
1
Prolonged labour ( Dystocia)
Dr Ban Hadi
F.I.C.O.G. 2015
Abnormal labour
Labour becomes abnormal when there is:
1. Poor progress (as evidenced by a delay in cervical dilatation or
descent of the presenting part)
2. The fetus shows signs of compromise.
3. There is a fetal malpresentation
4. A multiple gestation
5. A uterine scar
6. Labour has been induced
Risk factors for abnormal labour
Small woman
•
Big baby
•
Dysfunctional uterine activity
•
Malpresentation
•
Malposition
•
Early membrane rupture
•
Soft-tissue/pelvic malformation
Progress in labour is dependent on three variables:
1.
The power, i.e. the efficiency of uterine contractions
2.
The passenger (fetal size, presentation and position)
3.
The passages (the uterus, cervix and bony pelvis).
Poor progress in labour:
Poor progress in the first stage of labour
Poor progress in labour has been defined as cervical dilatation of less
than 2 cm in 4 hours, usually associated with failure of descent and
rotation of the fetal head.
Poor progress in the second stage of labour:
Delay in 2
nd
stage is diagnosed if delivery is not imminent after 2 hours
in a nulliparous woman and 1 hour for a parous woman. With epidural
use the birth of the baby is expected to take place within 3 hours of the

2
start of the second stage in nulliparous woman, and 2 hours in parous
woman.
Causes of poor progress in labour
:
Abnormalities can be classified as abnormalities of the power, the
passenger and the passages
A.Dysfunctional uterine activity
This is the most common cause of poor progress in labour. It is more
common in primigravidae and perhaps in older women and is
characterized by weak and infrequent contractions which can be
exacerbated by epidural use.
How would you assess uterine activity?
1. By clinical examination: palpate the uterine fundus and measure the
duration of contraction and its interval
2. By using external uterine tocography. However, this can only provide
information about the frequency and duration of contractions.
3. Intrauterine pressure catheters are available and these do give a more
accurate measurement of the pressure being generated by the
contractions, but they are rarely necessary.
Efficient uterine contractions: when the frequency is four to five
contractions per 10 minutes and each lasts for 40-50 seconds. Fewer
contractions than this does not necessarily mean progress will be slow,
but more frequent examinations may be indicated to detect poor progress
earlier.
B
.Abnormal fetal size, presentation and position
Such as fetal macrosomia, conjoined twin, brow presentation and occiput
posterior position.
Malpresentation
:
defined as anything other than a vertex, as it is vital to
good progress in labour is the tight application of the fetal presenting part
on to the cervix in normal vertex presentation.
Presentations that can be delivered vaginally at term are: vertex, face
(mento-ant.) and breech.
Presentations that are not deliverable vaginally at term are: face (mento-
post., brow and shoulder.
Face presentations may apply themselves poorly to the cervix and the
resulting progress in labour may be poor, although vaginal birth is still

3
possible. Brow presentations are associated with the mento-vertical
diameter, which is simply too large to fit through the bony pelvis unless
flexion occurs or hyperextension to a face presentation. Brow
presentation therefore often manifests as poor progress in first stage,
often in a multiparous woman. Shoulder presentations cannot deliver
vaginally and once again poor progress will occur. Malpresentations are
more common in women of high parity because of uterine laxity and
some carry a risk of uterine rupture if the labour is allowed to continue.
Malposition: normal position is occiput ant., malposition is occiput post.
and occiput transverse
C.Abnormalities of the birth canal (the ‘passages’)
The bony pelvis may cause delay in the progress of labour as in android
pelvis. Abnormalities of the uterus and cervix can also delay labour.
Unsuspected fibroids in the lower uterine segment can prevent descent of
the fetal head. Delay can also be caused by ‘cervical dystocia’, a term
used to describe a non-compliant cervix which effaces but fails to dilate
because of severe scarring, usually as a result of a previous cone biopsy.
Caesarean section may be necessary. It is rare for the soft tissues of the
pelvic floor to cause significant delay in labour.
Cephalopelvic disproportion:
Cephalopelvic disproportion (CPD) implies anatomical disproportion
between the fetal head and maternal pelvis.
Causes of CPD: It can be due to
1. A large head
2. A small pelvis
3. A combination of the two. Women of small stature with a large
baby in their first pregnancy are likely candidates to develop this
problem.
4. The pelvis may be unusually small because of previous fracture
or metabolic bone disease.
5. Rarely, a fetal anomaly will contribute to CPD. Obstructive
hydrocephalus may cause macrocephaly, and fetal thyroid and neck
tumours may cause extension at the fetal neck.
6. Relative CPD is more common and occurs with malposition
of the fetal head. The occipito-posterior position is associated
with deflexion of the fetal head and presents a larger skull
diameter to the maternal pelvis
Diagnosis of Cephalopelvic disproportion is suspected in labour if:
1
progress is slow or actually arrests despite efficient uterine contractions
2
the fetal head is not engaged

4
3
vaginal examination shows severe moulding and caput formation
4
the head is poorly applied to the cervix.
Management of prolonged labour
:
A. Diagnosis:
Partograph will diagnose long labour before obstructed labour develops,
so history should include:
- Age, parity
- Duration of labour, partograph abnormalities, duration of ruptured
membranes (amount and colour of liquore)
- Duration of bearing down
- Antenatal records and complications
- Previous prolonged labour, fetal death, instrumental delivery and
caesarean sections
Examination:
- General exam. Features of maternal distress: exhaustion, ketosis,
dehydration, tachycardia, fever and scanty urine.
- Abdominal exam.
Frequency and intensity of uterine contractions
Presentation, engagement, estimated fetal weight
The retraction ring (bandl's ring) is seen in obstructed labour and felt
between the tonically contracted upper segment of the uterus and the
distended, tender and stretched lower segment, it is the site of uterine
rupture.
- fetal heart auscultation for possible fetal compromise
- Vaginal exam. dry hot vagina, cervical dilatation, fetal presentation
and position, station, excessive caput and moulding indicates CPD.
5
B. Treatment
:
Treatment of poor progress in the 1
st
stage of labour:
1. Good hydration, adequate pain relief, empty bladder, cross match
blood and emotional support.
2. When poor progress in labour is suspected it is usual to recommend
repeat vaginal examination 2, rather than 4, hours after the last exam. and
plot on partograph.
3. If delay is confirmed, the woman should be offered artificial rupture of
membranes (ARM) and, if there is still poor progress in a further 2 hours;
use an oxytocin infusion to augment the contractions. The infusion is
commenced at a slow rate initially, and increased carefully every 30
minutes. Continuous EFM is necessary as excessively frequent and
augmented contractions may cause fetal compromise.
4. Women can be offered an epidural anaesthesia
5. If progress fails to occur despite 4–6 hours of augmentation with
oxytocin, a Caesarean section will usually be recommended
6. Active management of third stage of labour because of risk of PPH
Treatment of poor progress in the 2nd stage of labour:
1. Rehydration and intravenous oxytocin for inefficient uterine cont.
2. Instrumental birth can be considered for prolonged second stage
3. Caesarean delivery if the instrumental birth attempt is unsuccessful,
or if elements of obstructed labour present
Treatment of CPD:
1. Oxytocin can be given carefully to a primigravida with mild to
moderate CPD as long as the cardiotocography is reactive. Relative
disproportion may be overcomed if the malposition is corrected (i.e.
conversion to a flexed OA position).
2. Oxytocin must never be used in a multiparous woman where CPD is
suspected
3. A Caesarean section is indicated in cases of CPD with elements of
obstructed labour
Note: Extreme caution must be exercised when you augment labour in a
multiparous woman as excessive uterine contractions in a truly obstructed
labour may result in uterine rupture which is extremely rare in
primiparous women. Augmentation with oxytocin is contraindicated if
there are concerns regarding the condition of the fetus or previous uterine
scar.
6
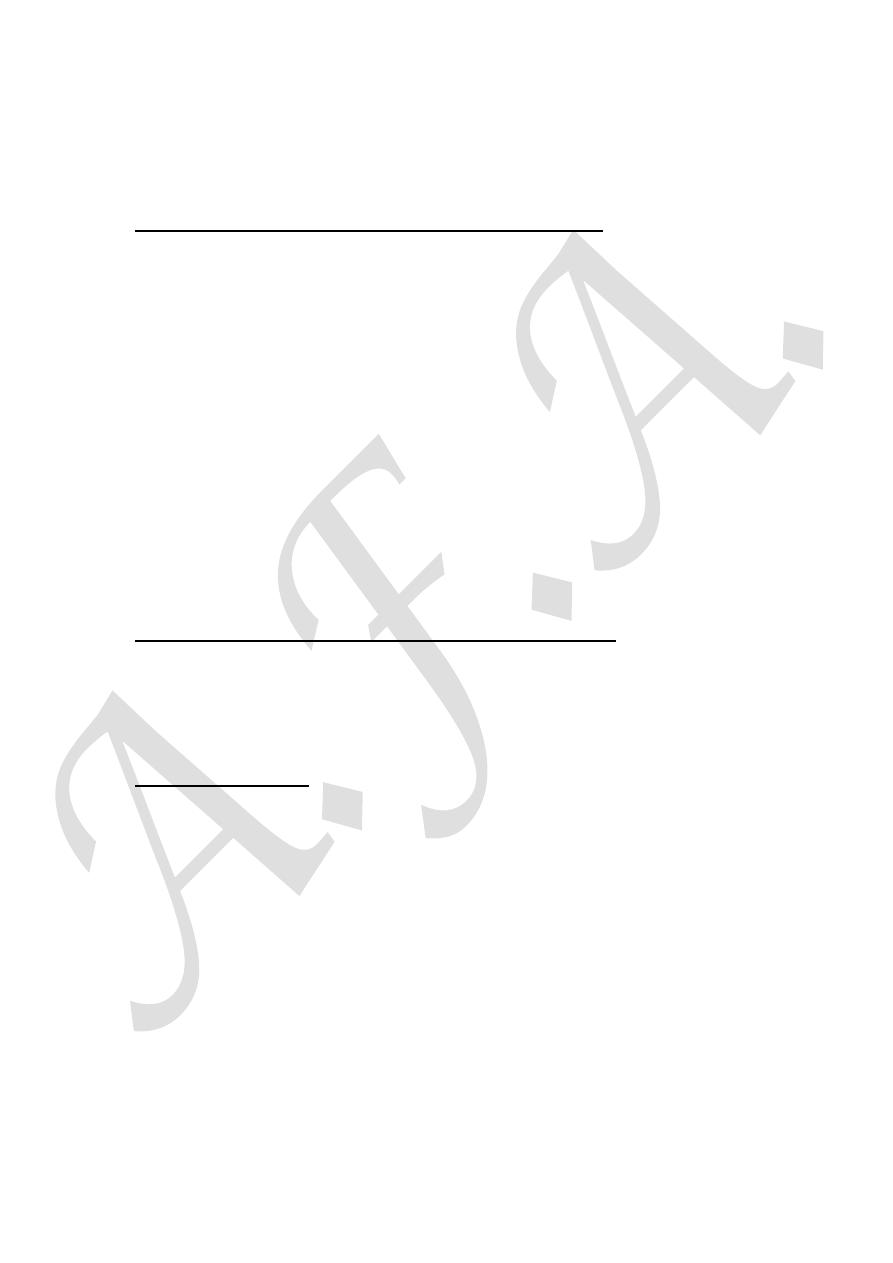
Patterns of abnormal progress in labour:
The use of a partogram to plot the progress of labour improves the
detection of poor progress. The main aim of partograph is the early
diagnosis of prolonged labour before the complicatins of obstructed
labour develop.
Normal labour progress should be at or to the left of the alert line of
partograph as shown below:
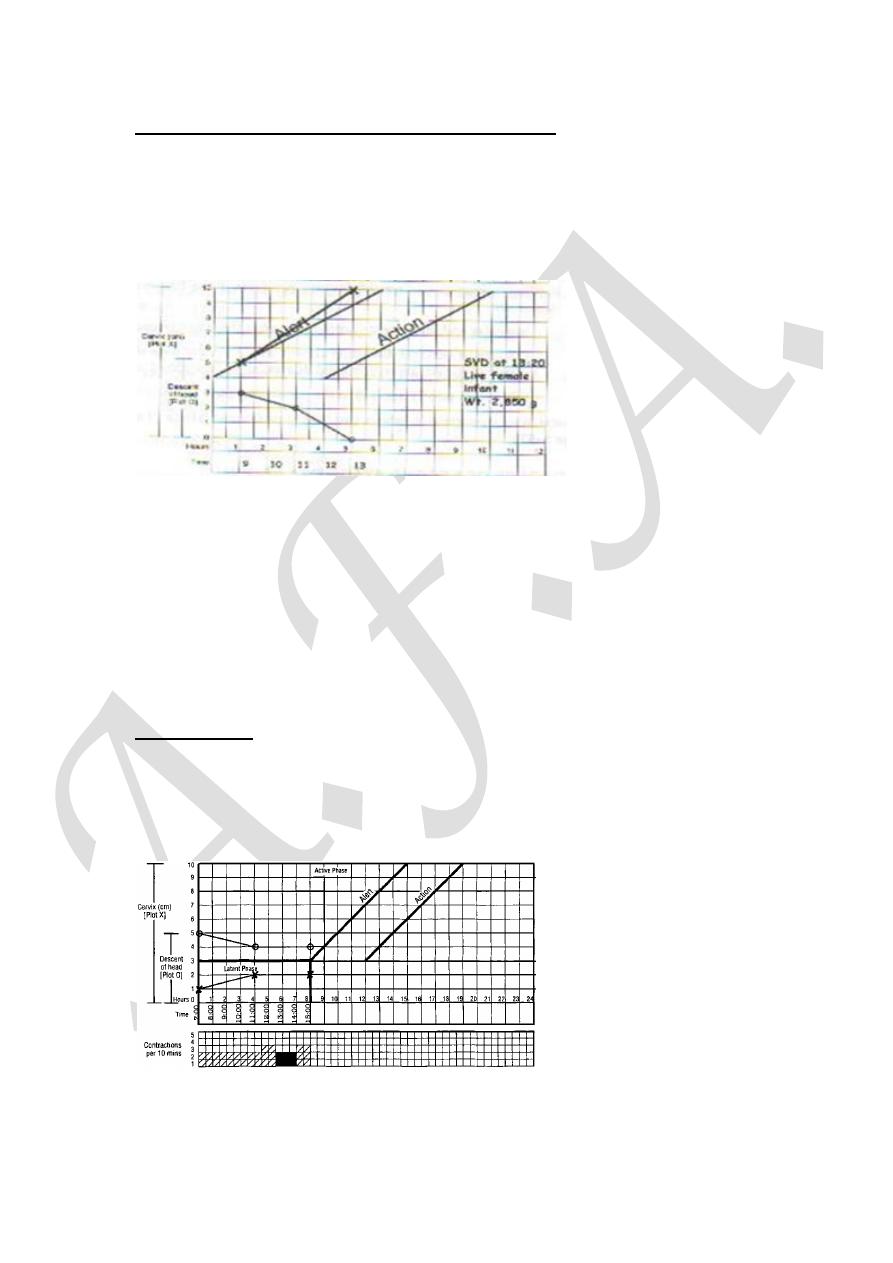
Patterns of abnormal labour are:
1. Prolonged latent phase occurs when the latent phase is longer than the
normal time limits (20 hrs in nulliparous and 14 hrs in multiparous
women). It is more common in primiparous women and probably results
from a delay in the chemical processes that occur within the cervix which
soften it and allow effacement. Prolonged latent phase can be extremely
frustrating and tiring for the woman.
Management: It is best managed away from the labour suite with simple
analgesics, mobilization and reassurance.
However, intervention in the form of ARM or oxytocin infusion will
increase the likelihood of poor progress later in the labour and the need
for Caesarean birth.
7
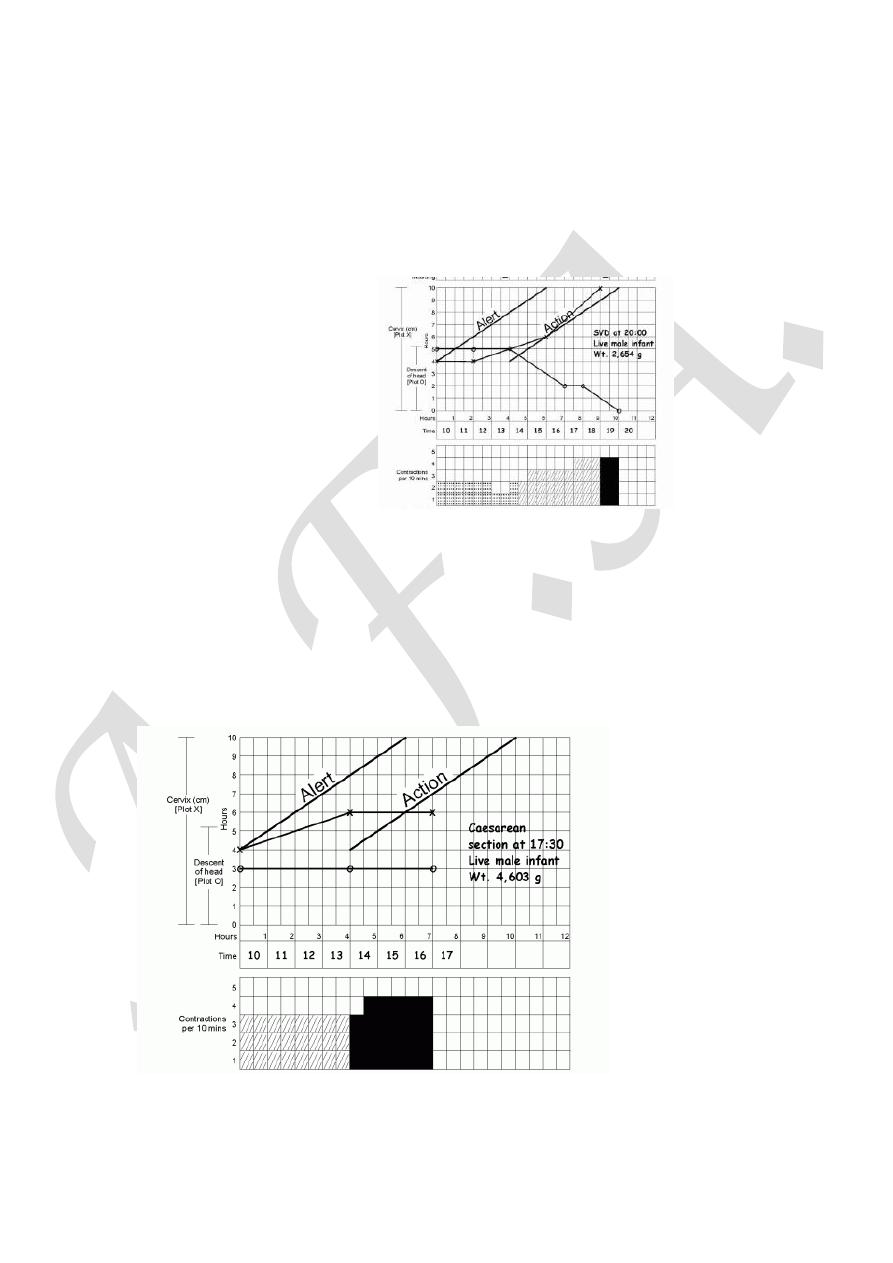
2. Primary dysfunctional labour: is the term used to describe poor
progress in the active phase of labour ( <2 cm cervical dilatation/4 hours)
and is also more common in primiparous women. It is most commonly
caused by inefficient uterine contractions, but can also result from CPD
and malposition of the fetus.
3. Secondary arrest of cervical dilatation: occurs when progress in the
active phase of first stage is initially good but then slows, or stops
altogether, typically after 7 cm dilatation. Although inefficient uterine
contractions may be the cause, fetal malpositions, malpresentations and
CPD are more common than in primary dysfunctional labour
8
4.Arrest of descent of presenting part: when the descent of the
presenting part stops as assessed by abdominal and vaginal examination,
fetal malpositions, malpresentations and CPD are possible causes.
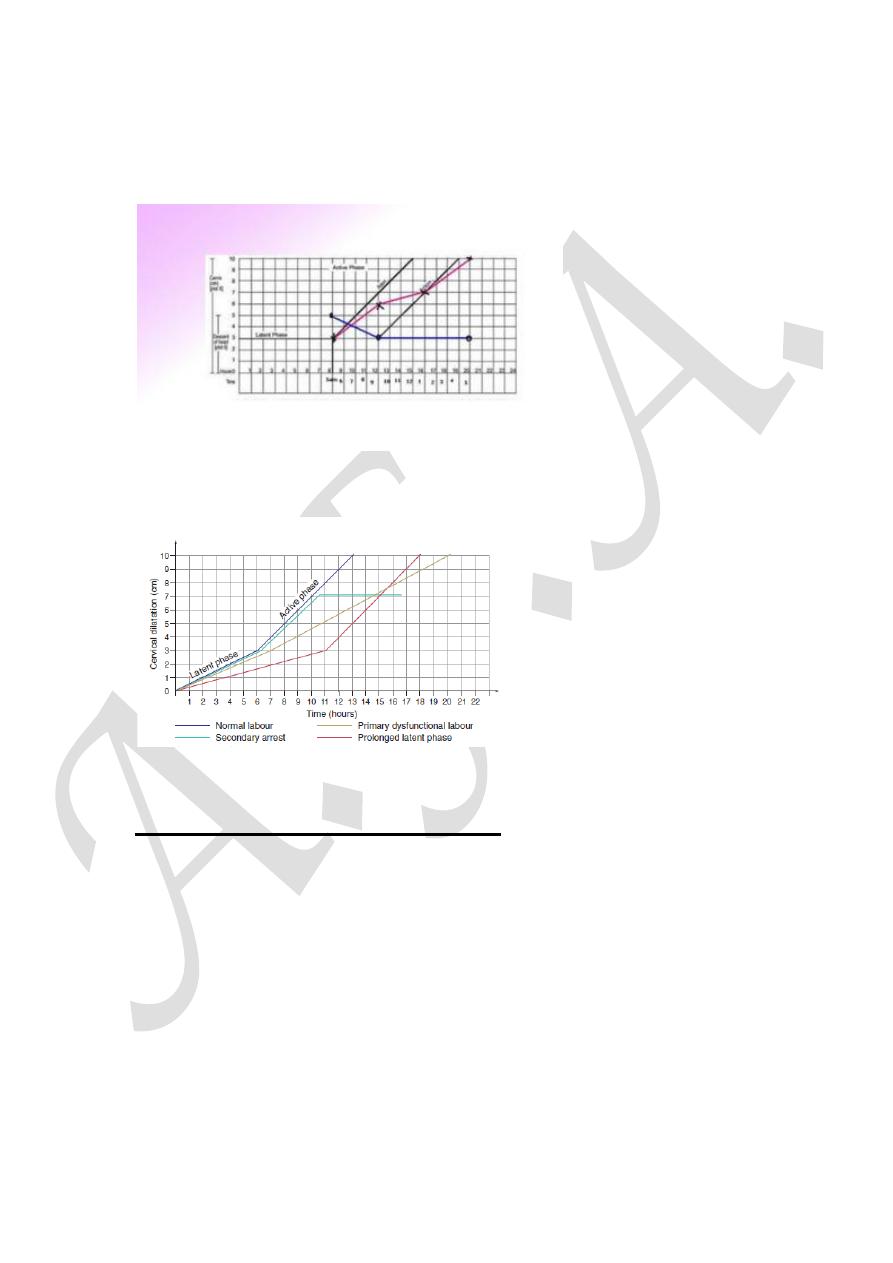
Abnormalities of the partogram
Complications of prolonged labour:
Maternal :maternal exhaustion and dehydration, rupture of uterus,
increased operative intervention, maternal injury, shock, postpartum
hemorrhage, puerperal sepsis and maternal death
Late maternal complications: urinary fistula and infertility
Fetal : birth asphyxia, acidosis, intracranial hemorrhage, meconium
aspiration, fetal trauma, death and neonatal infection
Late fetal complications: cerebral palsy and mental retardation
Thank you