د.توفيق جاسم
المرحلة الرابعة/الجراحة العامةكلية طب الكندي/جامعة بغداد
2014-2015
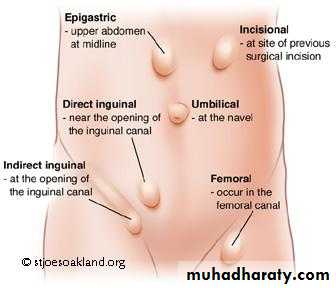
Paraumbilical hernia
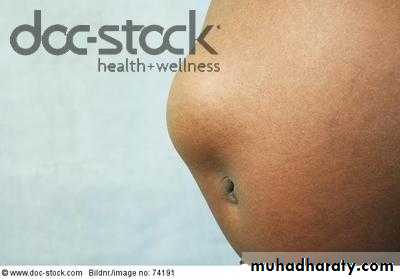
In adults, the hernia does not occur through the umbilical scar. It is a protrusion through the linea alba just above or sometimes just below the umbilicus. It is rounded or oval in shape. It can become very large. The neck is often narrow compared with the size of the sac, which usually consist of greater omentum often with small intestine and, alternatively or in addition, a portion of transverse colon. In long-standing cases, the sac becomes loculated due to adherence of omentum to its fundusClinical features
Women are affected 5 times more frequently than men. The patient is usually overweight and 35-50 years of age. Increasing obesity and repeated pregnancies are important causes. The hernia may become irreducible. Large hernia causes dragging pain by its weight. Gastrointestinal symptoms are common due to traction on the stomach or transverse colon. In long-standing cases, intertrigo of the adjacent skin and trophic ulcer of the fundus



Treatment
Untreated, the hernia increases in size and become irreducible. Eventually, strangulation may occur. Thus, operation is advised in nearly all cses. In obese patient with asymptomatic hernia, operation can be postpond until the patient has lost weightParaumbilical herniorrhaphy; in case of very large hernias(fascial defect>4cm) or for recurrent hernias, the use of prosthetic material(polypropylene mesh) is recommended
Additional lipectomy; in patients with a large pendulous, fat-laden abdominal wall
Strangulation is a frequent complication of a large hernia in adult. Owing to the narrow neck and the fibrous edge of the linea alba, gangrene is liable to occur unless early operation is carried out
Epigastric hernia(fatty hernia of the linea alba)
It occurs through the linea alba(midline) between the xiphoid process and the umbilicus, usually midway between them. Such a hernia commences as a protrusion of extraperitoneal fat through the linea alba. More than one hernia may be presentA swelling the size of pea cosists of extraperitoneal fat only(fatty hernia of the linea alba). If enlage, it drags a pouch of peritoneum and so becomes a true epigastric hernia. The mouth of the sac is rarely large enough to permit a portion of hallow viscus to enter it
It is likely that an epigastric hernia is the direct result of a sudden strain tearing the interlacing fibers of the linea alba. The patients are often manual workers 30-45 years of age
Clinical features
Symptomless;they are usually asymptomatic. a small fatty hernia may only be discovered in the course of routine abdominal palpationPainful; attacks of local pain(varying from mild to sever penetrating epigatric pain), worse on physical exersion, and tenderness to touch and light clothing.it may be accompanied by bloating, nausea and vomiting, often after meals.
Small hernia may be tender.the hernia can be made to bulge by asking the pt to strain.obese pts may need U/S or CT to confirm diagnosis
Referred pain; pain suggestive of a peptic ulcer
Treatment
Surgical repair is essential as there is a high risk that they will incarcerate or strangulate.Vertical or transverse incision. The protruding extraperitoneal fat is cleared by gauze dissection, the small opening in the linea alba is closed with non-absorbable sutures in adults and with absorbable sutures in children. When a hernia sac is present, its opened and any contents reduced, the neck is transfixed and the sac excised, then repairing the linea alba. If the hernia is large(defect greater than 4 cm), the repair should be reinforced by mesh positioned in the retromuscular plane.
Rare hernias in adults
Littre's: hernia sac contains a Meckel's diverticulum. Half are inguinal, 20% femoral, 20% umbilical..Perineal: usually occurs after perineal surgery and presents with asymptomatic swelling.
Traumatic: follows blunt trauma and presents with pain, bruising and bulge.
Interparietal hernia(interstitial hernia);Passes between the layers of the anterior abdominal wall. The sac may be associated with, or communicate with, the sac of comcomitant inguinal or femoral hernia
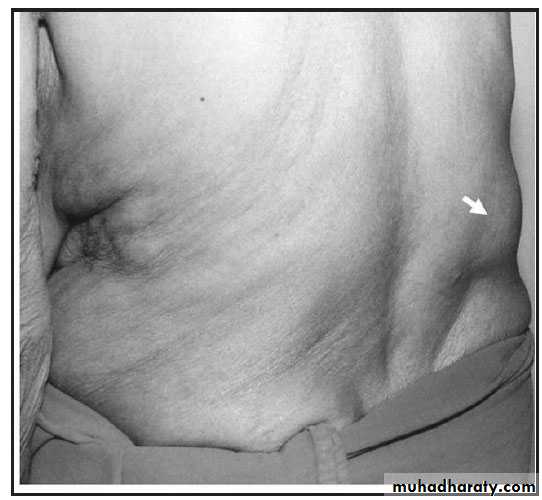
Spigelian. This rare form of abdominal wall hernia occurs at the level of the arcuate line through a defect in the spigelian fascia, which is defined by the lateral edge of the rectus muscle . It is very rare, only 1000 cases reported. The fundus may lie beneath the internal oblique, as it advances, it spreads out like a mushroom between the internal and external and gives rise to more evident sweeling. The patient is often obese, over 50 years with soft, reducible mass lateral to the rectus muscle and below the umbilicus. Diagnosis is confirmed by CT or US scanning. Strangulation may occur
Lumbar(dorsal) hernia
nearly always occurs in the superior and inferior lumbar triangles. Presents with a lump in the side with a heavy, pulling sensation
Most primary lumbar hernia occur through the inferior lumbar triangle of petit bounded below by the crest of the ileum, laterally by the external oblique and medially by the latissimus dorsi. Less commonly, the sac comes through the superior lumbar triangle which is bounded by the twelfth rib above, medially by the sacrospinalis and laterally by the posterior border of the internal oblique. Primary lumbar hernia are very rare(only300 cases reported). More commonly lumbar hernias are secondaey to renal operations
Obturator hernia;Passes through the obturator canal following the path of the obturator nerves and muscle, occurs 6 times more frequently in women than in men, because of a gender-specific larger canal diameter.. Most patients are over 60 years of age. The swelling is usually overlooked because it covered by pectineus, but if the limb is flexed, abducted and rotated outwards, the hernia may be apparent. The leg is usually kept semiflexed and movement increases the pain. On vaginal or rectal examination the hernia sometime can be felt as a tender swelling in the region of the obturator foramen, this hernia presents more commonly as a bowel obstruction than as a protrusion of bowel contents. Treatment is surgical by lower laparotomy
Gluteal and sciatic hernias;A gluteal hernia passes through the greater sciatic foramen. A sciatic hernia passes through the lesses sciatic foramen. The differential diagnosis are;
Lipoma or fibrosarcoma beneath the gluteus maximus
Tuberculous abscess
Gluteal aneurysm
All doubtful swelling in this situation should be explored by operation
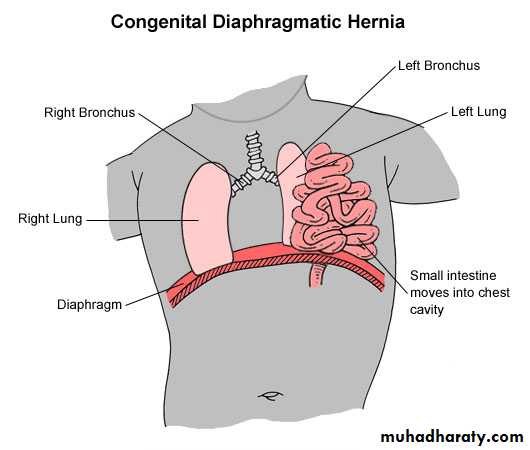
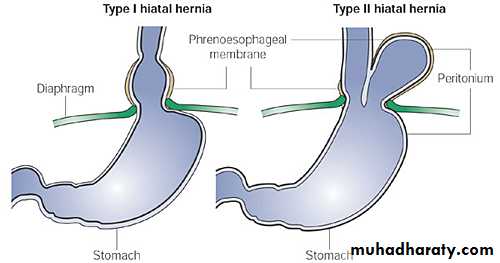
Diaphragmatic hernia;Resuls when part of the stomach or intestine protrudes into the chest cavity through a defect in the diapram
A hiatus hernia is a particular variant of this type in which the normal passageway through which the oesophagus meets the stomach(oesophagal hiatus) serves as a functional defect allowing part of the stomach to herniate into the chest
The hiatus hernia may be either sliding in which the gastro oesophageal junctins itself slids through the defect into the chest, or non-sliding(paraoesophageal), in which case the junction remains fixed while another portion of the stomach moves up through the defect, this type can be dangerous as they may allow the stomach to rotate &obstruct
A congenital diaphragmatic hernia is a distinct problem when the intestinal organs may herniate through several parts of the diaphragm
**
Umbilicus
PreviousNext Section: Etiology
Infection of the umbilical cord
Omphalitis is the medical term for infection of the umbilical cord stump in the neonatal newborn period. . When the stump of the umbilical cord becomes inflamed Usually due to aseptic severance of the cord.
Omphalitis is most commonly caused by bacteria. The most common bacteria are Staphylococcus aureus andless comonly Streptococcus pyogens, Escherichia coli, and Klebsiella pneumoniae.and clostridium tetani The infection is typically caused by a mix of these organisms and is a mixed Gram-positive and Gram-negative infection. Anaerobic bacteria can also be involved.
Like many bacterial infections, omphalitis is more common in those patients who have a weakened or deficient immune system or who are hospitalized and subject to invasive procedures. Therefore, infants who are premature, sick with other infections such as blood infection (sepsis) or pneumonia, or who have immune deficiencies are at greater risk. Infants with normal immune systems are at risk if they have had a prolonged birth, birth complicated by infection of the placenta (HYPERLINK "http://en.wikipedia.org/wiki/Chorioamnionitis" \o "Chorioamnionitis"chorioamnionitis), or have had umbilical catheters.
Clinically, neonates with omphalitis present within the first two weeks of life with signs and symptoms of infection (cellulitis) around the umbilical stump (redness, warmth, swelling, pain), pus from the umbilical stump, fever, tachycardia, low blood pressure , poor feeding, and yellow skin (jaundice). Omphalitis can quickly progress to necrotizing fasciitis and generalized sepsis and presents a potentially life-threatening infection. In fact, even in cases of omphalitis without evidence of more serious infection such as necrotizing fasciitis, mortality is high (in the 10% range).
The infection may spread along the defunct hypogastric arteries or umbilical vein, the following complications may occur;
Abscess of the abdominal wall; this must be opened
Extensive ulceration of the abdominal wall; due to synergistic infection
Septicaemia; from organisms entering the bloodstream via the umbilical vein. Jaundice is often the first sign
Jaundice; appearing 3-6 wks after birth
Portal vein thrombosis; with subsequent portal hypertension
Peritonitis; carries a bad prognosis
Umbilical hernia
Treatment
The chief prophylaxis is strict asepsis during severance of the cord and the use of 0.1% chlorhexidine locally for a few days
Treatment consists of antibiotic therapy aimed at the typical bacterial pathogens in addition to supportive care for any complications which might result from the infection itself such as hypotension or respiratory failure. A typical regimen will include intravenous antibiotics such as from the penicillin-group which is active against Staphylococcus aureus and an aminoglycoside for activity against gram-negative bacteria. For particularly invasive infections, antibiotics to cover anaerobic bacteria may be added (such as metronidazole). Treatment is typically for two weeks Rate this page
Page ratings
Current average ratings.
Umbilical granulomaAn umbilical granuloma is a red, solid, velvety mass on the umbilicus occurring in the first few weeks of life when the baby’s cord dries up and falls off and a stalk of tissue still remains. It looks like a pink to light reddish piece of tissue. The granuloma will not grow normal skin tissue on top of it, and will ooze mucous until it is treated.
Serous or serosanguineous discharge may occur. An umbilical granuloma may be treated with chemical cautery using silver nitrate. Although surgery is rarely needed, a granuloma that persists despite repeated treatment warrants further evaluation to rule out other pathology.. Granuloma is difficult to distinguish from umbilical adenoma(polyps). Usually, an umbilical granuloma can be treated by one application of silver nitrate followed by dry dressings, but an adenoma soon recurs inspite of these measures

Pilonidal sinus
It is a sinus containing a sheath of hairs. It should be excisedUmbilical calculus(umbolith)
Often black and is composed of desquamated epithelium. The treatment is to dilate the orifice and extract the calculus. It may be necessary to excise the umbilicus to prevent recurrenceUmbilical fistula
The umbilicus is a central abdominal scar. A slow leak from any viscus is liable to track to the surface at the umbilicus. Added to this, very occasionally, the vitellointestinal duct or the urachus remains patentThe vitellointestinal duct
If persists, it gives rise to one of the following;
It remains patent. The resulting umbilical fistula discharges mucus and, rarely, faeces. Often, a small portion of the duct near the umbilicus remains unobliterated. This give rise to a sinus that discharges mucus
Both the umbilical and the intestinal ends of the duct close and an intra-abdominal cyst develops
With its lumen obliterated or unobliterated, the duct provides an intraperitoneal band which is a potential danger, for intestinal obstruction is liable to occur when a coil of small intestine passing under or over or becoming twisted around the band
Such a band may contract and pull a meckels diverticulum into a congenital umbilical hernia
A vitellointestinal cord connected to a mickels diverticulum, but not to the umbilicus, becomes adherent to or knotted around, another loop of small intestine and so causes intestinal obstruction
A band extending from umbilicus to the mesentry. The band is probably an obliterated vitelline artery
Treatment; Apatent vitellointestinal duct should be excised together with a mickels diverticulum, preferably when the child is about 6 months old. When it gives rise to intestinal obstruction, dividing the band, excise the band and bury the cut ends
Patent urachus
Urachal remnants: The developing bladder remains connected to the allantois through the urachus. Remnants of this connection may give rise to a patent urachus, urachal sinus, urachal fistula and urachal cyst. Umbilical polyps can also be observed in association with a urachal remnant.Oozing of urine from umbilicus is characteristic of a urachal fistula. Drainage of urine from the umbilicus may suggest bladder outlet obstruction and warrants further investigation. A urachal sinus manifests with drainage that can be clear or purulent. A urachal cyst is usually discovered as a painful mass between the umbilicus and suprapubic area when it becomes infected. Pain and retraction of the umbilicus during urination may suggest a urachal anomaly.
Urachal fistula Seldom presents itself until maturity or old age because the contractions of the bladder commence at the apex and pass towards the base. A patent urachus opens into the apex of the bladder, is closed temporarily during micturition. Thus the fistula remains unobtrusive until a time when the organ is overfull or obstructed
Treatment
Removing the obstruction to the lower urinary tract. If the leak is continues or a cyst develops, umbilectomy and excision of the urachus down to its insertion into the apex of the bladder
Neoplasms of the umbilicus
BenignUmbilical adenoma(raspberry tumour)
Commonly in infants, due to unoblitirated vitellointestinal duct. Mucosa prolapsing through the umbilicus which is moist and tends to bleed
Treatment
If the tumour is pedunculated, a ligature is tied around it. If reappear, umbilectomy is indicated. If patent vitellointestinal duct or band is found with a mickels diverticulum, the diverticulum and the attached cord or duct should be excised
Endometrioma
Occurs in women between 20-45 yrs. The umbilicus becomes painful and bleeds at each menstruation, with a small fleshy tumour at the umbilicus becomes more apparent. Occasionally the condition associated with endometrioma of ovary or uterus. Usually the tumour is solitary, umbilectomy will cure the condition
Malignant
Secondary carcinomaSecondary carcinoma(sister josephs nodule) is always a late manifestation of the disease. The primary is often stomach, colon, or ovary and may be breast