Scabies Epidemiology
Epidemiology & Risk Factors:Causative agent:
Human scabies is caused by an infestation of the skin by the human itch mite (Sarcoptes scabiei var. hominis).
The adult female scabies mites burrow into the upper layer of the skin (epidermis) where they live and deposit their eggs.
Transmission
The microscopic scabies mite almost always is passed by direct, prolonged, skin-to-skin contact with a person who already is infested. An infested person can spread scabies even if he or she has no symptoms.
Humans are the source of infestation; animals do not spread human scabies.
Persons At Risk
• Scabies can be passed easily by an infested person to his or her household members and sexual partners.• Scabies in adults frequently is* sexually acquired.
• Scabies is a common condition found worldwide; it affects people of all races and social classes.
• Scabies can spread easily under crowded conditions where close body and skin contact is common.
• Institutions such as nursing homes, extended-care facilities, and prisons are often sites of scabies outbreaks.
• Child care facilities also are a common site of scabies infestations.
Crusted (Norwegian) Scabies
Some immunocompromised, elderly, disabled, or debilitated persons are at risk for a severe form of scabies called crusted, or Norwegian, scabies.
Persons with crusted scabies have thick crusts of skin that contain large numbers of scabies mites and eggs. The mites in crusted scabies are not more virulent than in non-crusted scabies; however, they are much more numerous (up to 2 million per patient).
Because they are infested with such large numbers of mites, persons with crusted scabies are very contagious to other persons. In addition to spreading scabies through brief direct skin-to-skin contact, persons with crusted scabies can transmit scabies indirectly by shedding mites that contaminate items such as their clothing, bedding, and furniture.
Persons with crusted scabies should receive quick and aggressive medical treatment for their infestation to prevent outbreaks of scabies
Causal Agent:
Sarcoptes scabiei var. hominis, the human itch mite.The mites burrow into the upper layer of the skin but never below the stratum corneum. The burrows appear as tiny raised serpentine lines that are grayish or skin-colored and can be a centimeter or more in length.
Other races of scabies mites may cause infestations in other mammals, such as domestic cats, dogs, pigs, and horses. It should be noted that races of mites found on other animals may cause a self-limited infestation in humans with temporary itching due to dermatitis; however they do not multiply on the human host.
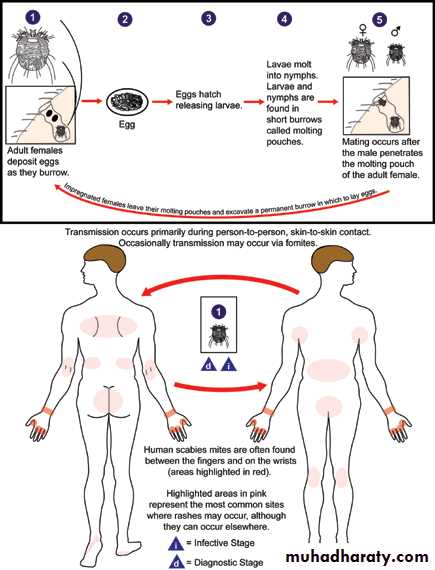
Transmission occurs primarily by the transfer of the impregnated females during person-to-person, skin-to-skin contact. Occasionally transmission may occur via fomites (e.g., bedding or clothing). Human scabies mites often are found between the fingers and on the wrists.
Disease
When a person is infested with scabies mites the first time, symptoms usually do not appear for up to two months (2-6 weeks) after being infested; however, an infested person still can spread scabies during this time even though he/she does not have symptoms.If a person has had scabies before, symptoms appear much sooner (1-4 days) after exposure.
An infested person can transmit scabies, even if they do not have symptoms, until they are successfully treated and the mites and eggs are destroyed.
Common Symptoms
The most common symptoms of scabies, itching and a skin rash, are caused by sensitization (a type of “allergic” reaction) to the proteins and feces of the parasite. Severe itching (pruritus), especially at night, is the earliest and most common symptom of scabies. A pimple-like (papular) itchy (pruritic) “scabies rash” is also common. Itching and rash may affect much of the body or be limited to common sites such as:
Between the fingers
Wrist
Elbow
Armpit
Penis
Nipple
Waist
Buttocks
Shoulder blades
The head, face, neck, palms, and soles often are involved in infants and very young children, but usually not adults and older children.
Tiny burrows sometimes are seen on the skin; these are caused by the female scabies mite tunneling just beneath the surface of the skin. These burrows appear as tiny raised and crooked (serpiginous) grayish-white or skin-colored lines on the skin surface. Because mites are often few in number (only 10-15 mites per person), these burrows may be difficult to find. They are found most often in the webbing between the fingers, in the skin folds on the wrist, elbow, or knee, and on the penis, breast, or shoulder blades.
Possible Complications
The intense itching of scabies leads to scratching that can lead to skin sores. The sores sometimes become infected with bacteria on the skin, such as Staphylococcus aureus or beta-hemolytic streptococci. Sometimes the bacterial skin infection can lead an inflammation of the kidneys called post-streptococcal glomerulonephritis.Diagnosis
Diagnosis of a scabies infestation usually is made based upon the customary appearance and distribution of the rash and the presence of burrows.Whenever possible, the diagnosis of scabies should be confirmed by identifying the mite or mite eggs or fecal matter (scybala). This can be done by carefully removing the mite from the end of its burrow using the tip of a needle or by obtaining a skin scraping to examine under a microscope for mites, eggs, or mite fecal matter (scybala). However, a person can still be infested even if mites, eggs, or fecal matter cannot be found; fewer then 10-15 mites may be present on an infested person who is otherwise healthy.
Treatment:
Suggested General Guidelines
It is important to remember that the first time a person gets scabies they usually have no symptoms during the first 2 to 6 weeks they are infested; however they can still spread scabies during this time.
In addition to the infested person, treatment also is recommended for household members and sexual contacts, particularly those who have had prolonged direct skin-to-skin contact with the infested person..
Both sexual and close personal contacts who have had direct prolonged skin-to-skin contact with an infested person within the preceding month should be examined and treated. All persons should be treated at the same time to prevent reinfestation
Scabicide lotion or cream should be applied to all areas of the body from the neck down to the feet and toes. In addition, when treating infants and young children, scabicide lotion or cream also should be applied to their entire head and neck because scabies can affect their face, scalp, and neck, as well as the rest of their body. The lotion or cream should be applied to a clean body and left on for the recommended time before washing it off. Clean clothing should be worn after treatment.
Bedding, clothing, and towels used by infested persons or their household, sexual, and close contacts (as defined above) anytime during the three days before treatment should be decontaminated by washing in hot water and drying in a hot dryer, by dry-cleaning, or by sealing in a plastic bag for at least 72 hours. Scabies mites generally do not survive more than 2 to 3 days away from human skin.
Because the symptoms of scabies are due to a hypersensitivity reaction (allergy) to mites and their feces (scybala), itching still may continue for several weeks after treatment even if all the mites and eggs are killed. If itching still is present more than 2 to 4 weeks after treatment or if new burrows or pimple-like rash lesions continue to appear, retreatment may be necessary.
Skin sores that become infected should be treated with an appropriate antibiotic prescribed by a doctor.
Use of insecticide sprays and fumigants is not recommended.
Management
Primary management of affected individuals involves application of a topical scabicide such as permethrin 5% (caution in children aged under 6 months), 5% malathion in aqueous base, 10–25% benzyl benzoate emulsion or 5–10% sulphur ointment applied all over the body. In addition, there is increasing interest in the use of oral ivermectin (safety in pregnant women or children under 15 kg body weight has not been established). Best results are obtained by treating the whole household at the same time.Secondary management involves prompt treatment of the complications of scabies, such as impetigo using appropriate antibiotics or antiseptics
Disease burden
Scabies is one of the commonest dermatological conditions, accounting for a substantial proportion of skin disease in developing countries. Globally, it affects more than 130 million people at any time. Rates of scabies occurrence vary in the recent literature from 0.3% to 46%. In the developed world, outbreaks in health institutions and vulnerable communities contribute to significant economic cost in national health services. However, in resource-poor tropical settings, the sheer burden of scabies infestation, as well as their complications, imposes a major cost on health-care systems. In 2010, it was estimated that the direct effects of scabies infestation on the skin alone led to more than 1.5.million YLDS (years lived with disability), and the indirect effects of complications on renal and cardiovascular function are far greater
Distribution
Scabies affects people from every country. However, it is the most vulnerable, young children and the elderly in resource-poor communities who are especially susceptible to scabies as well as to the secondary complications of infestation. The highest rates occur in countries with hot, tropical climates, where infestation is endemic, especially in communities where overcrowding and poverty coexist.Prevention & Control
When a person is infested with scabies mites the first time, symptoms may not appear for up to two months after being infested. However, an infested person can transmit scabies, even if they do not have symptoms. Scabies usually is passed by direct, prolonged skin-to-skin contact with an infested person. However, a person with crusted (Norwegian) scabies can spread the infestation by brief skin-to-skin contact or by exposure to bedding, clothing, or even furniture that he/she has usedScabies is prevented by avoiding direct skin-to-skin contact with an infested person or with items such as clothing or bedding used by an infested person. Scabies treatment usually is recommended for members of the same household, particularly for those who have had prolonged skin-to-skin contact. All household members and other potentially exposed persons should be treated at the same time as the infested person to prevent possible reexposure and reinfestation.
Bedding and clothing worn or used next to the skin anytime during the 3 days before treatment should be machine washed and dried using the hot water and hot dryer cycles or be dry-cleaned. Items that cannot be dry-cleaned or laundered can be disinfested by storing in a closed plastic bag for several days to a week. Scabies mites generally do not survive more than 2 to 3 days away from human skin. Children and adults usually can return to child care, school, or work the day after treatment.
persons with crusted scabies and their close contacts, including household members, should be treated rapidly and aggressively to avoid outbreaks. Institutional outbreaks can be difficult to control and require a rapid, aggressive, and sustained response.
Rooms used by a patient with crusted scabies should be thoroughly cleaned and vacuumed after use. Environmental disinfestation using pesticide sprays or fogs generally is unnecessary and is discouraged.