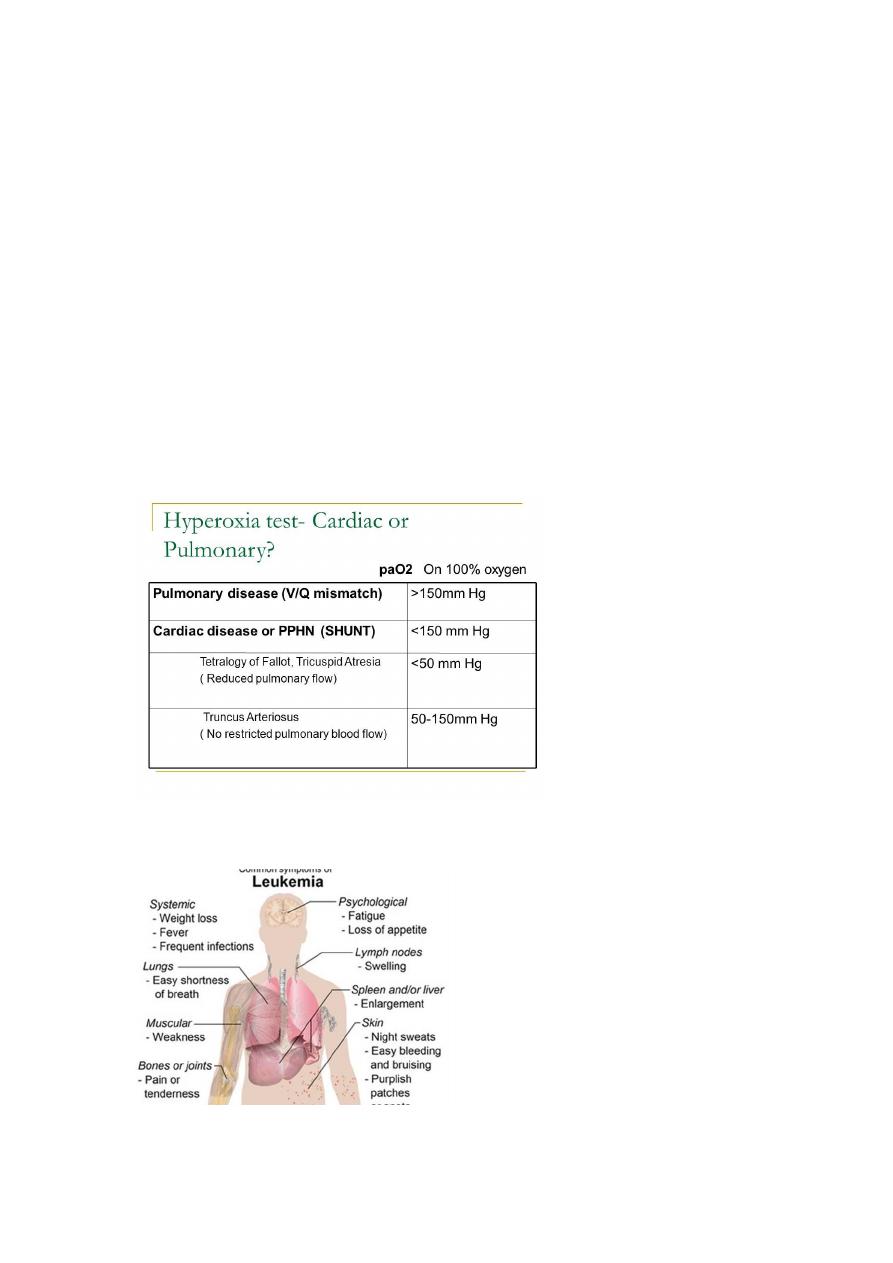
Leukemia presentation :
4
Degenerative brain disease
Cerebral palsy
1-inherited
1-acquired
2-progressive
2-static
3-autosomal recessive eg,
WHD
3-no inheritence
4-associated with PKU ,
glycogenolysis
4-associated with UTI
Bleeding tendency :
Check for
1-frequency
2- local or general
3-any trauma , circumcision
4-history of affected liver or spleen
5-history of bleeding tendency , PUO , haematological dis.
6-family history
7- ask about menorrhagia a,d metorrhagia in female
On Exam :
Look for :
1-anemia
2-purpura , petechia , ecchymosis
3-lymphadenopathy
4-hepatosplenpmegaly
5
5-uremia from acidotic breathing
6-exam the joint mainly in SLE ( bleeding + arthritis )
or recurrent haemarthrosis and leukemia
7-examine the skin , mucous membrane , conjunctiva
Note : if there is any hemorrhagic bullae in the oral cavity or conjunctiva
it is due to thrombocttopenia
Bleeding tendency :
pt
Normal
PTT
NormalVWP OR Klansman dis.
BT
platelets
Prolonged
Reduced (CBC)BM
PT ( protrombin time to measure factors ( 2 , 5 , 7 , 10 ) abbreviated as
(1927)
PTT ( prothromboplasin time ) : to measure any factor except 7
Case : a male baby with GIT bleeding , breast fed baby

6
Invx : PTT increased , PT increase , BT normal , what is the Dx ?
A: Hemorrhagic disease Vitamin K deficency
Invx : PTT , PT , BT
Tx :
According to condition :
Life threatening bleeding blood transfusion , fresh frozen plasma
Mild Vit.K replacement
After 2 hours pt return normal
Case : male newborn his aunt son with bleeding tendency and
heamarthrosis ?
A: Haemophilia
INVX : factor 8 , 9
Tx : factor 8 replacement
Note : all thrombocytopenia associated with mucous membrane
bleeding and GIT bleeding more than deeper tissue bleeding
Haemophilia rarely associated with GIT bleeding
Case :a child with infuenza , recurrent nose bleeding , skin bleeding
After 2 weeks from starting of infection , on exam normal temp. Hb =12
No hepatosplenomegaly no LAP your Dx ?
A: Idiopathic thrombocytopenia ( ITP )
Dx : BM biobsy , increase megakaryocytes
Case : a female child 3 years old with recurrent nose bleeding on exam
well growth no anemia no fever , Hb : 12 , platelets : 12 ,000

7
BT : increase , PTT : increase , her mother with heavy cycle ?
Dx : Von willbrand dis. VWB
Invx : PFT ( platelet function test )
Exam by : Antibiotics ( restocin ) , ADP
Treatment is to give DDAVP ,for mild bleeding, or give plasma-derived
FVIII concentrate ,which cannot produced by recombinant way ,it should
be with FVIII because it hold it in the plasma.. Also same advice to the pt,
not to have intramuscular injection or aspirin or NSAID.
Down's syndrome (trisomy 21)
This is the most common autosomal trisomy and the most common
genetic cause of severe learning difficulties. The incidence in live-born
infants is about 1 in 650. Cytogenetics
The extra chromosome 21 may result from non-disjunction,
translocation or Mosaicism
Non-disjunction (94%) most cases result from an error at meiosis the
pair of chromosome 21s fails to separate, so that one gamete has two
chromosome 21s and one has none fertilisation of the gamete with two
chromosome 21s gives rise to a zygote with trisomy 21 parental
chromosomes do not need to be examined.
Translocation (5%) When the extra chromosome 21 is joined onto
another chromosome (usually chromosome 14, but occasionally
chromosome 15, 22 or 21), this is known as an unbalanced Robertsonian
translocation. An affected child has 46 chromosomes, but three copies
of chromosome 21 material. In this situation, parental chromosomal
analysis is essential since one of the parents carries a balanced
translocation in 25% of cases.
Translocation carriers have 45 chromosomes, one of which consists
the two joined chromosomes the risk of recurrence is 10-15% if the
mother is the translocation carrier and about 2.5% if the father is the
carrier if a parent carries the rare 21:21 translocation, all the offspring
will have Down's syndrome if neither parent carries a translocation (75%
of cases)