
Lec.1
sixth stage
2016\7\17
Pediatrics
د.ندى العلي
An approach to a child with oedema
Oedema: accumulation excess interstitial fluid
Increased hydrostatic pressure
o Acute nephritic syndrome
o Congestive cardiac failure
Decreased plasma oncotic pressure
o Protein calorie malnutrition, Nephrotic syndrome; protein
loosing enteropathy
Increased capillary leakage
o Allergy, sepsis, angiooedema.
Impaired venous flow
o Vanacaval obstruction, hepatic vein obstruction
Impaired lymphatic flow
o Congenital lymphedema, Wuchereria bancrofti infection
Examples for formulation of questions
Localized oedema
o Insect bite; trauma; skin infections
o Kwashiorkar (bilateral pedal)
o Superior vanacaval obstruction
o Lymphatic obstruction

o Orthostatic
Generalized oedema
o Renal: periorbital; hematuria; hypertension; symptoms of
collagen disease (rash, joint pain); frothy urine; symptoms
of uraemia (vomiting, nausea, pallor), convulsion, low urine
output.
Examples for formulation of questions
Cardiac: orthopnoea, joint pain; palpitation; giddiness; fainting
episodes; bluish episodes;
Protein energy malnutrition: low calorie and protein in the diet for
long; precipitating factors (persistent diarrhea, chronic illnesses)
Hepatic: Jaundice; ascites; prominent abdominal veins; neonatal
umbilical sepsis; spleenomegaly; purpura
Collagen diseases: fever, rash, joint pain, pallor
First case
4 year old girl, who recently recovered from a sore throat, was
brought to the OPD with symptoms of swelling of both feet. Physical
examination reveals edema around the eyes and the ankle. A routine
urinalysis reveals the following results.
UrinChemical/Physical Analysis Color:Yellow’
Blood:Moderate;Clarity:Hazy;pH:6.5
Glucose:Negative;Protein:300mg/dL;Ketones:Negative
Specific Gravity:1.015 ;Nitrite:Negative
Microscopic Analysis
20-50 RBC/hpf
10-20 WBC/hpf

2-5 RBC casts/hpf
2-5 Granular casts/hpf
Second case
5 year male child
Swelling first noticed around eyes.
No history of shortness of breath; fever; cough; jaundice; umbilical
infection; no dark colored urine.
Height: 110cms; Wt: 18kg; liver not enlarged; Ascites present
Third case12 year male from Pokhara; arrived after traveling by
bus for 12 hours.
History of fever
Upper abdominal pain
Dark colored urine
No past history of sore throat, rash, joint pain diarrhea, trauma.
o
Comfortably lying flat in bed
o
Oral temp: 40C
o
Respiratory rate: 28.min
o
Bilateral pedal edema, non tender
o
Absence of Jaundice
o
Weight: 38 Kg.
o
Chest: normal
o
Abdomen: Tender R hypo. No free fluid

Third case:
Normal blood count
Urine: routine normal
Liver function: normal
X-ray chest: normal
What causes we have excluded?
Increased hydrostatic pressure?
Decreased plasma oncotic pressure?
Increased capillary leakage?
Impaired venous flow?
Impaired lymphatic flow?
Third case: further investigation
Bilateral edema and tender R hypochondrium.
Ultrasound of the abdomen:
o Thickened Gall Bladder wall
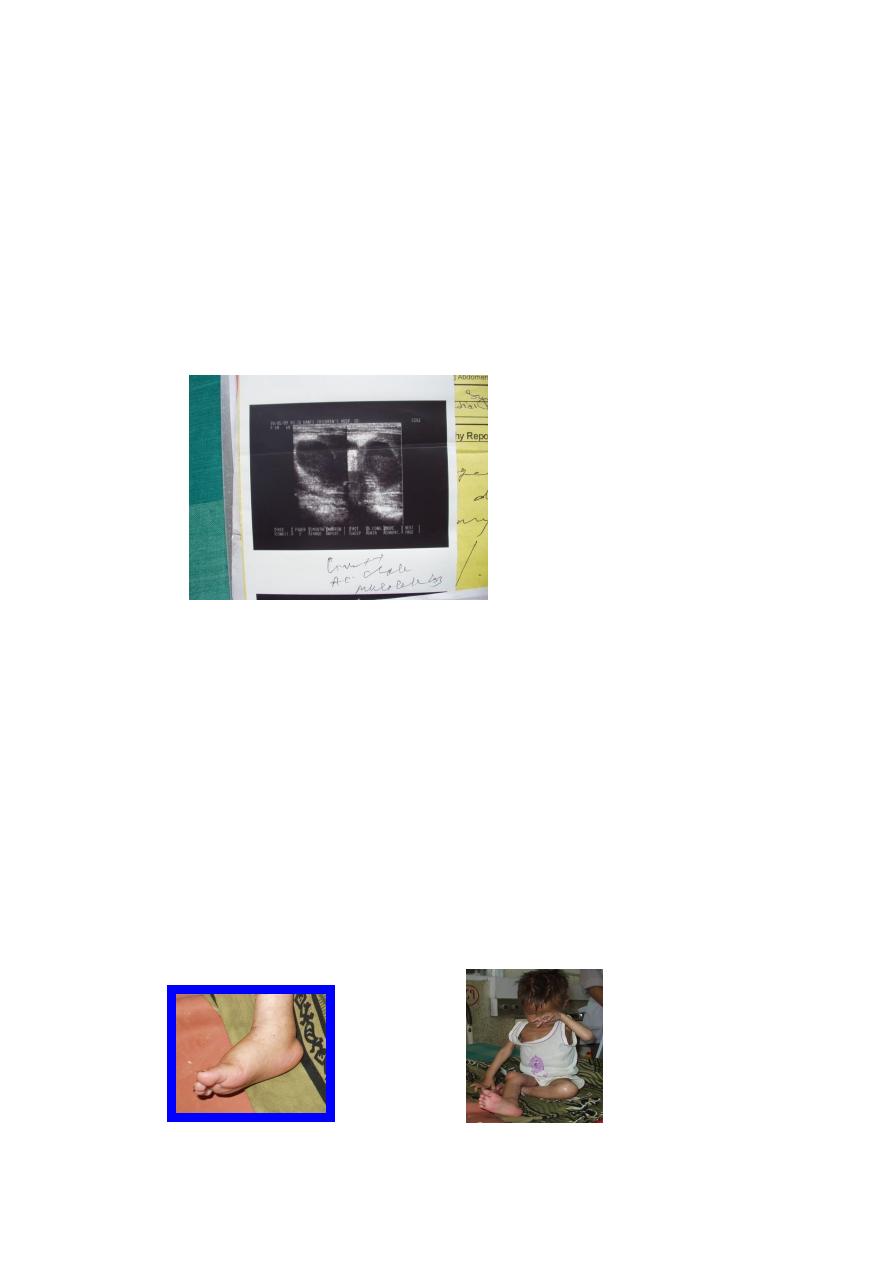
o Mucocoele
Third case :Final diagnosis and pathophysiology
Edema: increased hydrostatic pressure due to gravitational effect
from prolonged leg hanging.
R. Hypochondrium pain and fever: cholecystitis and mucocele of
gall bladder (ultrasound supported)
Fourth case
5 year male child
Swelling started from limb : one month
No history of cough, shortness of breath, cyanosis, jaundice, dark
colored urine, umbilical infection.
Persistent diarrhea +.
Irritable; wt: 12 kg; Ht: 100cms. Serum protein: 1.5G/dL; Urine
normal
l
