1
P a g e
|
Perforated peptic ulcer
- Despite the widespread use of gastric anti-secretory agents and
eradication therapy, the incidence of perforated peptic ulcer has changed
little,
age limits increase
NSAIDs elderly
Anterior d.u& incisura g.u most common perforate
Clinical features
History of peptic ulceration
sudden-onset, severe generalized abdominal pain as a result of the
irritant effect of gastric acid on the peritoneum
bacterial peritonitis supervenes over a few hours
patient may be shocked with a tachycardia
abdomen exhibits a board-like rigidity
The abdomen does not move with respiration
Very frequently, the elderly patient who is taking NSAIDs will have a
less dramatic presentation, board-like rigidity not observed
Difficult diagnosis:
potent analgesic effect of NSAID
Small perforation
Posterior g,u perforation to lesser sac
Sealed perforation
Diabetic patient(silent)
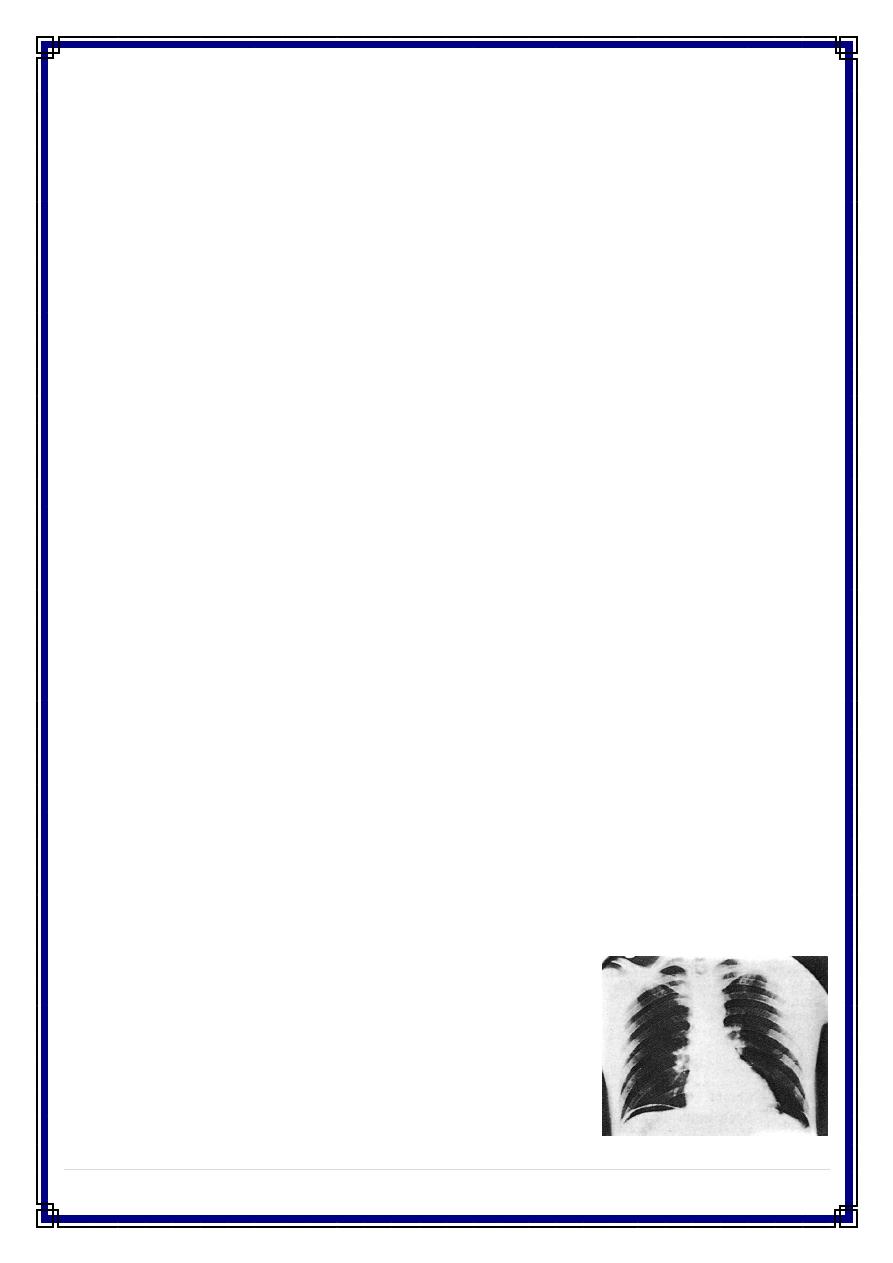
Investigations
An erect plain chest radiograph will reveal free gas under the
diaphragm in more than 50% of cases
CT scan imaging is more accurate
S .amylase to distinguish from pancreatitis
Treatment
resuscitation and analgesia
Laparotomy
2
P a g e
|
thorough peritoneal toilet to remove all of the fluid and food debris
Duodenal perf. it can usually be closed by several well-placed sutures,
closing the ulcer in a transverse direction
omental patch =leak sealing
Massive duodenal or gastric perforation=Billroth II gastrectomy
Gastric ulcers should, if possible, be excised and closed, so that
malignancy can be excluded
definitive procedures TV+PP or HSV: in well-selected patients and in
expert hands this is a very safe strategy
Minimally invasive techniques if the expertise is available
Anti h. pylori + ppi post op.
Conservative management of perforated ulcer
- Patients with a delayed presentation (i.e. greater than 24 hours) and
extensive co-morbid factors.
- In patients who are hemodynamically stable with minimal abdominal
symptoms
Causes of upper gastrointestinal bleeding
Condition Incidence (%)
Ulcers 60
- Esophageal 6
- Gastric 21
- Duodenal 33
Erosions 26
- Esophageal 13
- Gastric 9
- Duodenal 4
Mallory–Weiss tear 4
Esophageal varices 4
Tumor 0.5
Vascular lesions, e.g. Dieulafoy’s disease 0.5
Others 5
3
P a g e
|
Bleeding peptic ulcers
- In recent years, the population affected has become much older and the
bleeding is commonly associated with the ingestion of NSAIDs
- The three cardinal principles in the management are:
1- Vigorous resuscitation of the initial bleed to restore hemodynamic
stability, followed by monitoring for re-bleeding and appropriate
resuscitation if this should occur.
2- Prompt investigation to establish the cause.
3- Institution of appropriate measures to arrest bleeding and prevent
further hemorrhage.
- Upper gastrointestinal endoscopy should be carried out by an
experienced operator
- In patients in whom the bleeding is relatively mild, endoscopy may be
carried out on the morning after admission.
- In all cases of severe bleeding it should be carried out immediately
Medical and minimally interventional treatments
- proton pump antagonist
- tranexamic acid, an inhibitor of fibrinolysis, reduces the re-bleeding rate
- injection of the bleeding ulcer with adrenaline or sclerosant,
- laser photocoagulation
- coagulation with bipolar diathermy
Surgical treatment
- if bleeding persists, or recurs despite endoscopic intervention surgery,
should attempted
- factors which should encourage surgical intervention
A large vessel, visible in the ulcer base
a major initial bleed,
a re-bleed in hospital
advanced age
Patient who has required more than 6 units
- The aim of the operation is to stop the bleeding
- The most common site of bleeding from a peptic ulcer is the duodenum
4
P a g e
|
- the duodenum, and usually the pylorus, are opened longitudinally
- bleeding controlled by using well-placed sutures that under-run the vessel
- Pyloroplasty is then closed with interrupted sutures in a transverse
direction
- Bleeding G.U same line +biopsy or excision
- Definitive acid lowering surgery is not now required
- very large ulcer eroding into a major branch of the left gastric artery may
necessitate a subtotal gastrectomy incorporating the ulcer
GASTRIC OUTLET OBSTRUCTION
- gastric outlet obstruction should be considered malignant until proven
otherwise
- Clinical features
In benign gastric outlet obstruction there is usually a long history of
peptic ulcer disease
pain may become unremitting and in other cases it may largely
disappear
vomitus is characteristically unpleasant in nature and is totally lacking
in bile, recognize foodstuff taken several days previously
Examination wt loss, unwell look, dehydrated
Succession splash +ve
- Metabolic effects
- Acid loss
- hypochloraemic alkalosis
- initially, sodium and potassium levels may be relatively normal
- Initially, the urine has a low chloride and high bicarbonate content
- Progressive hyponatremia
- Dehydration
- Na retention
- Potassium and hydrogen are excreted
- Urine becoming paradoxically acidic
- hypokalemia
5
P a g e
|
Management
- aim
correcting the metabolic abnormality
dealing with the mechanical problem
intravenous isotonic saline with potassium Supplementation
stomach should be emptied using a wide-bore gastric tube.+ lavage the
stomach
- Investigation
FBC,s. electrolyte,
Endoscopy biopsy to exclude malignancy.
Contrast radiology
- Treatment
an anti-secretory agent, initially given intravenously
severe cases are treated surgically, usually with a gastroenterostomy
rather than a pyloroplasty
Endoscopic treatment with balloon dilatation has been practised and
may be most useful in early case
Causes of gastric outlet obstruction
- Ca stomach
- Peptic ulcer
- Adult pyloric stenosis
- Pyloric mucosal diaphragm
Intractability/Non-healing
- rare indication for operation nowadays Surgical treatment should be
considered in patients with
- non-healing or intractable peptic ulcer who have multiple recurrences,
- Large ulcers (>2 cm),
- complications (obstruction, perforation or hemorrhage), or
- suspected gastric cancer
Done by: #MOHDZ Dr.Loay – Surgery