
Taking a Psychiatric History: Notes by Jason Hancock
www.askdoctorclarke.com 1
Taking a Psychiatric History
1) Referral And Informants
• Patient’s details.
• When and where is patient being seen?
• Legal status of admission: voluntary or detained.
• Why are they being seen?
• Who was history taken from; patient or carer?
2) Introduction
• Who I am, my purpose and how long I have to interview the patient.
• Consent confidentiality, permission to take notes.
• Demographics, name, date of birth, occupation, marital status.
3) Presenting Complaint
What is the complaint(s), is this all of them?
‘If we could sort out all of these would things be all right?’
4) History of Presenting Complaint
• When did you last feel well?
• SOCRATES! The mnemonic for taking a history of a pain may be helpful for
some symptoms: Site, Onset, Character, Radiation, Alleviating factors , Time
course and periodicity, Exacerbating and precipitating factors, Severity
• When/ how did problems start? Can you think of any potential triggers?
Duration, course of the problem.
• These questions then vary depending on the specific problem that the patient
has presented with;
• DEPRESSION (treat feelings of low mood in the same way you would treat
pain, find out everything about the depression before moving on to ask about
other features/ associated symptoms).
How has mood been? How long has mood been long for, is mood always low,
when is it at its worst? Can you do anything to lift your mood? Do you ever
look forward to anything? Are you ever tearful?
Do you ever feel guilty, worthless or hopeless? Do you ever self harm? Have
you ever thought of ending it all?
Associated symptom; Is patient experiencing other physical symptoms? Is
appetite reduced, any weight loss, lack of motivation, sleep effected (trouble
getting to sleep, sign of mild depression, or early waking a sign of more
severe depression). Do you suffer from any other physical symptoms aches
and pains etc, has sex drive been effected? Have these symptoms caused
you any problems at work or at home?
• PSYCHOSIS
May be difficult to work out what symptoms patient is experiencing as they
are unlikely to tell you they are suffering from delusions etc.
• Have you been had any thoughts recently that you now accept as being
strange or that others have commented on being strange?
• Are there any plots against you?
Taking a Psychiatric History: Notes by Jason Hancock
www.askdoctorclarke.com 2
• Have people been interfering with your thoughts (thought insertion) or are
your thoughts being withdrawn or broadcast? (Thought alienation).
• Do you ever see or hear things that other people seem unable to see or hear?
(Hallucinations). If yes, are the voices talking about you (third person) or to
you (second person), are they commenting on what you are doing (running
commentary) or are they telling you to do certain things, if so what?
• Do you believe the voices and do you do what they tell you to do?
• Does the patient have any insight?
• Try to get an idea of how long these problems have been going on and how
they have changed over time.
• ANXIETY
Generalised anxiety; general feelings of anxiousness, feeling on edge, worry,
irritable, unable to relax.
Panic attacks; hyperventilation, SOB, chest pain/ palpitations, sweating,
tremor, how long do attacks last, what brings them on.
Phobias; any fears that you or others may consider to be irrational, any
thoughts you would consider obsessive.
Important to ask for all
• What does patient think the cause is?
• Any recent events that have precipitated the presenting complaint that the
patient feels may have had an effect. These events may be negative
(separation, death in family) or can be positive (promotion at work, increased
stress).
• Timing, did this event occur before or after the presenting complaint?
• What are the patients coping strategies?
5) Present Social Situation And Effect That The Illness Is Having
Effect that the condition is having on lifestyle: mainly work, family and friends.
• Who does patient live with?
• Who cares for them?
• SOCIAL SUPPORT, Do they have anybody they can confide in?
• Remember that some close family members can have a negative effect if they
show high expressed emotion (especially causing relapses of schizophrenia).
• What is patient’s normal level of functioning, how do they cope with activities
of daily living (ADL)?
• Does patient receive/ require any additional support?
• Does patient have any financial, employment or legal problems?
6) Previous history: psychiatric and general medical
(i) All PMH, Tell me about your birth, were you ever told you had any problems at
birth or during childhood? Has patient ever suffered a head injury, meningitis or from
epilepsy?
(ii) Past psychiatric history, past contact with psychiatric or mental health services,
dates, diagnosis, treatment, duration, legal status of admissions, history of self-harm
or suicide attempts. What has triggered problems in the past?

Taking a Psychiatric History: Notes by Jason Hancock
www.askdoctorclarke.com 3
7) Drug History
All current medications, prescribed, over the counter and street drugs.
Treatments that have been already tried/ used in the past, did they work, if not why
not?
Does patient have any problems with medications, do medications have any side
effects, does patient find it easy to comply with treatment, what are patients thoughts
towards treatments e.g. do they feel they need medication?
8) Family Medical And Psychiatric History
Is there a family history of neurological or psychiatirc disorders, suicides, criminal
behaviour or alcoholism?
For Asian patients it is important to ask about a family history of ‘possession’. For
afrocarabean patients it is important to ask about a family history of ‘witchcraft’.
9) Personal History
• How did patient find their childhood? Did patient get on well with siblings? Did
patient enjoy their childhood? Does patient remember being separated from
their parents for a period of time?
• What was patient’s relationship with their family like in the past is there a
history of abuse; ‘were you ever touched as a child in a way that made you
feel uncomfortable?’
• Did patient enjoy school, did they find it easy to make friends, what were their
hobbies, what were their educational achievements, and did patient go onto
further education?
• Is patient able to read and write confidently? Are they able to manage their
own money?
• Occupational history, types of job, length at each, and reasons for leaving.
What does patient currently do for a living and how are patient’s relationships
with colleagues?
• If patient currently unemployed what do they fill their day with, any hopes for
future employment?
• Psychosexual development, loss of virginity, orientation, if appropriate.
• Personal relationships, length, reason for ending, marital status and history,
any children? Degree of support from partner, current or past problems with
sexual performance (if appropriate).
• What levels of stress has patient been exposed to in their life and how do
they feel they have coped?
• Reproductive
history
• If female, history of teenage pregnancy? Abortions? History of menstruation,
first period, any PMT or heavy periods? Attitudes to periods?
• Forensic
history
• Has patient ever been in trouble with the law?
10) Premorbid Personality
(Can be difficult for some patient to assess their own personality and so a witness
may help)
• Personality, Are you happy go lucky, tense, shy, greedy, insecure?
• Are you an anxious person? Evidence of obsessional traits, what is patient’s
predominant mood?
• Relationships with superiors, and peers.
• Hobbies and interests?

Taking a Psychiatric History: Notes by Jason Hancock
www.askdoctorclarke.com 4
11) Alcohol And Drug History
Alcohol use at present; how much does patient drink a week, types of alcohol as well
as quantity. In what situations does patient drink, alone, in pub with friends?
Remember CAGE;
• Have you ever felt you should cut down the amount you drink?
• Have you ever felt annoyed by somebody commenting on the amount you
drink?
• Have you ever felt guilty about the amount you drink?
• Have you ever had an eye opener, a drink first thing in the morning to get
you going?
Alcohol use in the past; what has been the patient’s maximum regular usage?
Any use of illicit drugs in the past or substance misuse?
*Remember that a full psychiatric assessment requires a full history and a full mental
state examination. Although some of the questions may overlap generally the history
aims to find out what has been going on recently (leading up to this point), while the
mental state examination aims to assess the patients mood, thoughts etc at the time
of assessment.
Mental State Examination
¾
APPERANCE AND BEHAVIOUR
• Self care (reduced with dementia and depression).
• Eye contact, (reduced in depression, staring with Parkinsonism and
following use of some drugs).
• Face, pupils dilated and horizontal creases on forehead = anxiety,
corners of mouth turned down vertical lines on forehead =
depression.
• Agitation, can appear as either – i) Excessive motor activity with
depression or anxiety, ii) high level of activity with no anxiety i.e.
mania.
• Psychomotor retardation, posture slumped, slowing down of thought
and a reduction of physical movements, often seen in clinical
depression and can be accompanied by psychosis.
• Abnormal movements can have many causes:
¾
Tardive dyskinesias, involuntary movements of the face and
neck, may follow use of antipsychotics.
¾
Tremors.
¾
Stupor.
¾
Waxy flexibility – patients stays in any position that they are
placed in, e.g. schizophrenia or structural brain disorder.
¾
Forced grasping, takes examiners hand whenever offered,
dementia or chronic schizophrenia.
¾
Stereotypies uniform, repetitive non goal directed actions,
found in schizophrenia.
¾
SPEECH,
Æ
Form (rate), Æ Content,
• FORM, rate and flow; 1) If increased may indicate anxiety or a thought
disorder, if goal directed this is pressure of speech - thoughts jump
from one thought to another with a connection between thoughts then
think mania, if no connection between thoughts this indicates
Taking a Psychiatric History: Notes by Jason Hancock
www.askdoctorclarke.com 5
schizophrenia. 2) Decreased, may indicated psychomotor retardation,
mutism maybe present with schizophrenia or severe depression. 3)
Incoherent? 4) Perseveration, repeating same words or phrases
mainly seen in dementia.
• CONTENT, is speech appropriate, is speech congruent? Neologisms:
words created by schizophrenic patients to describe morbid
experiences, Echolalia (repeating same words phrases as examiner),
echopraxia (repeating movements of examiner), are both common in
schizophrenia.
¾
MOOD
• Subjective (how patient tells you it is) and objective, how it looks to
you that they are.
• DEPRESSION
• Do you feel your mood is low? Feeling tearful? Can you do anything to
cheer yourself up?
• Have they ever felt guilty about the past, pessimistic about the present
or hopeless about the future?
• ‘It must be difficult feeling so worthless and hopeless about the future,
have you ever thought of ending it all?’
• ANXIETY, how do you feel when you get anxious? Any palpitations,
dry mouth, sweating, trembling.
• MANIA, how are your spirits, unusually good?
• Objective
• Do emotions appear appropriate; is range of emotions restricted as
may be the case with depression or schizophrenia, are emotions
incongruent as may be the case with mania,
• Do emotions appear to be labile (excessively changing)?
¾
THOUGHTS
• Delusions; Have you noticed that you have been having any odd
thoughts? Or thoughts that others have found strange?
¾
Primary delusions, thought alienation, persecutory delusions in
schizophrenia.
¾
Nihilistic, hypochondrical, worthless, guilt, hopelessness in
depression.
¾
Grandiose delusions in mania.
• Thought disorders; Do you find it hard to concentrate/ notice that your
thoughts fly from place to place.
• Any thought block?
• Obsessional phenomena; do thoughts keep entering your head even
though you try hard to stop them? Ask about compulsive rituals.
• Thought alienation, schizophrenia; Are your thoughts being interfered
with, are people putting thoughts into your head or listening to your
thoughts, is anybody harming you or plotting to harm you?
• Depersonalisation; do you feel unreal or that any part of your body is
unreal?
• Derealisation; do you feel ever that things around you are unreal?
Depersonalisation and derealisation can occur in anxiety disorders.
Taking a Psychiatric History: Notes by Jason Hancock
www.askdoctorclarke.com 6
5) PERCEPTION
• Can you see or hear things others can not?
• Does sense come from within or is it external e.g. can you hear voice
in the same way you can hear me now?
• Have you ever seen something and thought that it was something
else? (Illusions).
• Auditory hallucination, 3
rd
person, is there only one voice or are there
more? commentary schizophrenia, 2
nd
person abusing them.
• Visual hallucinations, think organic brain disease.
• Depersonalisation or derealisation can occur with anxiety or fatigue.
6) COGNITIVE FUNCTION
• Best to perform a full mini mental state examination however
Hodgkinsons abbreviated mental test score is quicker.
• Score out of ten, serial scores are better than one off values;
¾
Present year and your age (2)
¾
Time to nearest hour (1)
¾
Recognition of people (1)
¾
Name of place (1)
¾
Birthday
(1)
¾
Name of prime minister (1)
¾
Memorise address (1)
¾
Date of second world war (1)
¾
Count backwards from 20 Æ 1 (1)
• Other useful questions; abstract thought, can patient understand how
a phrase like ‘a rolling stone gathers no moss’ could relate to humans,
(if not think schizophrenia).
7) INSIGHT
i.
Abnormal experiences are extraordinary.
ii.
That they are a result of the disease process.
iii.
That they can be prevented by medical treatment.
iv.
CRUCIALLY, must assess if patient is a risk to themselves or
others.
Full mini mental state examination
Orientation;
What is the (year) (season) (date) (day) (month)? [5]
Where are we: (country) (county) (town/city) (building) (floor)?
[5]
Registration
Name 3 common objects (apple, table, penny) take 1 second to say each word.
Ensure patient has understood; ask them to repeat three words.
Give 1 point for each correct answer. Record how many trials it takes for patient to
understand all three words. [3]
Attention
Spell WORLD backwards. The score is the number of letters in the correct order. [5]
Taking a Psychiatric History: Notes by Jason Hancock
www.askdoctorclarke.com 7
Recall
Ask for the 3 objects named above. Give 1 point for each correct answer. [3]
Language
Point to a ‘pencil’ and ‘watch’ ask patient to name. [2]
Repeat: ‘No ifs ands or buts’.
[1]
Follow a three stage command: ‘Take a piece of paper in your right hand, fold it in
half and place it on the floor’. (Do not gesture to the patient at all while doing this,
they must follow auditory commands)
[3]
Read and obey the following:
[1]
Close your eyes
Write a sentence.
[1]
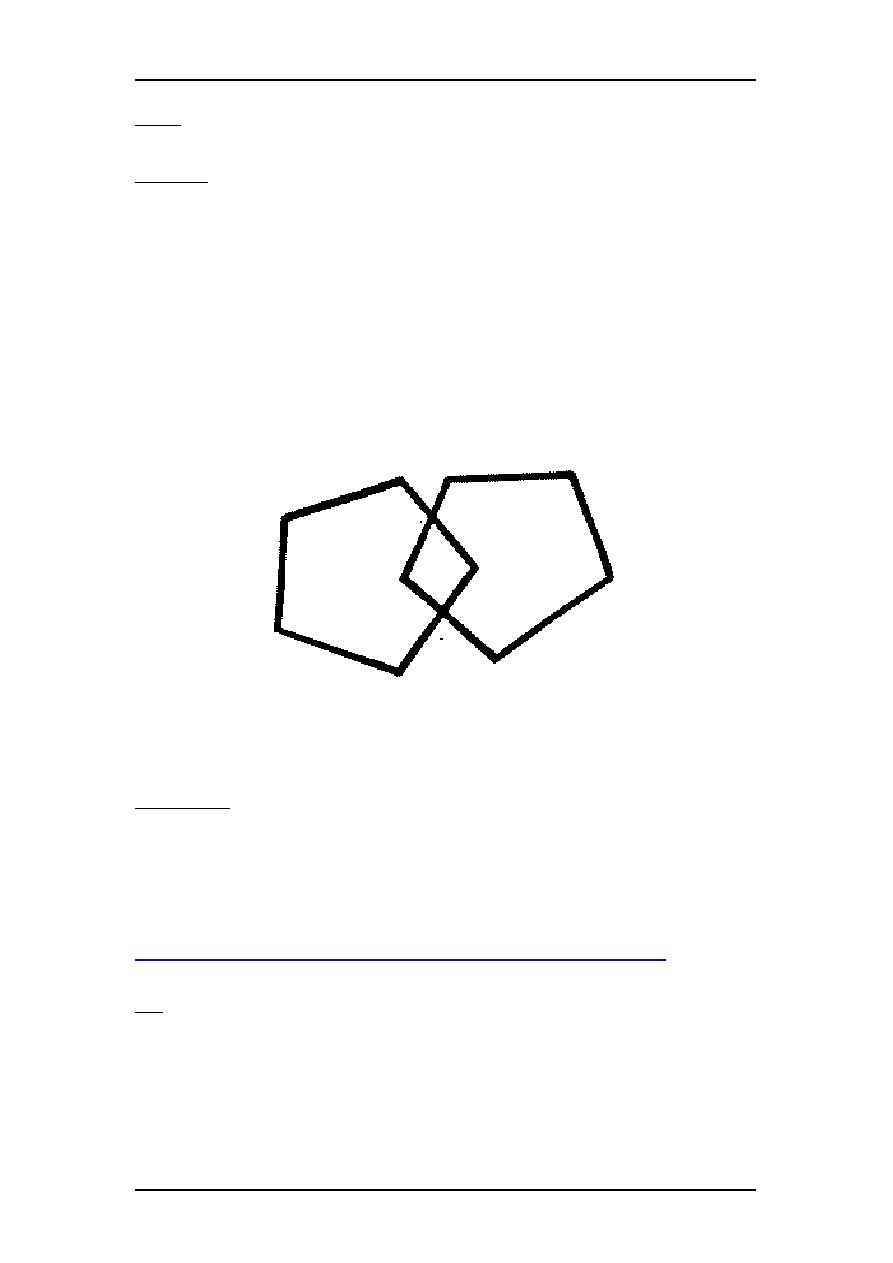
Copy the following design;
[1]
Full score out of 30.
Bibliography;
Chapter 4, ‘Psychiatry’, ‘Oxford handbook of clinical specialties’, seventh edition,
New York, oxford university press, 2006,
Chapter 4, ‘Anxiety disorders’, ‘Master medicine, psychiatry’, first edition, London,
Churchill Livingstone, 2002,
Design for MMSE taken from;
http://app1.unmc.edu/geriatricsed/delirium/mini_mental_satus_exam.htm
Accessed
on the 11/11/07
Note
These notes were written by Jason Hancock as a medical student in 2008. They are presented in good
faith and every effort has been taken to ensure their accuracy. Nevertheless, medical practice changes
over time and it is always important to check the information with your clinical teachers and with other
reliable sources. Disclaimer: no responsibility can be taken by either the author or publisher for any loss,
damage or injury occasioned to any person acting or refraining from action as a result of this information