
Acute infectious URT obstruction
stridor, a rasping sound heard predominantly on inspiration
Hoarseness (inflammation of the vocal cords)
a barking cough like a sea lion
a variable degree of dyspnoea
Croup (Laryngotracheobronchitis)
Etiology& Epidemiology
•
Para influenza virus commonest
•
Other viruses
•
Age 3mon.-5years.
•
Higher in boys.
•
Common in late fall& winter.
•
Recurrence frequent 3-6y.
CLINICAL MANIFESTATIONS
•
URTI 1–3 days
•
barking cough, hoarseness, inspiratory stridor.
•
low-grade fever ; some children are afebrile.
•
characteristically worse at night .
•
Agitation and crying aggravate the symptoms.
•
The child prefer to sit up in bed or be held upright.
Physical examination
•
hoarse voice, coryza.
•
normal to moderately inflamed pharynx.
• Rarely, progresses to an increasing respiratory rate; dyspnea; and
continuous stridor.
•
Hypoxia when complete airway obstruction is imminent.
•
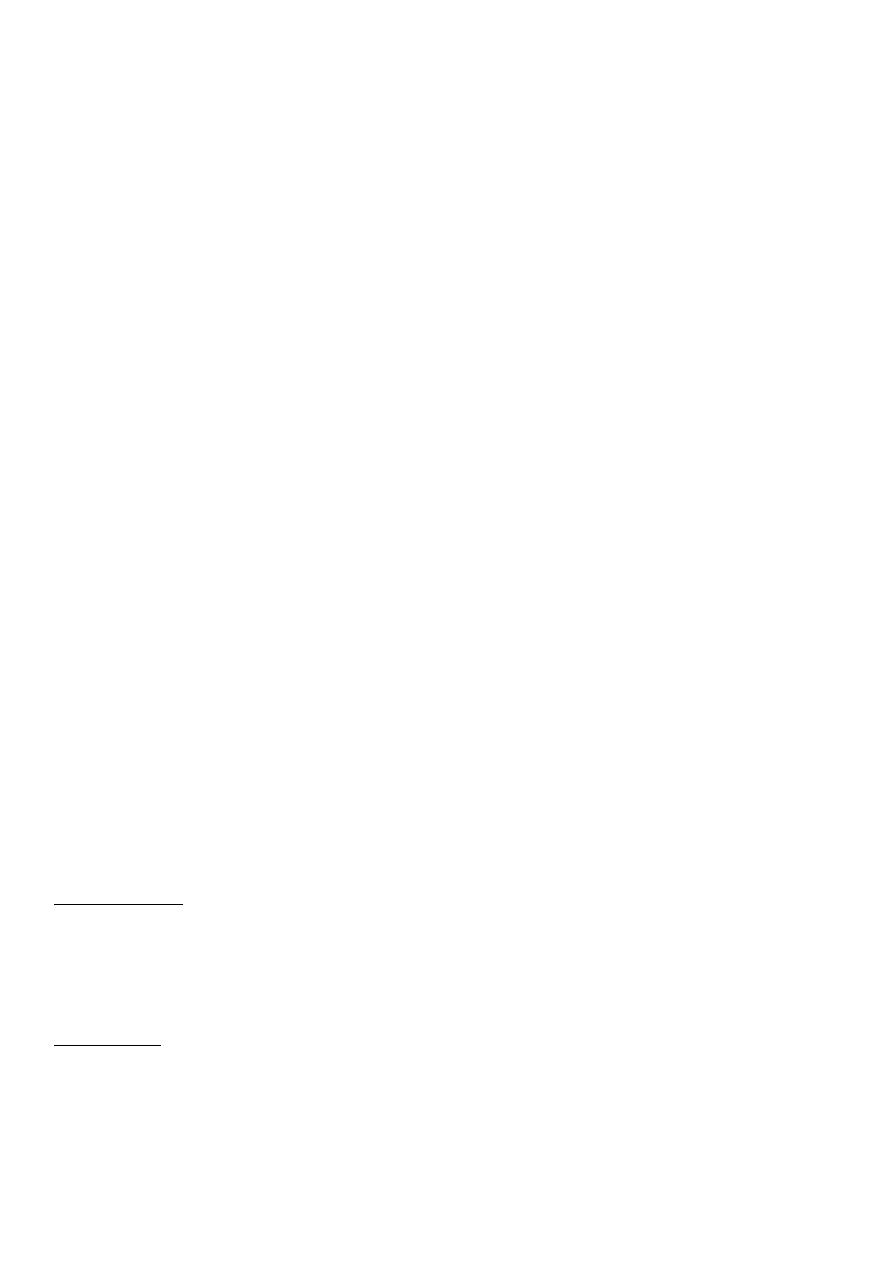
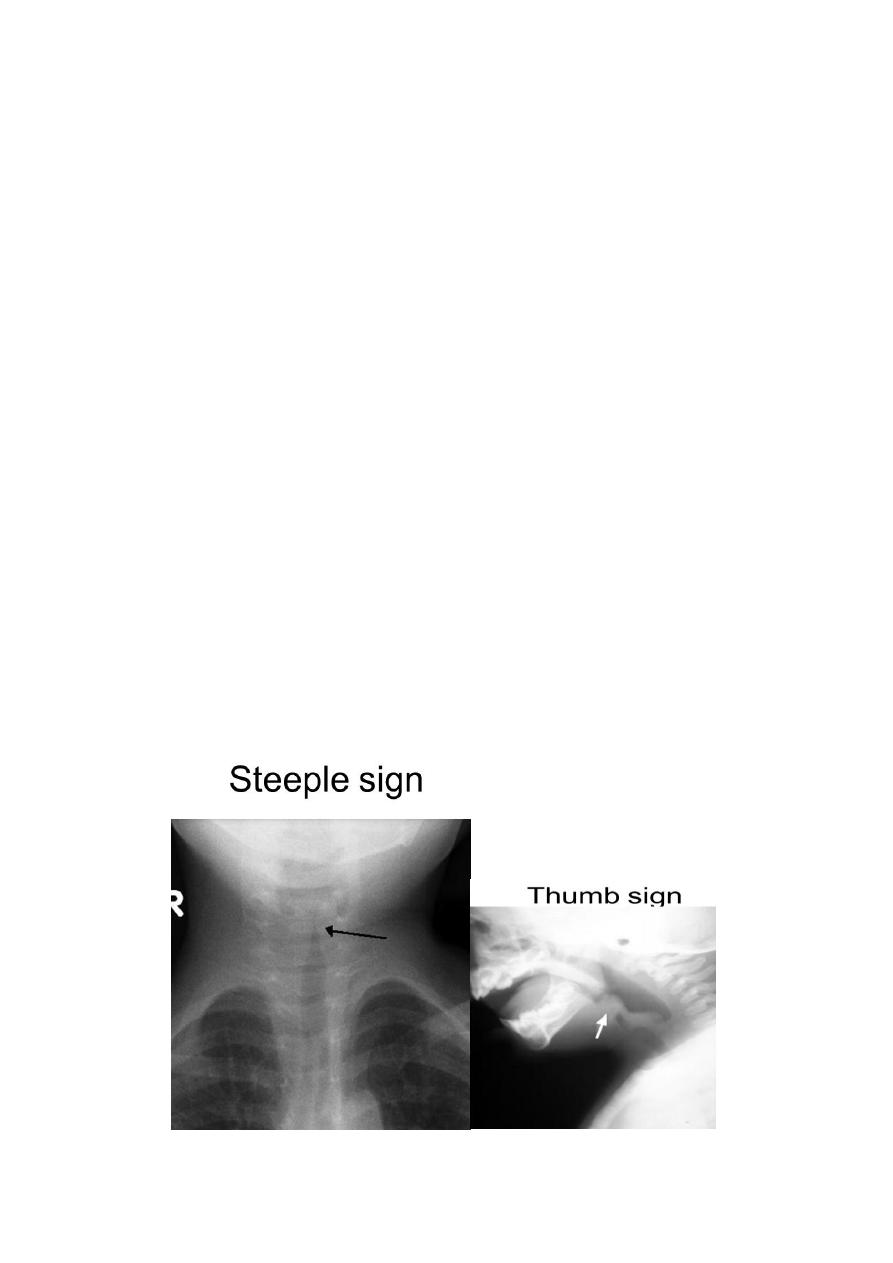
Radiographs of the neck may show
•
subglottic narrowing or “steeple sign”.
•
considered only:-
•
-after airway stabilization in children who
•
have an atypical presentation or clinical

•
course.
•
distinguish between severe
•
laryngotracheobronchitis and epiglottitis.
Acute Epiglottitis (Supraglottitis)
Etiology& Epidemiology
-H.influenza type b in prevaccine era,
age 2-4y.
-strep.pyogen, strep.pneumoniae, staph.
In vaccinated child
Clinical Features
•
dramatic, potentially lethal condition .
•
high fever, sore throat, dyspnea, and rapidly
progressing respiratory obstruction.
•
appears toxic, swallowing is difficult.
•
breathing is labored.
•
Drooling , the neck is hyperextended.
•
tripod position
•
•
rapidly increasing cyanosis and coma.
•
Stridor is a late finding and suggests near-
complete airway obstruction.
•
The diagnosis requires visualization of a
large, “cherry red” swollen epiglottis by
laryngoscopy, (should be performed in an operating room or intensive care
unit).
Anxiety-provoking interventions ( phlebotomy, intravenous line placement,
placing the child supine, or direct inspection of the oral cavity)
should be avoided until the airway is secure.
Classic lateral radiographs show the “thumb sign”
Acute Infectious Laryngitis
•
Laryngitis is a common illness. Viruses cause most cases
Spasmodic Croup
•
occurs most often in children 1–3 yr
•
clinically similar to acute LTB ( history of a
viral prodrome and fever in the patient and
family are frequently absent).
• The cause is viral in some cases, but allergic and psychologic factors could
be.
DIFFERENTIAL DIAGNOSIS
1-Bacterial tracheitis
2-Diphtheritic croup
3- foreign body
4- A retropharyngeal or peritonsillar abscess
5- angioedema of the subglottic areas as part of anaphylaxis .
6-extrinsic compression of the airway (laryngeal web, vascular ring) and
intraluminal obstruction from masses (laryngeal papilloma, subglottic
hemangioma);
.
7-hypocalcemic tetany.
8- infectious mononucleosis, trauma, and tumors or malformations of the larynx.
COMPLICATIONS
viral croup 15% .
Infection of middle ear, terminal bronchioles, pulmonary parenchyma
Bacterial tracheitis If associated with S. aureus, toxic shock syndrome may
develop.
Epiglottitis: Pneumonia, cervical lymphadenitis, otitis media, or, rarely,
meningitis or septic arthritis.
Mediastinal emphysema and pneumothorax are the most common complications
of tracheotomy

TREATMENT
1- Airway management
.
• Mist has been traditionally used to treat croup.. There is no evidence to
support the effectiveness of mist therapy
•
cold night air
•
2- Medications
•
1- Nebulized racemic epinephrine :
•
decrease in
the laryngeal mucosal edema.
•
0.25–0.75 mL of 2.25% racemic
•
epinephrine in 3 mL of normal saline can
•
be used as often as every 20 min.
.
•
The duration of activity of racemic pinephrine
•
is <2 hr. Therefore, observation is mandated.
•
2- Oral or IM dexamethasone used a single dose of 0.6 mg/kg.
•
3- Nebulized budesonide.
•
4- A helium-oxygen mixture (Heliox) may be
•
effective in children with severe croup who may need intubation.
•
Indications of hospitalizations:
1.
progressive stridor.
2.
severe stridor at rest.
3.
respiratory distress.
4.
hypoxia, cyanosis, depressed mental status.
5.
poor oral intake.
6.
the need for reliable observation.
Epiglottitis
is a medical emergency
1-artificial airway placed under controlled conditions, either in an operating room
or intensive care unit. regardless of the degree of apparent respiratory
distress, because lower mortality rate.
2-oxygen . .
3-Cultures of blood, epiglottic surface, and, in selected cases, cerebrospinal fluid
should be collected after airway stabilization.
4-Ceftriaxone, cefotaxime, or a combination of ampicillin and sulbactam should
be given parenterally, antibiotics should be continued for 7–10 days..
Chemoprophylaxis
Indications for rifampin prophylaxis (20 mg/kg orally once a day for 4 days;
maximum dose, 600 mg) :
(1) any contact <48 mo of age who is incompletely immunized;
(2) any contact <12 mo who has not received the primary vaccination series;
(3) an immunocompromised child in the household
PROGNOSIS
.Untreated epiglottitis has a mortality rate of 6%. but if early diagnosis is made
and appropriate treatment is initiated the prognosis is excellent.
The outcome of acute LTB, laryngitis, and spasmodic croup is also excellent.