Dr. Mumtaz Khudhur
Hanna AlnaserAssistant professor
consultant general and laparoscopic surgeon..-Fellow of Arab board of general surgery
Fellow of royal college of physicians and surgeon of glasgowMBchB , C.A.B.S. , FRCS (glasgow)
LIVERSurgical anatomy
It is the largest organ in the body
It wt 1.5 kg
It is divided into two main lobes a large right lobe and a smaller left lobe
Internal anatomy of the liver divided into 8 segment each one is considered as a functional unit each with a branch of hepatic artery portal vein and bile duct and drained by hepatic vein
LIVER FUNCTION
Adequate liver function is essential to survival
No body can live fore more than 48 hrs without liver
Bile formation and excretion at rate of 500-1500ml per day
Bile consist apart from water bile acid cholesterol phospholipid and bilirubin
Bile acid have a dual function 1 transport of cholesterol 2 involved in the digestion of FATS
Bilirubin is formed from haemoglobin degradation inc. level may be associated with inc. haemglobin breakdown , hepatocellular dysfunction,billiry obstruction
Protein metabolism
CHO metabolism and storage
Lipid metabolism
Enzyme production serum transaminases,serum alkaline phosphatase
IMAGING THE LIVER
• Ultra sound bile duct dilatation ,gall stone,liver tumour ,doppler u/s,guiding of biopsy.• Computerized tomography.
• Magnatic resonance imaging
• MRCP produce exellant quality imaging of biliary tract ,it is non invasive
• ERCP required in patient with obstructive pattern of liver function tests .
• PTC
• ANGIOGRAGHY
• NUCLIAR MEDICINE
• SCANNING
• LAPAROSCOPY AND LAPAROSCOPIC U/S.
LIVER TRAUMA
Divided into
Blunt trauma
Penetrating injury by stab and gunshot wound
• Diagnosis
• Clinical picture
• Plain x-ray may show R lower ribs fracture
• u/s of the abdomin
• CT scan of the abdomin and chest
• Liver function test
• Peritoneal lavage and laparoscopy
• Treatment;
• ALWAYS surgical
• Resuscitation,patent airway,replacment of blood loss
• Exploration,stop the bleeding ,stop bile leak,prevent abscess clean from blood and clot deal with any associated injuries
LIVER ABSCESS
• PYOGENIC LIVER ABCESS• ETIOLOGY USUALLY UNEXPLAINED BUT
• Ascending infection-billiary system due to gallstone
• Portal pyaemia (appendicitis,diverticulitis)
• Septicemia especially in DM, elderly.
• Infective hydatid cyst.
• Casative microorganism are E.coli, stept, klebsiella, proteus.
dignosis
• Clinical picture:
• General ill health,increase temperature ,anorexia,malaise, right upper abdominal discomfort.
• Ultrasound or ct scan :(multiloculated cystic mss)
• Aspiration for c &s.
• Increase W.B.C of (PMN type).
• Chest x-ray: (elevated right dome+right basal pneumonia).
• Treatment:
• Antibiotic + U/S guided aspiration.
• Percutaneous drainage with U/S.
• Source of liver abscess.
Amoebic liver abscess
Entamoeba histolytica.Spread by faeco-oral route.
In more than 1/3 of the cases there is amoebic dysentry.
diagnosis:
isolation of the parasite from the liver lesion or the stool.usually from multiple abscesses but single large one(anchovy sauce).
U/S of the abdomen.
Chest x-ray.
Sigmoidoscopy.
Treatment:
Medical treatment for small abscesses by metronidazole 750 mg t.d.s for 5-10 days.
Large abscess needs surgical drainage.
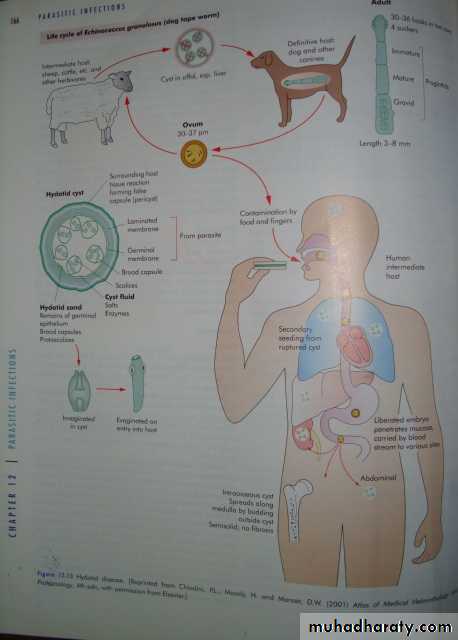
HYDATED LIVER DISEASE
Etiology echinococcus granulosus
Life cycle
Hydatid cyst in tissue of cattle ,sheepmeat eaten by dog ,adult worm in the intestine of dog ,eggs in stool contaminate soil and vegetables ,ingested by human sheep or cattle ,larva hatch in the intestine and inter the portal circulation into the liver.
PATHOLOGY
Right lobe is affected in 80%
• 25%-30% are multiple
CYST is composed of 3 LAYERS
• Aventitia (pseudocyst)
• Laminated membrane (ectocyst)
• Germinal layer(Endocyst)
CLINICAL MANIFESTATION
AsymtomaticAbdominal pain ,tenderness,palpable mass,or hepatomegaly and palpable liver
Jaundice and ascitis
Signs of secondary infection
Anaphylactic reaction
DIAGNOSIS
History and clinical examination
U\S and CT
PlainX-ray
Oesinophilia
Serology in the form of ELISA
complication
• Infection
• Intrabiliary rupture
• Intraperitonial rupture
• Intrathoracic rupture
• Obstructive jaundice
TREATMENT
Small calcified cyst and negative serology need no treatmentUSUALLY treatment is surgical
Contamination is avoided by continuing drug therapy with albindazole and praziquantil
Small localized cyst can be treated by serial u\s for regression in size.
Benign liver tumour
• Haemangioma• Adenoma
• Focal nodular hyperplasia
• Hepatocellar (liver cell carcinoma)
• Bile duct carcinoma( cholangiocarcinoma)
• Hepatoblastoma
Etiology cirrhosis due to chronic liver disease 60%(HBV and HCV)
Clonorchis sineses
Aflatoxin
Clinical Features
Wt. loss and weakness in 80% of cases
Pain in 50% it is dull and persistent ,may be sever and sudden due to secondary rupture or to erosion of blood vessels
Mass may be felt over the liver or hepatomegally
Symptoms of chronic liver disease
Investigation
Liver function test, U\S ,CT and MRI, guided FNA cytology by u\s ,CT,MRI can provide definit diagnosis
Caeliac angiography .
TREATMENT
• The only curative therapy is surgical excision either lopictomy or segmentectomy,however most of the liver tumour are unresectable.• Hepatic artery embolisation.
• Chemotherapy and radiotherapy.
• Liver transplantation
Metastatic neoplasm
It is the most common malignant tumours of the liverPrimary to 2ndary as 1 to 20
Liver is the 2nd to lymph node as a site of metastasis
25% -50% of patients die of cancer have been found to have liver metastesis
Usually are multiple
Treatment
Because it is multiple with presence of primary tumour in G.I.T. there is no way for radical surgery,so AIM OF TREATMENT
• Palliative by embolization or ligation of the hepatic artery.
• Chemotherapy
• If 2nd tumour is multiple and affecting one lobe so remove the primary and hepatic lobectomy.