Cardiovascular system
Part 2

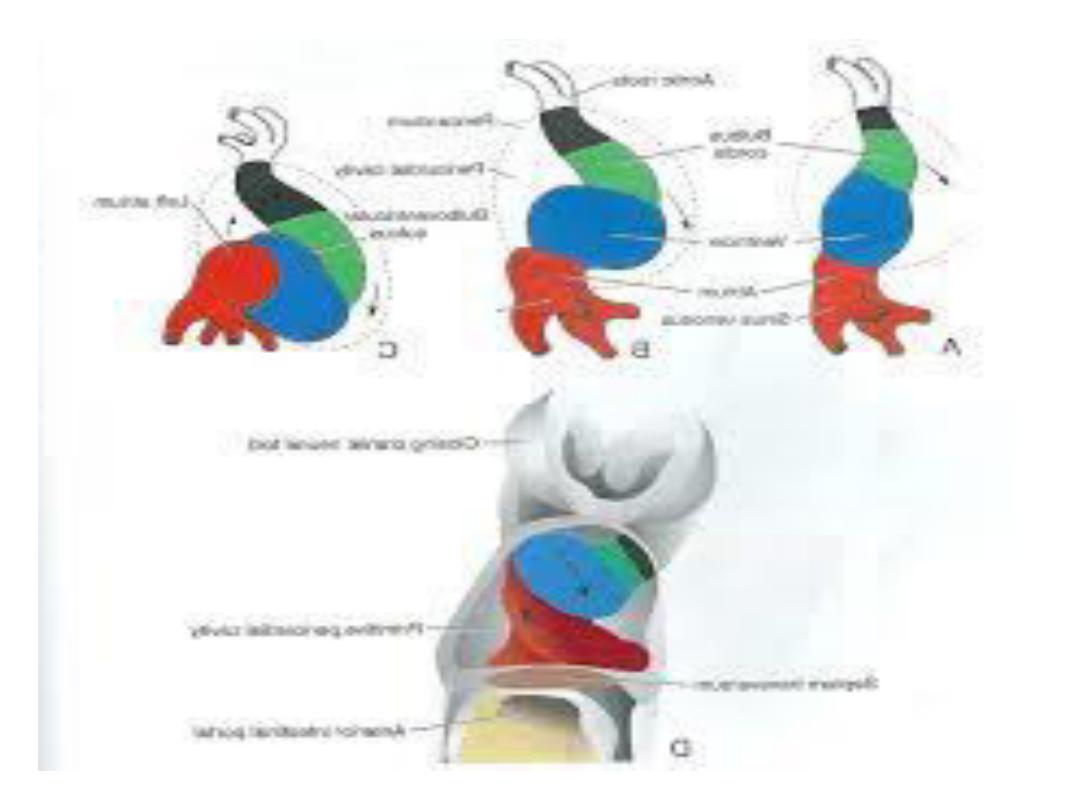
Formation of cardiac loop
• ^ cardiac tube continues to elongate & bend on day 23.
• ^ cephalic portion of ^ tube bends ventrally, caudally, & to ^
Rt; & ^ atrial (caudal) portion shifts dorsocranially & to ^ Lt.
• This bending, which may be due to cell shape changes,
creates ^
cardiac loop.
• It is complete by day 28.
• While ^ cardiac loop is forming, local expansions become
visible throughout ^ length of ^ tube.
• ^
atrial portion,
initially a paired structure outside ^
pericardial cavity,& it is incorporated into ^ pericardial cavity

• ^
atrioventricular junction
remains narrow &
forms ^
atrioventricular canal,
which connects
^ common atrium & ^ early embryonic
ventricle.
• ^
bulbus cordis
is narrow except for its
proximal third.
• This portion will form ^
trabeculated part of ^
Rt. Ventricle.
^ midportion, ^
conus cordis,
will
form ^ outflow tracts of both ventricles.
• ^ distal part of ^ bulbus, ^
truncus arteriosus,
will form ^ roots & proximal portion of aorta &
pulmonary artery.

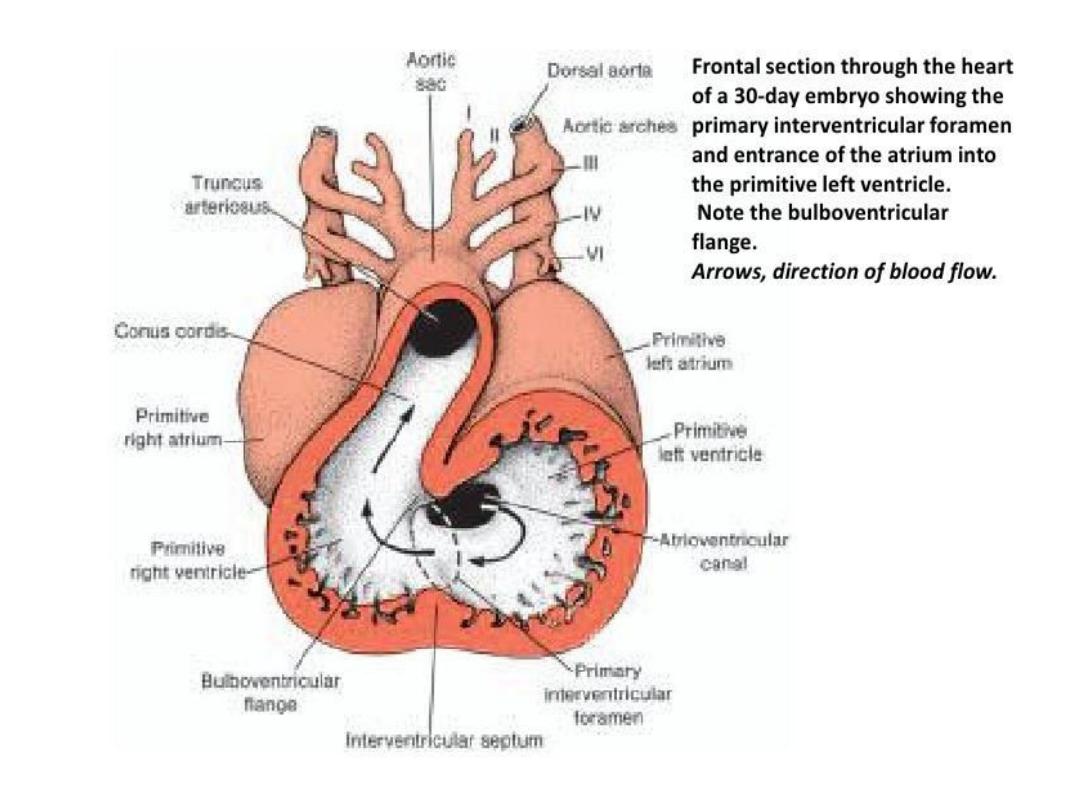
• ^ junction between ^ ventricle& ^ bulbus
cordis, externally indicated by ^
bulboventricular sulcus,
re ai s arrow. it’s
called
^ primary interventricular foramen.
• Thus, ^ cardiac tube is organized by regions
along its craniocaudal axis from ^ conotruncus
to ^ Rt. Ventricle to ^ Lt. ventricle to ^ atrial
region, respectively.
• At ^ end of ^ loop formation, ^ smooth walled
heart tube begins to form primitive trabeculae
in two sharply defined areas just proximal &
distal to ^ primary interventricular foramen.

• ^ primitive ventricle, which is now trabeculated,
is called ^
primitive left ventricle,
&^trabeculated
proximal third of ^ bulbus cordis may be called ^
primitive Rt. Ventricle.
• This change in position is ^ result of formation of
two transverse dilatations of ^ atrium, bulging on
each side of ^ bulbus cordis.
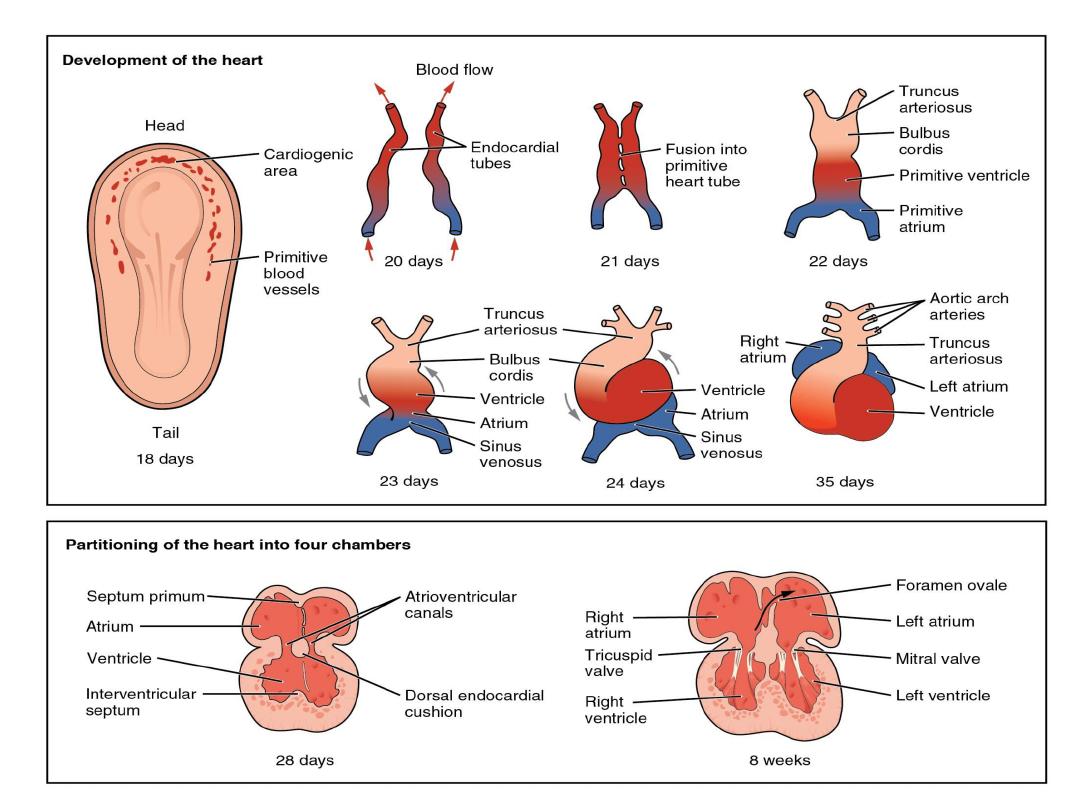

Septum formation in ^ heart
• During ^ 4
th
-7
th
weeks, ^ heart undergoes looping
followed by separation into a typical 4 chambered
structure.
• Septum formation in ^ heart in part arises from
development of endocardial cushion tissue in ^
atrioventricular canal (atrioventricular cushion )&
in ^ conotruncal region (conotruncal swellings).
• Because of key location of cushion tissue, many
cardiac malformations are related to abnormal
cushion morphogenesis.

Septum formation in ^ atrium
• ^ septum primum, a sickle-shaped crest descending
from ^ roof of ^ atrium, begins to divide ^ atrium in
2 but leaves a lumen, ^ ostium primum, for
communication between ^ 2 sides.
• Later, when ^ ostium primum is obliterated by
fusion of ^ septum primum with ^ endocardial
cushions, ^ ostium secondum is formed by cell
death that creates an opening in ^ septum primum.
• Finally, a septum secondum forms, but an
interatrial opening, ^ oval foramen, persists.

• Only at birth, when pressure in ^ LT. atrium
increases, do ^ 2 septa press against each other &
close ^ communication between ^ 2.
• Abnormalities in ^ atrial septum may vary from
total absence to a small opening known as probe
patency of ^ oval foramen.

Septum formation in ^ atrioventricular
canal
• Four endocardial cushions surround ^
atrioventricular canal. Fusion of ^ opposing superior
& inferior cushions divides ^ orifice into RT. & LT.
atrioventricular canals.
• Cushion tissue then becomes fibrous & forms ^
mitral (bicuspid) valve on ^ LT. & ^ tricuspid valve on
^ RT.
• Persistence of ^ common atrioventricular canal&
abnormal division of ^ canal are well-known defects

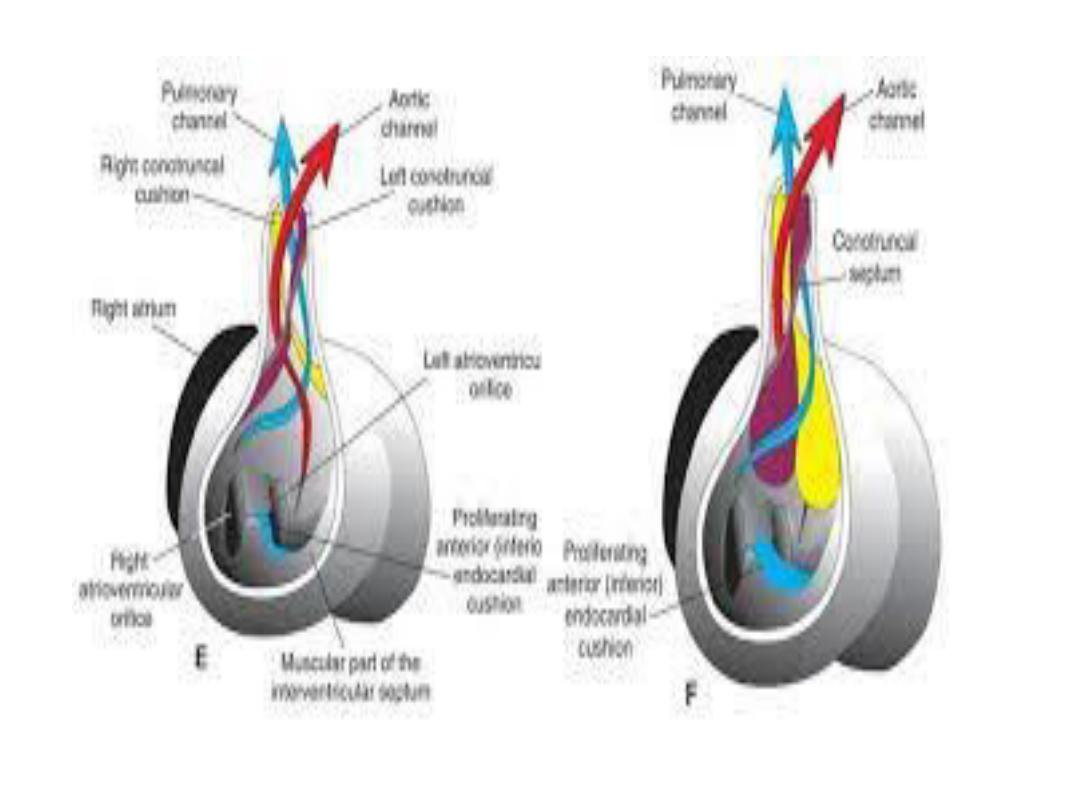
Septum formation in ^ ventricles
• ^ interventricular septum consists of a thick
muscular part & a thin membranous portion,
formed by: (a)-an inferior endocardial
atrioventricular cushion.
(b)-^ RT. Conus swelling.
(c)- ^ LT. conus swelling.
• In many cases, these 3 components fail to fuse,
result in an open interventriculat foramen.
• This abnormality may be isolated, but it is
commonly combined with other defects.

Septum formation in ^ bulbus
• ^ bulbus is divided into:
(a)^ truncus (aorta & pulmonary trunk)
(b)^conus(outflow tract of ^aorta & pulmonary trunk)
(c) ^ trabeculated portion of ^RT. Ventricle.
• ^ truncus region is divided by ^ spiral aorti-
pulmonary septum into ^ 2 main arteries.
• ^ conus swellings divide ^ outflow tracts of ^ aortic
& pulmonary channels & with tissue from ^ inferior
endocardial cushion, close^interventricular foramen

• Many vascular abnormalities, such as
transposition of ^ great vessels & pulmonary
valvular atresia, result from abnormal division of
^ conotruncal region; their origin may involve
neural crest cells that contribute to septum
formation in ^ conotruncal region (i.e.
endocardial cushions in conotruncal region
originate from neural crest cells).