PNEUMOTHORAX
Q/Regarding pneumothorax .all true except:1- It mean the accumulation of air into the pleural space
2- Is more common in smokers and exsmokers
3-Tension pneumothorax is potentially acute deterioration in cardiopulmonary status requiring prompt relief of the positive pleural pressure.
4-Findings on physical exam .include Reduced breath sounds and dullness
5- Cautious observation in the asymptomatic patient with <15% pneumothorax can be done.
PNEUMOTHORAX
DEFINITION
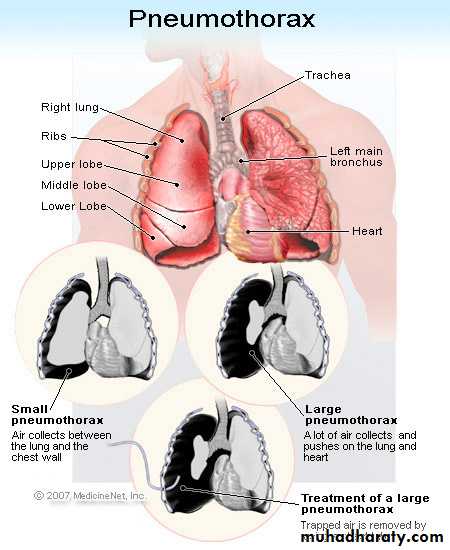
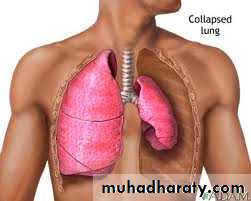
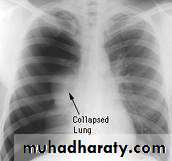
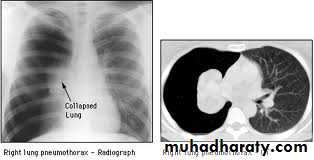
A spontaneous pneumothorax (SP) is defined as the accumulation of air into the pleural space, collapsing the lung. This can be primary SP (i.e., without any obvious underlying lung disease) or secondary SP (i.e., with underlying lung disease).
Which population of patients is most likely to experience a primary spontaneous pneumothorax?
@Primary spontaneous pneumothorax, occurring in patients with no history of pulmonary disease, likely results from spontaneous rupture of a subpleural emphysematous bleb.
It has a peak incidence at 20-30 years of age, is more common in smokers and exsmokers,
has a 4:1 male-to-female ratio, and is seen most often in tall, thin people.
In which patients is a secondary spontaneous pneumothorax most often seen?
Secondary spontaneous pneumothorax, occurring in patients with underlying pulmonary disease, is most often seen with . COPD, is also be associated with pneumonia, bronchogenic carcinoma, mesothelioma, sarcoidosis, tuberculosis, cystic fibrosis, and many other lung diseases.
Pneumothorax may be iatrogenic (after thoracentesis or transbronchial biopsy or secondary to barotrauma) or traumatic. Catamenial pneumothorax is rare and occurs in women at the time of menstruation.
How does pneumothorax present clinically?
Spontaneous pneumothorax usually occurs at rest. Ipsilateral pleuritic chest pain and acute dyspnea are the most common complaints.Findings on physical exam .include:
Sinus tachycardia
Reduced breath sounds
Reduced tactile fremitus
Hyper resonance
Reduced chest wall excursion on the ipsilateral side
What is a tension pneumothorax?
Tension pneumothorax is due to unidirectional flow of air into the pleural space from which it cannot escape. It develops when intrapleural pressure > atmospheric pressure during expiration, causing collapse of the involved lung, shift of the mediastinum, and potentially acute deterioration in cardiopulmonary status requiring prompt relief of the positive pleural pressure.List the physical findings that suggest tension pneumothorax
Signs of a significant pneumothorax (no tactile fremitus, markedly decreased or absent breath sounds, and hyperresonance)
Cardiopulmonary compromise (rapid pulse, hypotension, cyanosis, electromechanical dissociation)
Possibly a shift of the trachea away from the involved side
DIFFERENTIAL DIAGNOSIS of PNEUMOTHORAX:
Pleurisy Pulmonary embolism Myocardial infarction Pericarditis Asthma Pneumonia
Investigation
Includes (pulse oxymetry or ABGs, chest x-ray and, in some (cases, CT scan of the chest
• ABGs may show hypoxemia and hypocapnia
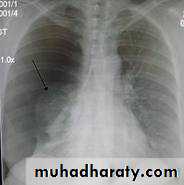
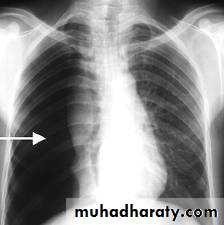
• CXR: Spontaneous pneumothorax is usually confirmed by chest x-ray ..
1. Expiratory films are better at demarcating the pneumothorax pleural line.2. Films should be done with patient standing, not supine.



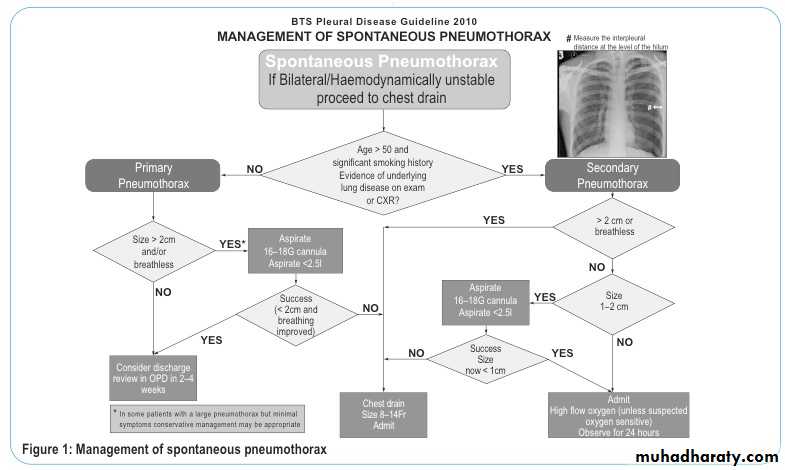


TREATMENT
• Supplemental oxygen: increases the rate of pneumothorax absorption.- Cautious observation in the asymptomatic patient with <15% pneumothorax can be done but requires close daily outpatient monitoring.
- Aspiration using a small IV catheter in the second intercostal space midclavicular line attached to a three-way stopcock and a large syringe.
Repeated films are done immediately after aspiration and again in 24 hours.
#Chest tube insertion has been recommended for patients with primary SP who failed observation and simple aspiration and for all patients with secondary SP. # In tension pneumothorax . the mediastinal contents, including the heart, are shifted to one side. Treatment consists of emergent needle decompression repeated spontaneous pneumothorax should be treated by pleurodesis or surgical intervention (including parietal pleurectomy)
KEY POINTS: TENSION PNEUMOTHORAX
1-Tension pneumothorax is a medical emergency.
2-It should be suspected in any patient with sudden, unexplained deterioration in cardiopulmonary status or a history of pneumothorax.
3-It also should be suspected after a procedure known to cause pneumothorax and in patients receiving mechanical ventilation
4-Tension pneumothorax also may occur during CPR, if it is difficult to ventilate the patient or if electromechanical dissociation is present.
Regarding pneumothorax .all true except:
1- It mean the accumulation of air into the pleural space
2- Is more common in smokers and exsmokers
3-Tensino pneumothorax is potentially acute deterioration in cardiopulmonary status requiring prompt relief of the positive pleural pressure.
4-Findings on physical exam .include Reduced breath sounds and dullness
5- Cautious observation in the asymptomatic patient with <15% pneumothorax can be done
Thank you
Best Regards;
Saif AlDeen Adil Kamil