1
TUMOURS OF THE BRONCHUS AND LUNG
•
Lung cancer is the most common cause of death from cancer world-wide,
causing 1.4 million deaths per year.
•
Tobacco use is the major preventable cause
•
The great majority of tumours in the lung are primary bronchial carcinomas,
and in contrast to many other tumours, the prognosis remains poor,
with
fewer than 30% of patients surviving at 1 year and 6-8 % at 5 years
.
•
Carcinomas of many other organs, as well as osteogenic and other sarcomas,
may cause metastatic pulmonary deposits.
The burden of lung cancer
•
Strikes 900 000 men and 330 000 women each year
•
Accounts
for 18% of all cancer deaths
•
More than a threefold increase in deaths since 1950
•
Rates rising in women: female lung cancer deaths outnumber male in some
Nordic countries
•
Has overtaken breast cancer in several countries, making it the
most
common cause of cancer death in men and women
Primary tumours of the lung
Aetiology
•
Cigarette smoking is by far the most important cause of lung cancer. It is
thought to be directly responsible for
at least 90% of lung carcinomas, the
risk being proportional to the amount smoked and to the tar content of
cigarettes.
•
The death rate from the disease in heavy smokers is 40 times that in non-
smokers. Risk falls slowly after smoking cessation, but remains above that in
non-smokers for many years.
•
It is estimated that 1 in 2 smokers dies from a smoking-related disease.
The
effect of 'passive' smoking is more difficult to quantify but is currently
thought to be a factor in 5% of all lung cancer deaths.
•
Exposure to naturally occurring radon is another risk.
2
•
The incidence of lung
cancer is slightly higher in urban than in rural dwellers,
which may reflect differences in
atmospheric pollution
(including tobacco
smoke)
•
or
occupation
, since a number of industrial materials (e.g. asbestos, silica,
beryllium, cadmium and chromium) are associated with lung cancer.
•
In recent years, the strong link between smoking and ill health has led many
Western governments to legislate against smoking in public places,
•
and smoking prevalence and some smoking-related diseases are already
declining in these countries.
Bronchial carcinoma :
•
The incidence of bronchial carcinoma increased dramatically during
the 20th
century as a direct result of the tobacco epidemic
.
•
In women, smoking prevalence and deaths from lung cancer continue to
increase, and more women now die of lung cancer than breast cancer in the
USA and the UK.
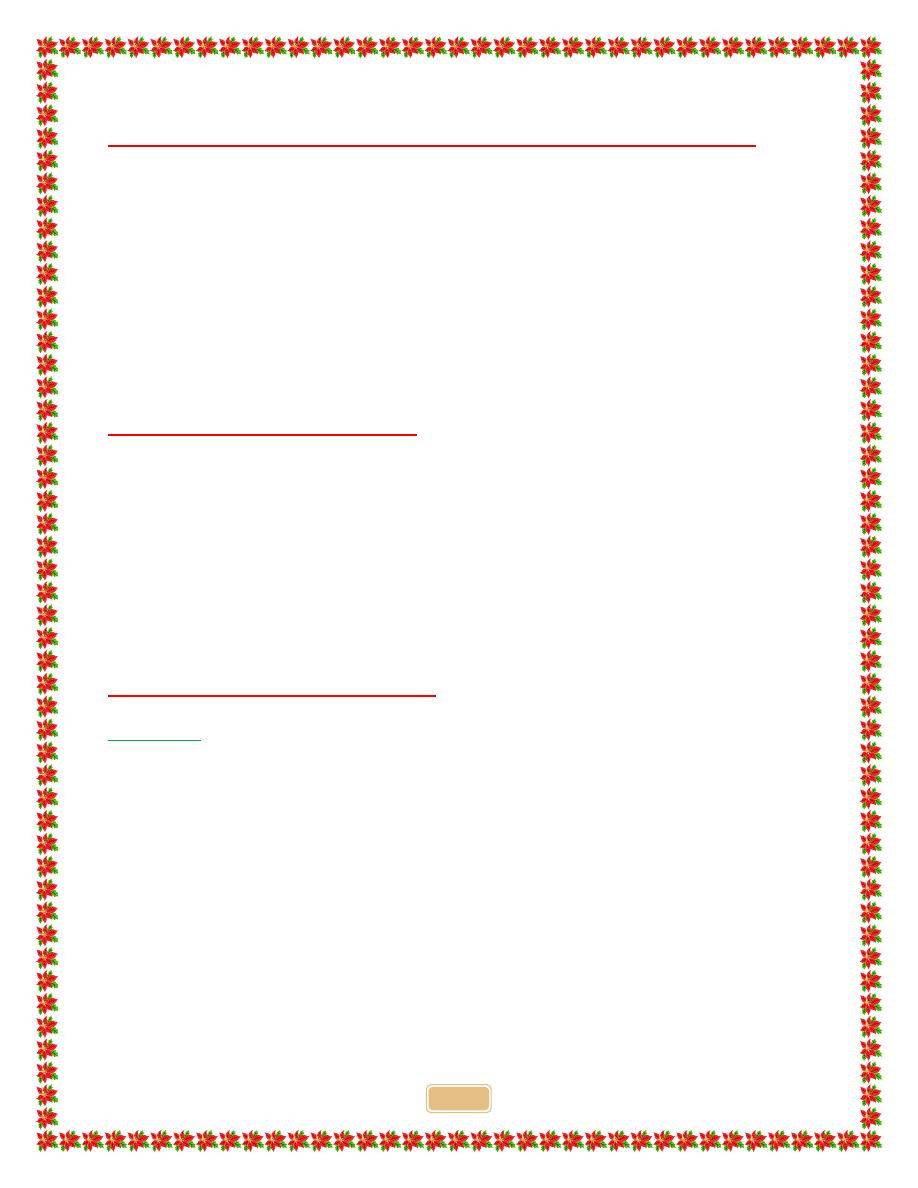
Mortality trends from lung cancer in England and Wales, 1950-2004 by age
and year of death. Note the decline in mortality from lung cancer in men
towards the end of this period, reflecting a change in smoking habit.
3
Pathology
Common cell types in bronchial carcinoma Cell type
•
Squamous 35 %
•
Adenocarcinoma 30 %
•
Small-cell 20 %
•
Large-cell 15 %
•
Bronchial carcinomas arise from the bronchial epithelium or mucous
glands.
•
When the tumour occurs in a large bronchus, symptoms arise early, but
tumours originating in a peripheral bronchus can grow very large without
producing symptoms, resulting in delayed diagnosis.
•
Peripheral squamous tumours may undergo central
necrosis and
cavitation, and may resemble a lung abscess on X-ray
.
Bronchial carcinoma may involve the pleura either directly or by lymphatic spread
and may extend into the chest wall, invading the
intercostal nerves or the brachial plexus and
causing pain
•
Lymphatic spread to mediastinal and
supraclavicular lymph nodes frequently
occurs prior to diagnosis.
•
Blood-borne metastases occur most
commonly in
liver, bone, brain, adrenals and
skin.
•
Even a small primary tumour may cause
widespread metastatic deposits and this is
a particular characteristic
of small-cell
lung cancers.
4
•
Lung cancer presents in many
different ways, reflecting
local, metastatic or
paraneoplastic tumour
effects.
•
Cough
.
The most common
early symptom, cough is often
dry; however, secondary
infection may cause purulent
sputum.
•
A change in the character of
a smoker's cough, particularly
if associated with other new
symptoms, should always raise
suspicion of bronchial
carcinoma.
•
Haemoptysis
.
This is
common, especially with
central bronchial tumours.
Although it frequently
accompanies bronchitic
infection and may be benign, haemoptysis in a smoker should always be
investigated to exclude a bronchial carcinoma.
•
Occasionally, central tumours invade large vessels, causing sudden massive
haemoptysis which may be fatal.
Bronchial obstruction
.
•
This is another common presentation, and the clinical and radiological
manifestations depend
on the site and extent of the obstruction, any
secondary infection, and the extent of coexisting lung disease.
•
Complete obstruction causes collapse of a lobe or lung, with breathlessness,
mediastinal displacement and dullness to percussion with reduced breath
sounds.
•
Partial bronchial obstruction
may cause a monophonic, unilateral wheeze
that fails to clear with coughing and may also impair the drainage of
secretions sufficiently to cause pneumonia or lung abscess as a presenting
problem.
5
•
Pneumonia that recurs at the same site or responds slowly to treatment,
particularly in a smoker, should always suggest an underlying bronchial
carcinoma.
•
Stridor (a harsh inspiratory noise) occurs when the lower trachea, carina or
main bronchi are narrowed by the primary tumour or by compression from
malignant enlargement of the subcarinal and paratracheal lymph nodes.
Breathlessness
.
•
This may be caused by collapse or pneumonia, or by tumour causing a large
pleural effusion or compressing a phrenic nerve causing diaphragmatic
paralysis.
Pain and nerve entrapment
.
•
Pleural pain usually indicates malignant pleural invasion, although it can occur
with distal infection.
•
Intercostal nerve involvement causes pain in the distribution of a thoracic
dermatome.
•
Carcinoma in the lung apex may cause
Horner's syndrome
(ipsilateral
partial ptosis, enophthalmos, miosis and hypohidrosis of the face) due to
involvement of the sympathetic chain at or above the stellate ganglion.
•
Pancoast's syndrome
(pain in the shoulder and inner aspect of the arm,
sometimes with small muscle wasting in the hand)
indicates malignant
destruction of the T1 and C8 roots in lower part of the brachial plexus by an
apical lung tumour.
6
Mediastinal spread
.
•
Involvement of the oesophagus may cause dysphagia.
•
If the pericardium is invaded, arrhythmia or pericardial effusion may occur.
•
Superior vena cava obstruction
by malignant nodes causes suffusion and
swelling of the neck and face, conjunctival oedema, headache and dilated
veins on the chest wall, and is most commonly due to bronchial carcinoma.
•
Involvement of the left recurrent laryngeal nerve by tumours at the left
hilum causes vocal cord paralysis,
voice alteration and a 'bovine' cough
(lacking the normal explosive character).
•
Supraclavicular lymph nodes may be palpably enlarged; if so, a needle
aspirate may provide a simple means of cytological diagnosis.
Metastatic spread
.
•
This may lead to focal neurological defects, epileptic seizures, personality
change, jaundice, bone pain or skin nodules. Lassitude, anorexia and weight
loss usually indicate metastatic spread.
Digital clubbing
.
•
Overgrowth of the soft tissue of the terminal phalanx leading to increased
nail curvature is often seen.
•
This may be associated with hypertrophic pulmonary osteoarthropathy
(HPOA), characterised by periostitis of the long bones, most commonly the
distal tibia, fibula, radius and ulna.
•
This causes pain and tenderness over the affected bones and often pitting
oedema over the anterior aspect of the shin.
7
Non-metastatic extrapulmonary manifestations
of bronchial carcinoma
Endocrine
•
Inappropriate antidiuretic hormone secretion causing
hyponatraemia(associatedusually with small cell ca.)
•
Ectopic adrenocorticotrophic hormone secretion
•
Hypercalcaemia due to secretion of parathyroid hormone-related peptides
•
Carcinoid syndrome .
•
Gynaecomastia
Neurological
•
Polyneuropathy
•
Myelopathy
•
Cerebellar degeneration
•
Myasthenia (Lambert-Eaton syndrome)
Other
•
Digital clubbing
•
Hypertrophic pulmonary osteoarthropathy
•
Nephrotic syndrome
•
Polymyositis and dermatomyositis
•
Eosinophilia
8
Investigations
•
The main aims of investigation
are to confirm the diagnosis, establish the
histological cell type and define the extent of the disease.
1- Imaging
•
plain X-rays
•
CT is
usually performed early, as it may reveal mediastinal or metastatic
spread, and helps to direct histological sampling procedures.
•
Imaging also indicates whether a tumour is likely to be accessible by
bronchoscopy.
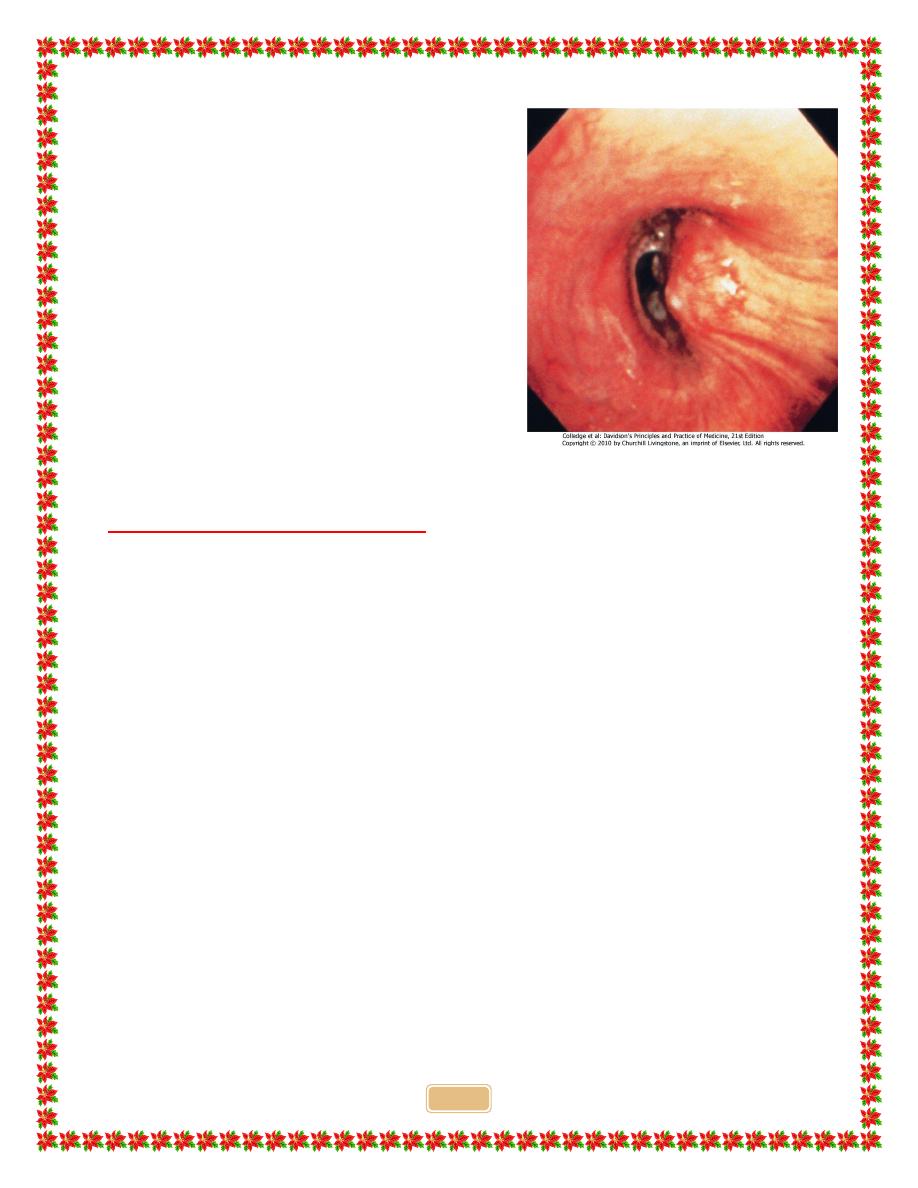
2- Histological characterisation
Around three-quarters
of primary lung tumours can be visualised and
sampled directly by biopsy and brushing using a flexible bronchoscope.
Bronchoscopy
also allows an assessment of operability, from the proximity of
central tumours to the main carina .
•
For tumours which are too peripheral to be accessible by bronchoscope, the
yield of 'blind' bronchoscopic washings and brushings from the radiologically
affected area is low, and percutaneous needle biopsy under CT or ultrasound
guidance is a more reliable way to obtain a histological diagnosis.
•
There is a small risk of iatrogenic pneumothorax, which may preclude the
procedure if there is
extensive coexisting COPD in the remaining lung
.
•
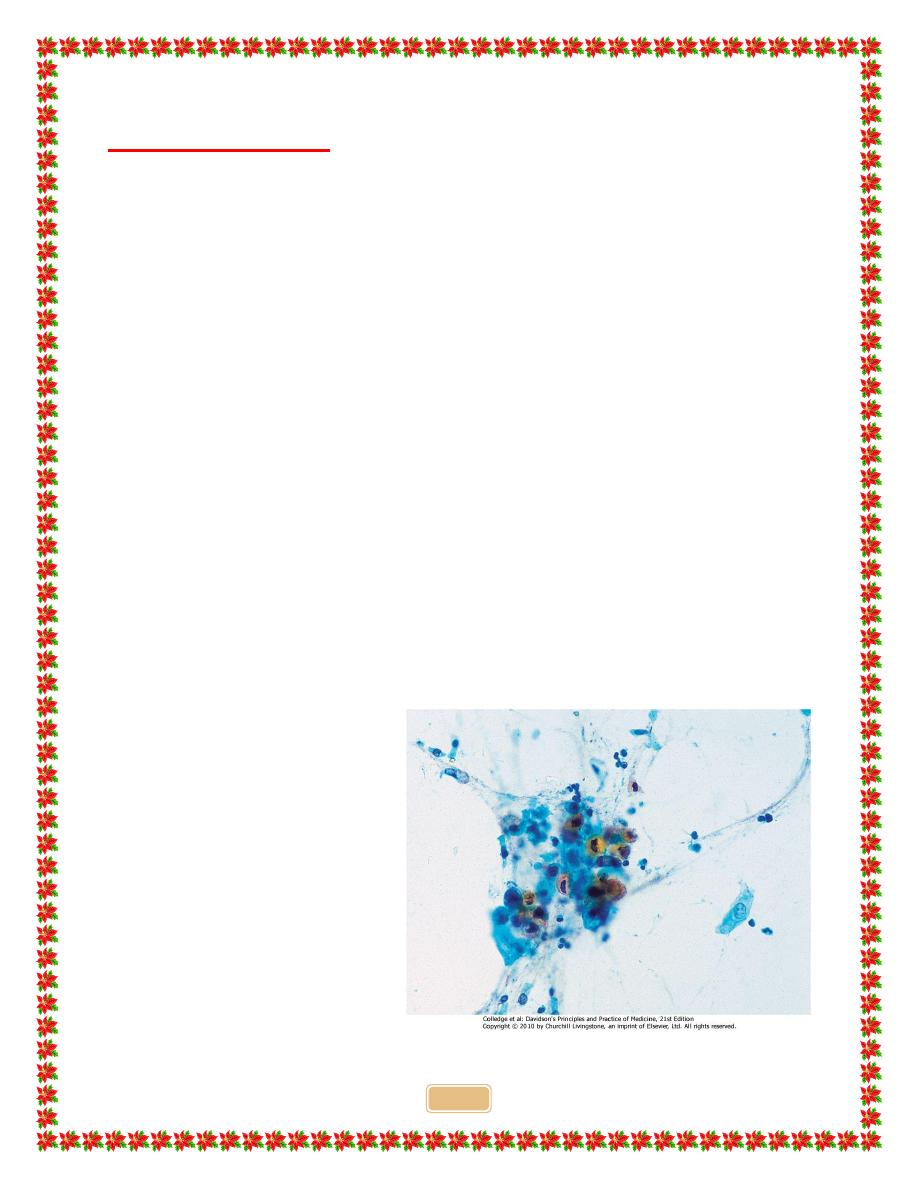
In patients who are not fit enough for invasive investigation,
at least three
sputum samples should be
obtained for cytology,
which may confirm the
diagnosis non-invasively
9
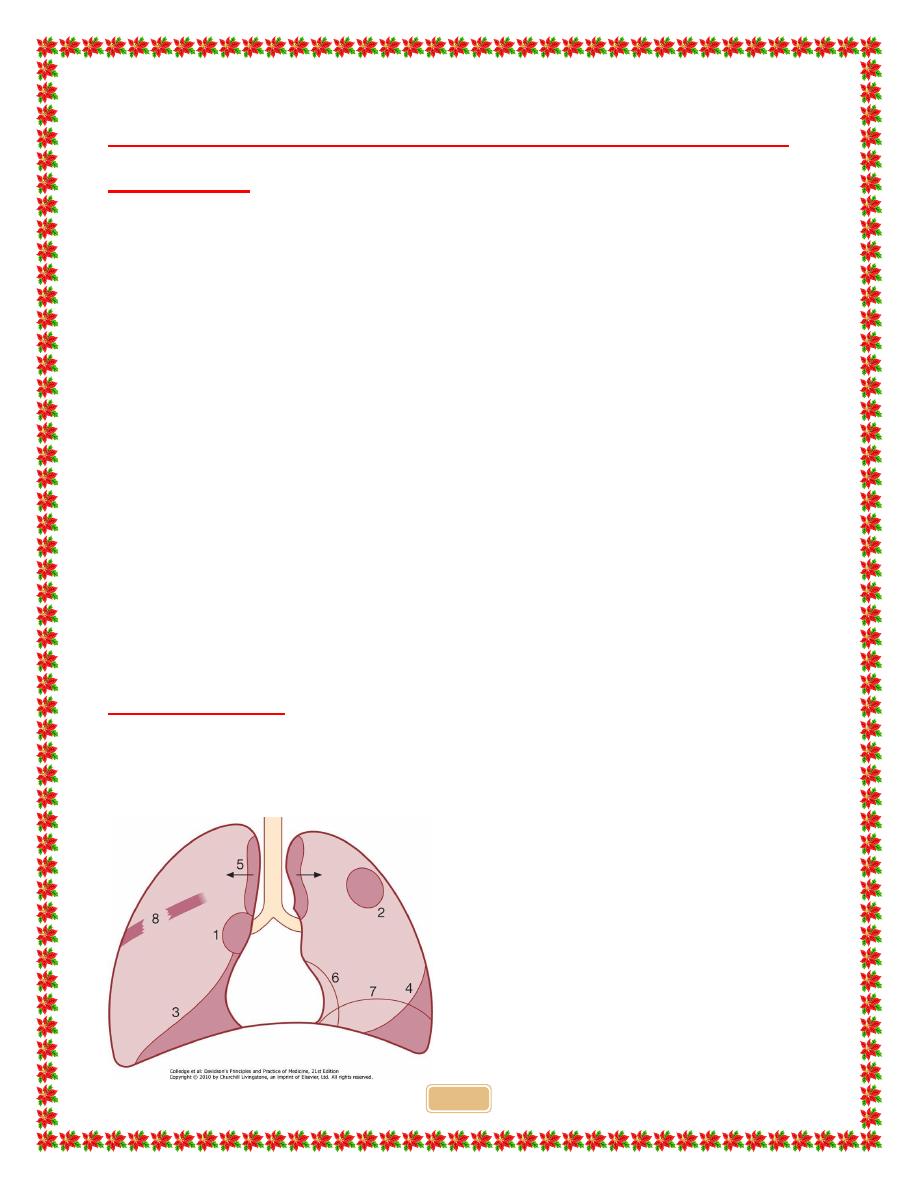
Common radiological presentations of bronchial
carcinoma
•
Unilateral hilar enlargement Central tumour.
Hilar glandular involvement.
However, a peripheral tumour in the apical segment of a lower lobe can look
like an enlarged hilar shadow on the PA X-ray
•
Peripheral pulmonary opacity
Usually irregular but well circumscribed, and
may contain irregular cavitation. Can be very large
•
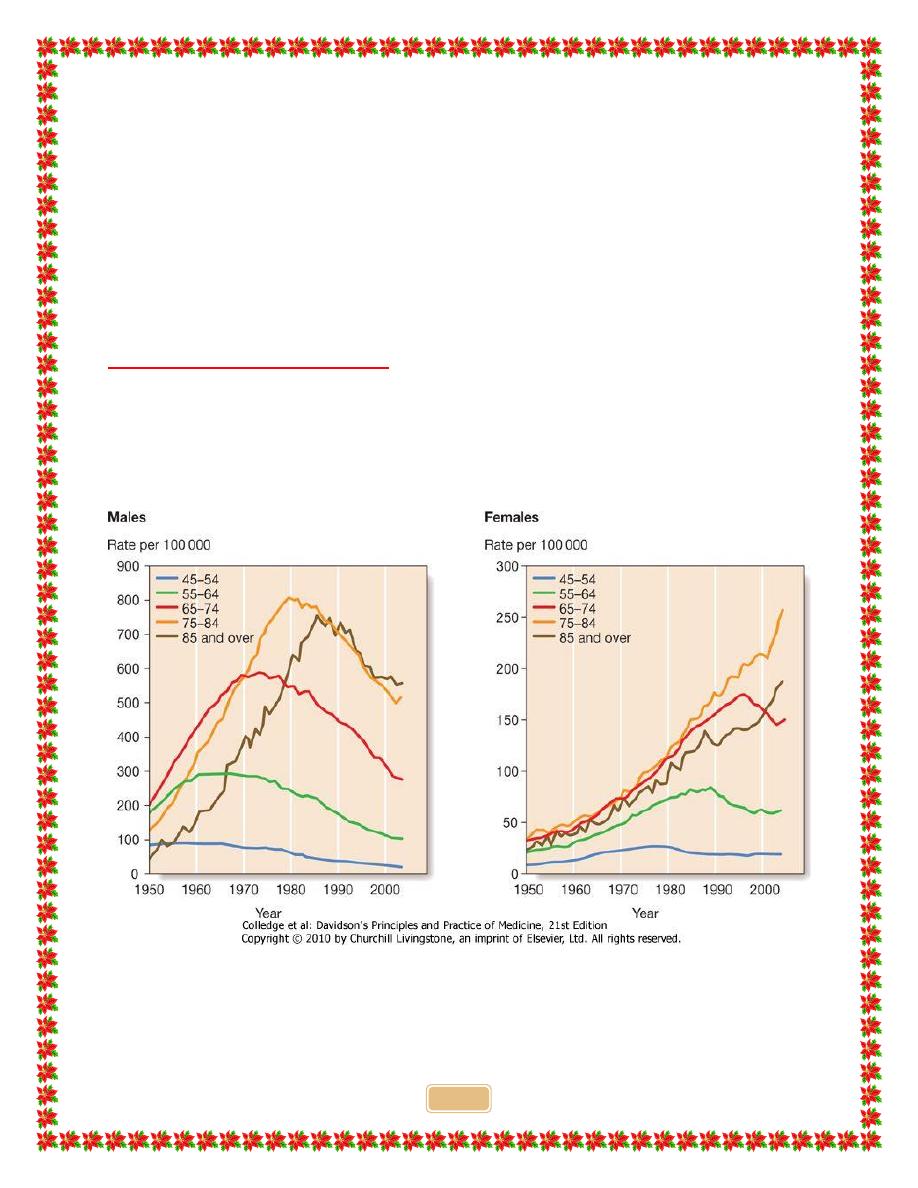
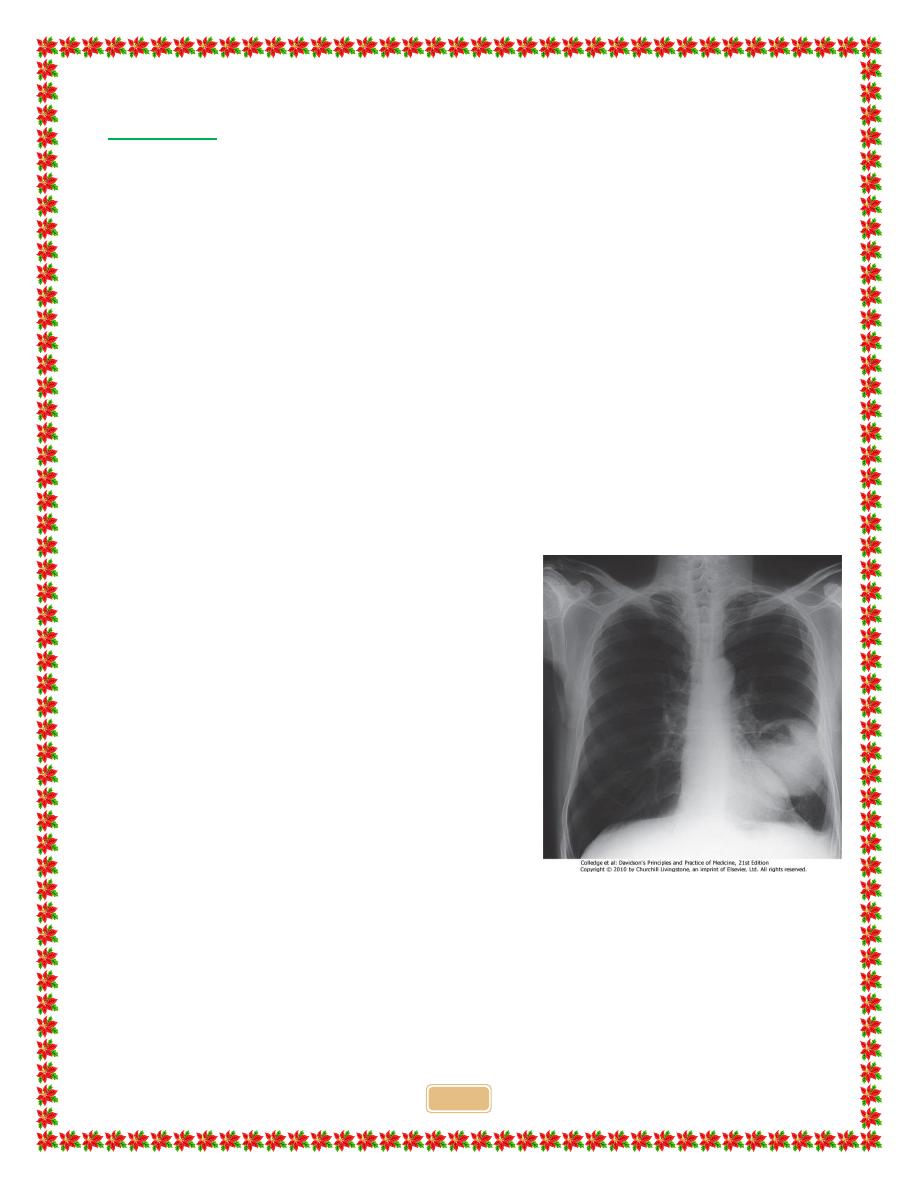
Lung, lobe or segmental collapse
Usually caused by tumour within the
bronchus leading to occlusion. Lung collapse may be due to compression of
the main bronchus by enlarged lymph glands
•
Pleural effusion
Usually indicates tumour invasion of pleural space; very
rarely, a manifestation of infection in collapsed lung tissue distal to a
bronchial carcinoma
Broadening of mediastinum, enlarged cardiac shadow, elevation of a
hemidiaphragm
Paratracheal lymphadenopathy may cause widening of the upper mediastinum. A
malignant pericardial effusion will cause enlargement of the cardiac shadow.
If a raised hemidiaphragm is caused by phrenic nerve palsy, screening will show it
to move paradoxically upwards when patient sniffs
Rib destruction
Direct invasion of the chest wall or blood-borne metastatic spread can cause
osteolytic lesions of the ribs
10
•
In patients with pleural effusions,
pleural
aspiration and biopsy is the preferred
investigation
.
•
Where facilities exist, thoracoscopy
increases yield by allowing targeted
biopsies under direct vision.
•
In patients with metastatic disease, the
diagnosis can often be confirmed by
needle aspiration or
biopsy of affected
lymph nodes, skin lesions, liver or bone
marrow.
Staging to guide treatment
•
The propensity of small-cell lung cancer to metastasise early dictates that
patients with this tumour type are usually
not suitable for surgical
intervention.
•
In patients with other cell types, subsequent investigations should focus on
determining whether the tumour is operable
, because complete resection
may be curative.
•
While CT may show obvious spread of disease, for many patients the results
are equivocal and further investigation is required before deciding whether
curative surgery is feasible.
•
Enlarged upper mediastinal nodes may be sampled by using a bronchoscope
equipped with
endobronchial ultrasound (EBUS) or by mediastinoscopy.
•
Nodes in the lower mediastinum can be sampled through the oesophageal wall
using endoscopic ultrasound.
•
Combined
CT and PET imaging
is used increasingly to detect metabolically
active tumour metastases.
•
Head CT, radionuclide bone scanning, liver ultrasound and bone marrow
biopsy
are generally reserved for patients with clinical, haematological or
biochemical evidence of tumour spread to such sites.
11
•
Finally, detailed physiological testing is required to ensure that the patient's
respiratory and cardiac function is sufficient to allow surgical treatment.
Contraindications to surgical resection in bronchial
carcinoma
•
Distant metastasis (M1)
•
Invasion of central mediastinal structures including heart, great vessels,
trachea and oesophagus (T4)
•
Malignant pleural effusion (T4)
•
Contralateral mediastinal nodes (N3)
•
FEV
1
< 0.8 L
•
Severe or unstable cardiac or other medical condition
Management
•
Surgical resection carries the best hope of long-term survival; however,
some patients treated with radical radiotherapy and chemotherapy also
achieve prolonged remission or cure.
•
Unfortunately,
in over 75% of cases, treatment with curative intent is not
possible, or is inappropriate due to extensive spread or comorbidity.
Such
patients can only be offered palliative therapy and best supportive care.
•
Radiotherapy, and in some cases chemotherapy, can relieve distressing
symptoms.
Surgical treatment
•
Accurate pre-operative staging, coupled with improvements in surgical and
post-operative care, now offers 5-year survival rates of over 75% in stage I
disease (N0, tumour confined within visceral pleura) and 55% in stage II
disease, which includes resection in patients with ipsilateral peribronchial or
hilar node involvement.
12
Radiotherapy
•
While much less effective than surgery, radical radiotherapy can offer long-
term survival in selected patients
with localised disease in whom comorbidity
precludes surgery.
•
The greatest value of radiotherapy, however, is in the palliation of
distressing complications
such as superior vena cava obstruction, recurrent
haemoptysis, and pain caused by chest wall invasion or by skeletal metastatic
deposits.
•
Obstruction of the trachea and main bronchi can also be relieved
temporarily.
•
Radiotherapy can be used in conjunction with chemotherapy in the
treatment of small-cell carcinoma, and is particularly efficient at preventing
the development of brain metastases in patients who have had a complete
response to chemotherapy.
Chemotherapy
•
The treatment of small-cell carcinoma with combinations of cytotoxic drugs,
sometimes in combination with radiotherapy, can increase the median
survival from 3 months to well over a year.
•
Combination chemotherapy leads to better outcomes than single-agent
treatment.
•
In general, chemotherapy is less effective in non-small-cell bronchial
cancers. However, studies in such patients using platinum-based
chemotherapy regimens have shown a 30% response rate associated with a
small increase in survival.
Neoadjuvant and adjuvant chemotherapy
•
In non-small-cell carcinoma, there is some evidence that chemotherapy given
before surgery may increase survival and can effectively 'down-stage'
disease with limited nodal spread.
•
Post-operative chemotherapy is now proven to improve survival rates when
operative samples show nodal involvement by tumour.
13
Laser therapy and stenting
•
Palliation of symptoms caused by major airway obstruction can be achieved in
selected patients using bronchoscopic laser treatment to clear tumour tissue
and allow re-aeration of collapsed lung.
•
The best results are achieved in tumours of the main bronchi. Endobronchial
stents can be used to maintain airway patency in the face of extrinsic
compression by malignant nodes.
General aspects of management
•
The best outcomes are obtained when lung cancer is managed in specialist
centres by multidisciplinary teams including oncologists, thoracic surgeons,
respiratory physicians and specialist nurses; effective communication, pain
relief and attention to diet are important.
•
Lung tumours can cause clinically significant depression and anxiety, and
these may need specific therapy. The management of non-metastatic
endocrine manifestations .
•
When a malignant pleural effusion is present, an attempt should be made to
drain the pleural cavity using an intercostal drain; provided the lung fully re-
expands, pleurodesis with a sclerosing agent such as talc should be
performed.
Prognosis
•
The overall prognosis in bronchial carcinoma is very poor, with around 70% of
patients dying within a year of diagnosis and only 6-8% of patients surviving
5 years after diagnosis.
•
The best prognosis is with well-differentiated squamous cell tumours that
have not metastasised and are amenable to surgical resection.