1
Forth stage
Obstetric
Lec-X
د.ولدان
9/12/2015
NORMAL LABOUR
Labour:
Is the whole process whereby the products of conception are expelled from the mother
being naturally about term
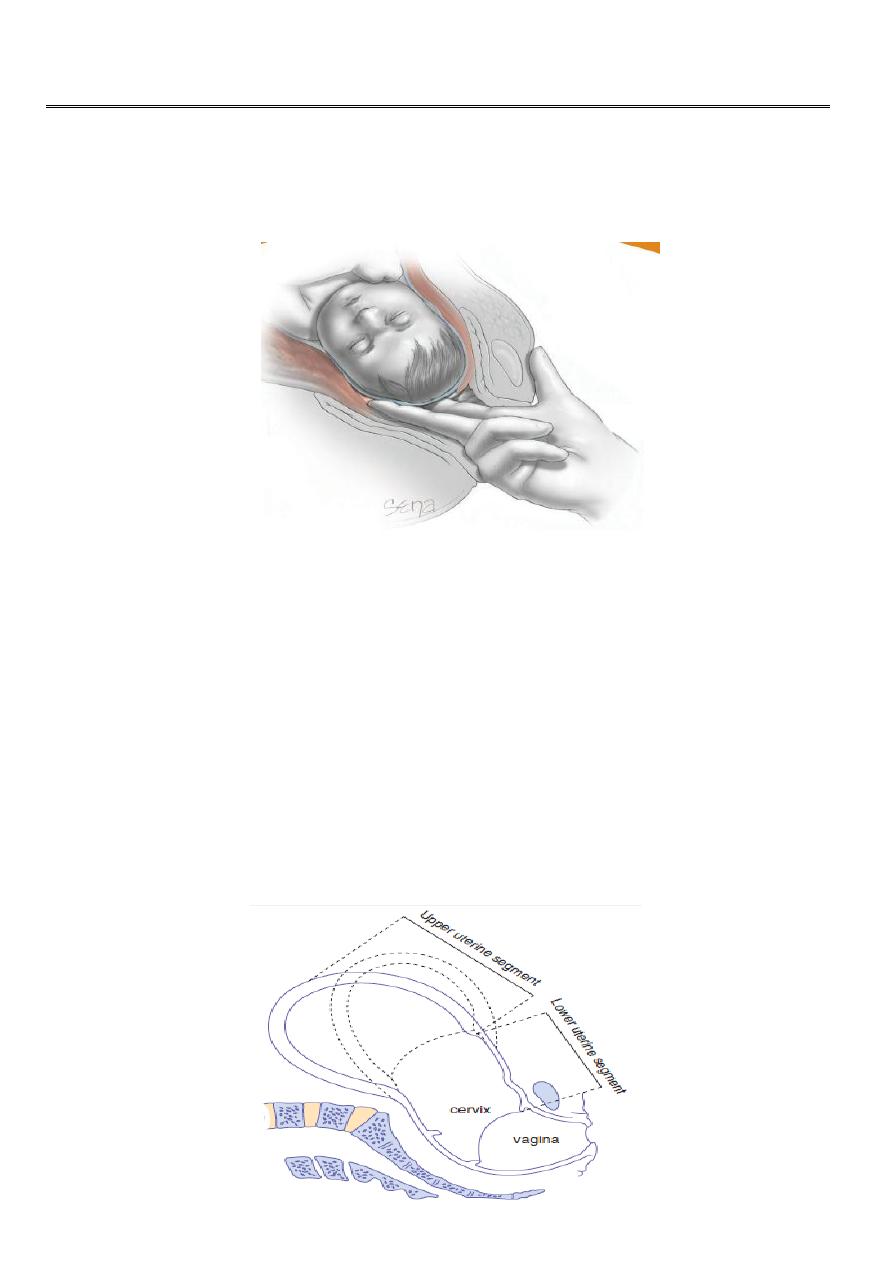
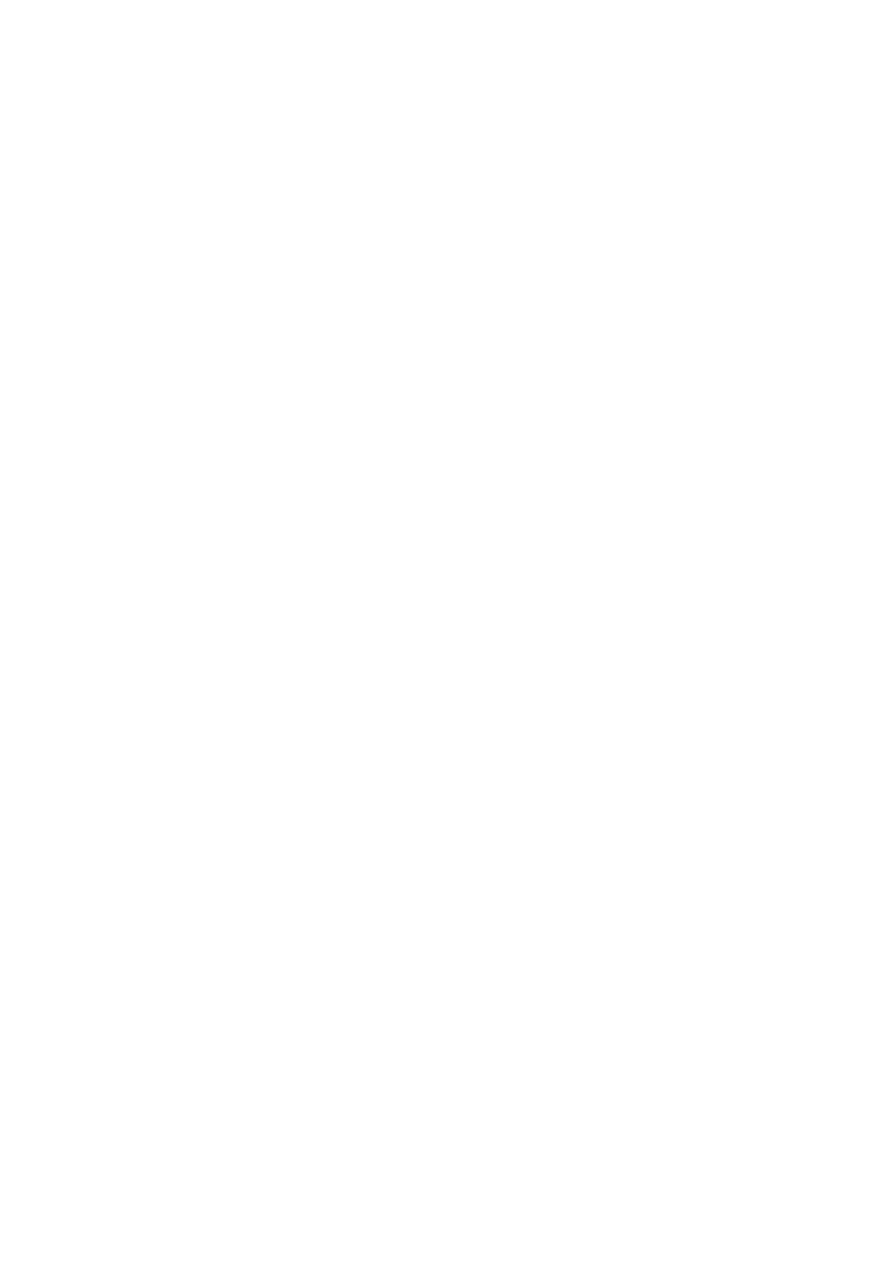
The uterus is divided into upper & lower segment that are fully formed at the end of first
stage of labour. With each contraction the upper part of uterus [upper segment] muscles
become shorter & thicker.
The [lower segment] consist of lower part of body of the uterus & cervix which become
thinner, taken up with contractions & then cervix dilated.

2
Symptoms & signs of the onset of labour
Painful uterine contractions.
The show.
Rupture of membranes.
Shortening & dilatation of cervix.
The contractions:
The uterus contracts irregularly & painlessly throughout pregnancy [Braxton hicks
contractions], labour is recognized by regular & painful contraction during which uterus is
felt harden with increase in duration, intensity & frequency. At end of first stage it may
come every two to three minutes & last 45 seconds to one minute.
The show:
This is mucous discharge from the cervix mixed with little blood as a result of taking up of
the internal os & separation of membranes.
Rupture of the membranes:
The membranes may rupture at any time during labour & usually occurs towards the end of
first stage of labour. Early rupture of membranes is more likely to occur if the presenting
part not engaged or there is malpresentation.
Shortening & dilatation of the cervix:
When labour begins the contraction & retraction of upper segment stretches the lower
segment & upper part of cervix so that the internal os is pulled open, the cervix is dilated
from above downwards becoming shorter until no projection into vagina is felt.
3
The stages of labour:
Labour is divided into three stages:
First stage
,
or stage of dilatation from onset of true labour until the cervix is fully dilated.
Second stage,
or stage of expulsion of fetus, from full dilatation of the cervix to delivery of
fetus or fetuses.
Third stage
,
from delivery of fetus until the placenta & membranes are delivered.
The first stage of labour:
The uterine contraction & dilatation of internal os cause separation of chorion from decidua
closest to it thus a small back of membranes is formed into the internal os, the head then
comes down separates liquor amnii which is above it from that in the back called
respectively the hind & fore waters. When membranes ruptured the fetal axis pressure
comes into play; the upper pole of fetus is pressed on by the fundus of the uterus. While
the lower pole is pressed down onto the lower segment & cervix.
Normal first stage should not exceed 12 hours in a primigravida & 8 hours in
multipara.
The character of pain is the same as spasmodic dysmenorrhoea caused by ischaemia
of uterine muscles from compression of blood vessels in the wall of the uterus.
The first stage of labour can be divided into two phases
The ‘latent phase’ is the time between the onset of labour and 3–4 cm dilatation. During
this time, the cervix becomes ‘fully effaced’.
Effacement is a process by which the cervix shortens in length as it becomes included into
the lower segment of the uterus. The effacement may begin during the weeks preceding
the onset of labour, but will be complete by the end of the latent phase.
The cervical os cannot usually begin to dilate until effacement is complete. Effacement and
dilatation should be thought of as consecutive events in the nulliparous woman, but may
occur simultaneously in the multiparous woman. The duration of the latent phase is
variable, usually lasts between 3 and 8 hours, being shorter in multiparous women.
The second phase of the first stage ‘active phase’ and describes the time between the
end of the latent phase (3–4 cm dilatation) and full dilatation (10 cm). It is also variable
in length, usually lasting between 2 and 6 hours. Again, it is usually shorter in
multiparous women. Cervical dilatation during the active phase usually occurs at 1
cm/hour or more in a normal labour but is only considered abnormal if it occurs at less
than 2 cm/hour.
4
The second stage of labour:
This describes the time from full dilatation of the cervix to delivery of the fetus or fetuses.
The second stage of labour may also be subdivided into two phases.
The passive phase: The time between full dilatation and the onset of involuntary
expulsive contractions. There is no maternal urge to push and the fetal head is still
relatively high in the pelvis.
The second phase is rather confusingly called the ‘active second stage’. There is a
maternal urge to push because the fetal head is low (often visible), causing a reflex need
to ‘bear down’.

5
In a normal labour, second stage is often diagnosed at this point because the maternal
urge to push prompts the midwife to perform a vaginal examination. Conventionally, a
normal active second stage should last no longer than 2 hours in a primiparous woman and
1 hour in those who have delivered vaginally before. Use of epidural anaesthesia may
influence the length and the management of the second stage of labour.
The presenting part is pushed down onto the pelvic floor; pelvic floor resistance has to be
overcome by uterine contractions, aided by the action of the voluntary muscles of the
abdominal wall & diaphragm. As contraction comes on patient takes a deep breath then
bears down with all the force of her abdominal muscles, during height of pain there may be
expiratory groans.
With each contraction the presenting part is forced down to pelvic floor, during intervals
between contraction at first slipped back, after this with contraction & expulsive effort the
head slowly moves down in a forward direction, when the widest diameter of the head
distends the vulva it is said to be crowned. Then the head passed through vulva followed by
the body in next contraction.
The duration of labour:
It is difficult to define prolonged labour, but it would be reasonable to suggest that labour
lasting longer than 12 hours in nulliparous women and 8 hours in multiparous women
should be regarded as prolonged.
The third stage of labour:
This is the time from delivery of the fetus or fetuses until delivery of the placenta(e). The
placenta is usually delivered within a few minutes of the birth of the baby. A third stage
lasting more than 30 minutes should be considered abnormal, unless the woman has opted
for ‘physiological management’ in which case it is reasonable to extend this definition to 60
minutes.
As the cavity of the uterus becomes smaller after delivery the placenta is shorn off the
spongy layer of decidua basalis, further uterine contractions expel the placenta from the
upper segment into the lower segment & vaginal vault this is called separation of placenta.
The placenta is expelled from vagina followed by membranes & any retroplacental blood
clot.

6
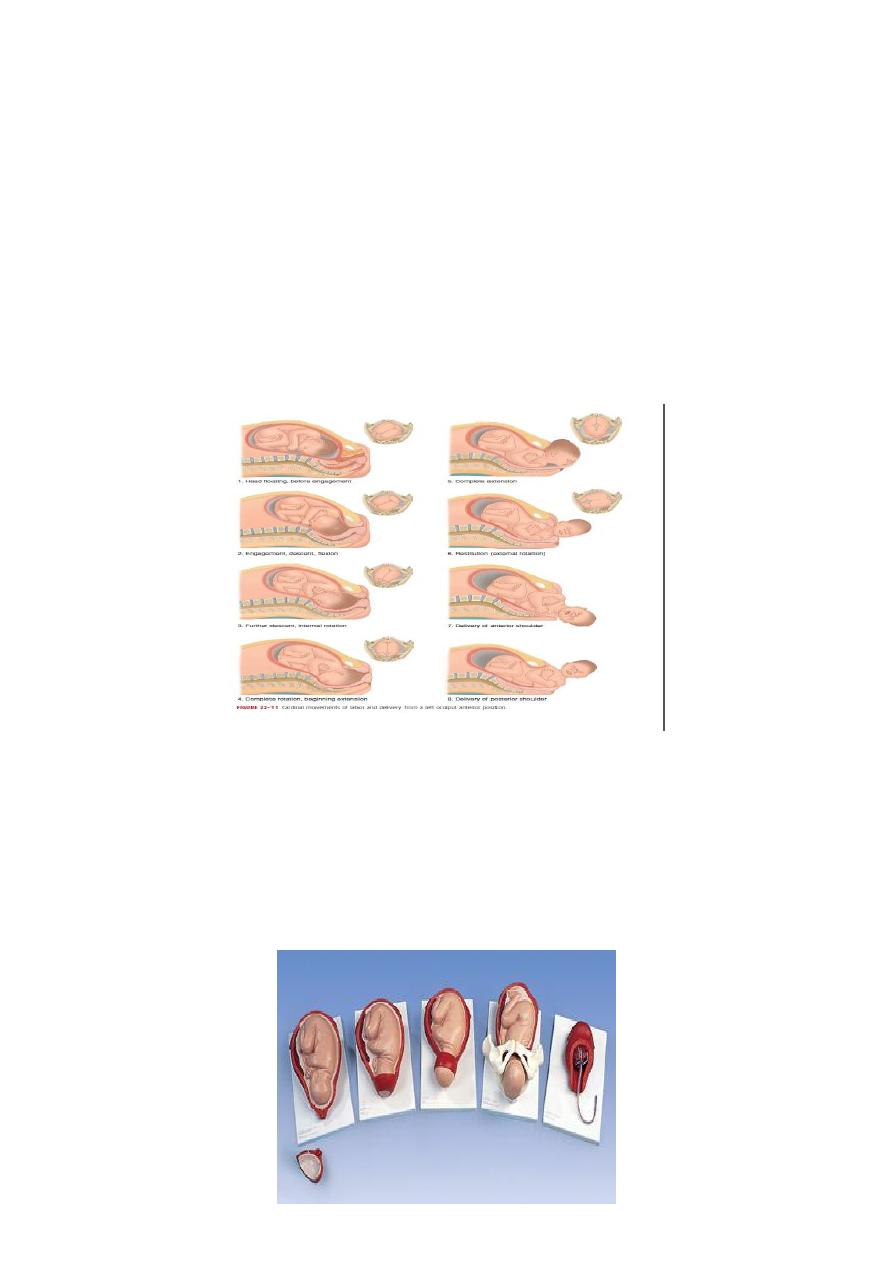
THE MECHANISM OF LABOUR
This is referred to series of changes in position & attitude which the fetus undergoes during
its passage through the birth canal.
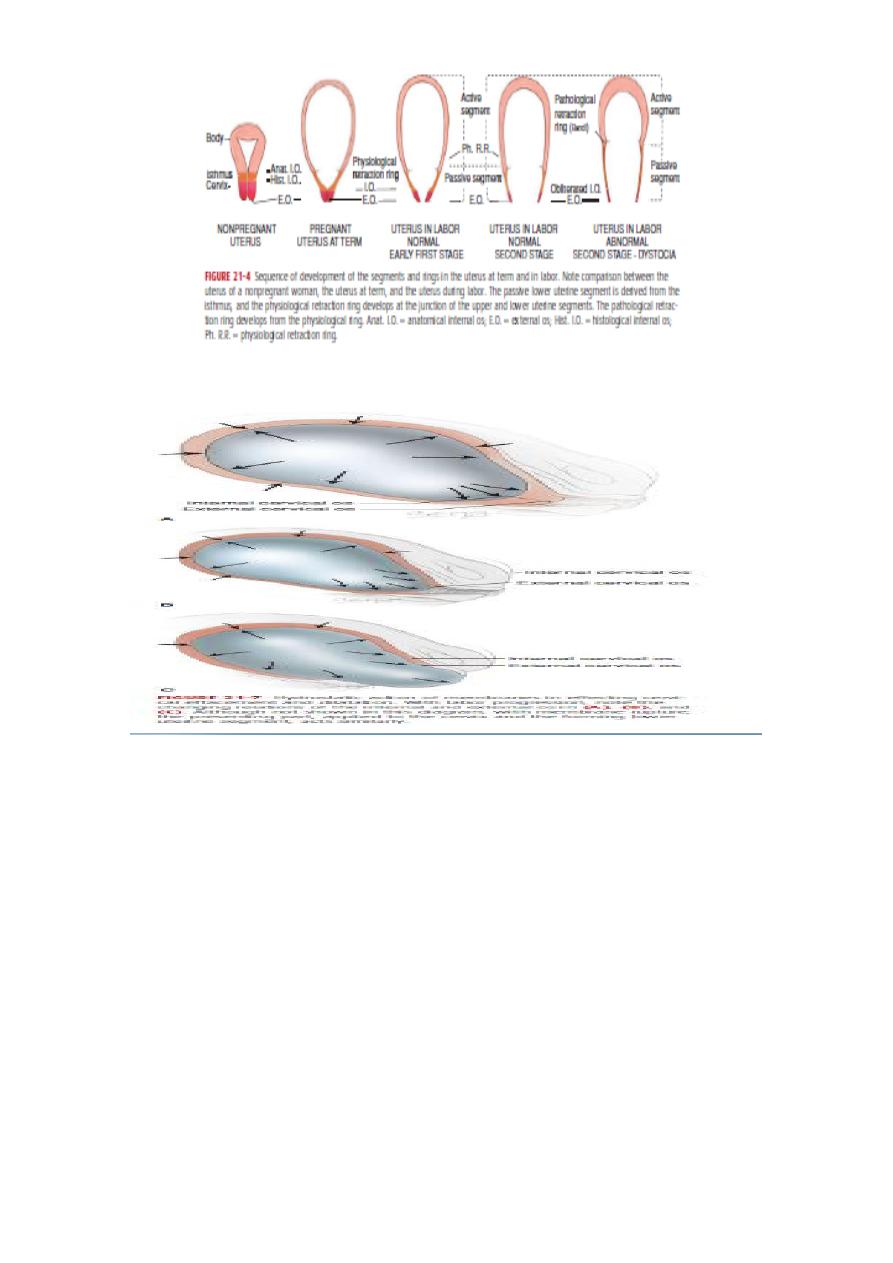
The following items are used to describe the position of fetus in relation to the uterus &
maternal pelvis;
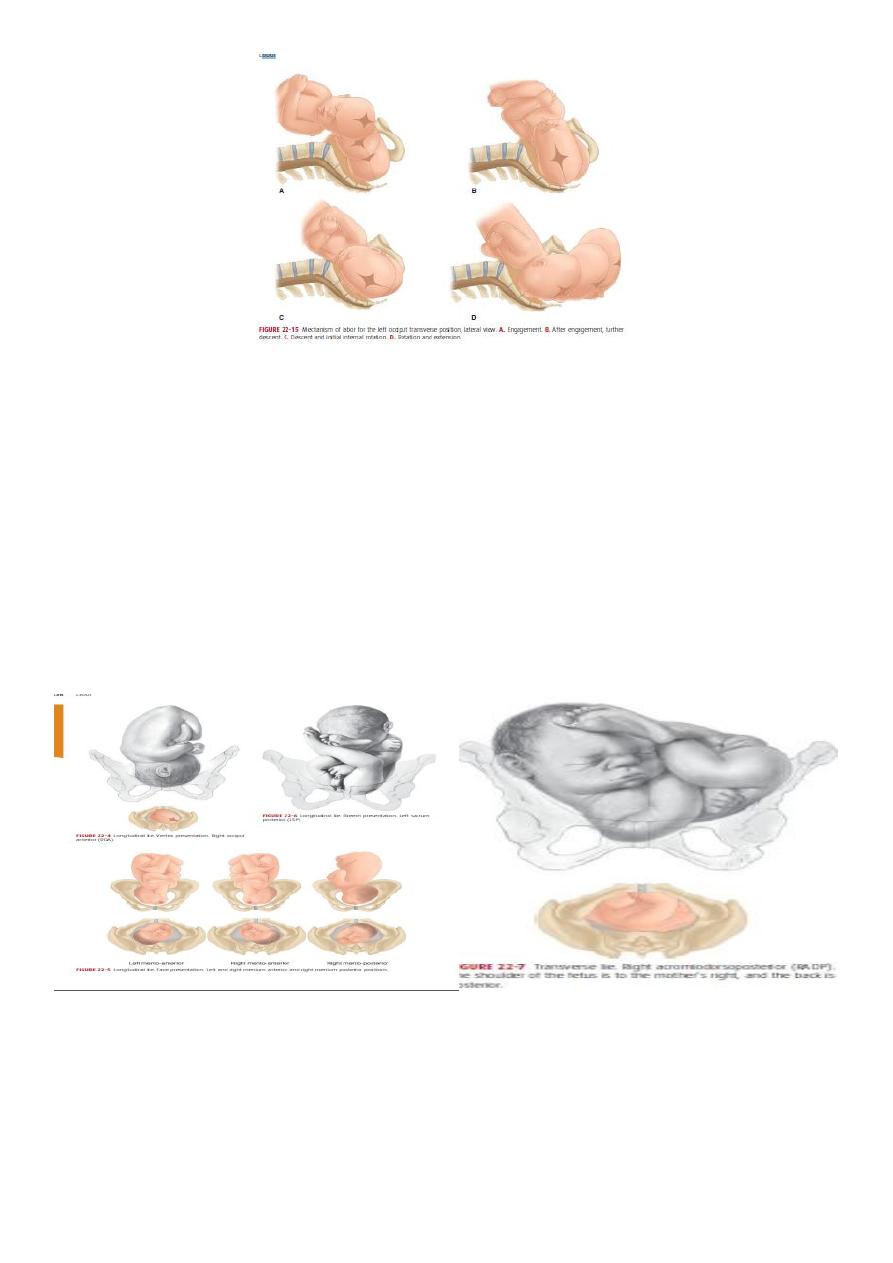
Lie
The relation of the long axis of the fetus to the uterus, this may be longitudinal, oblique or
transverse.
Presentation
Is that part of the fetus in or over the pelvic brim in relation to the cervix. If the head
occupies the lower segment the presentation is cephalic, if is flexed on the spine the vertex
presents.
If the head is fully extended this caused face presentation
if is partly extended cause brow presentation.
If the breech occupies lower segment termed Podalic presentation.
If the fetus lies obliquely caused shoulder presentation.
7
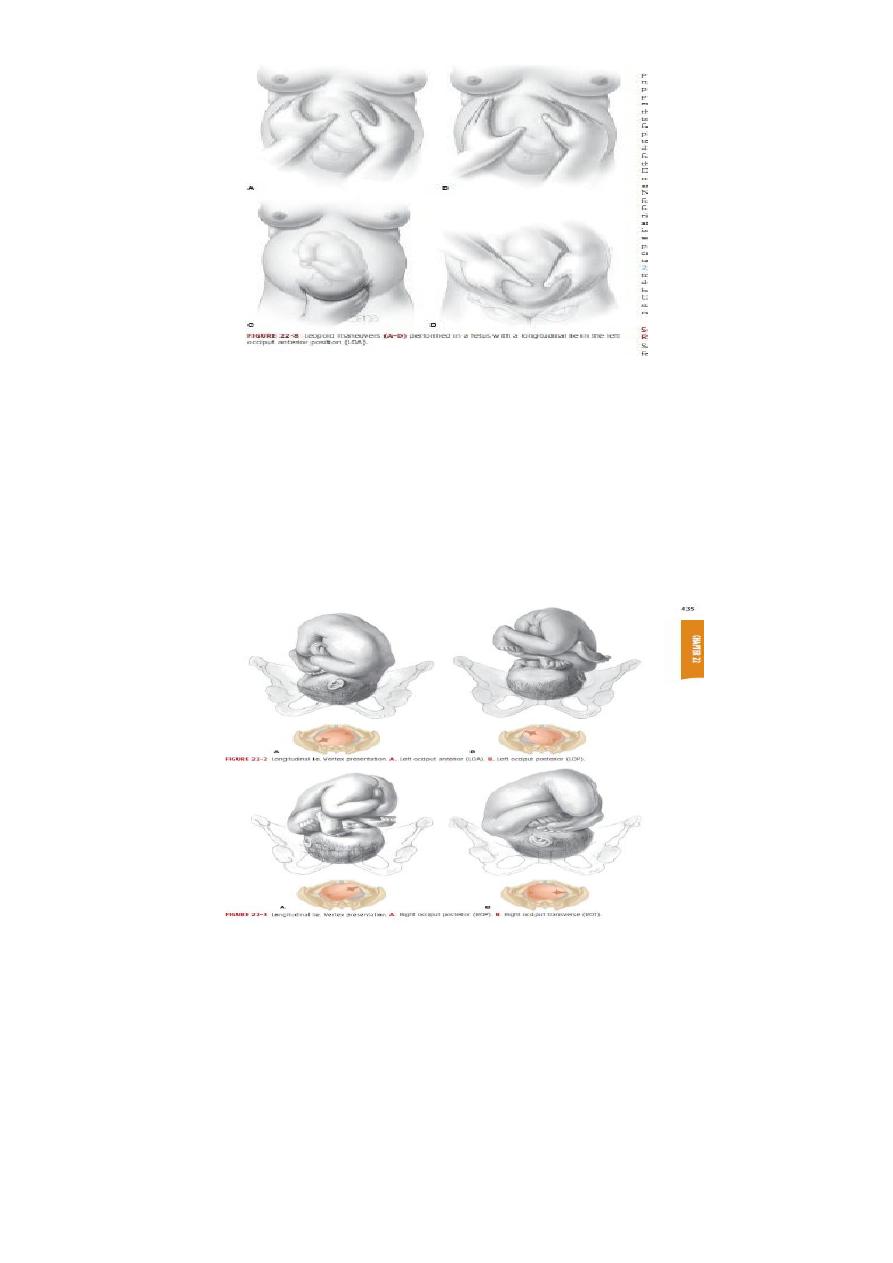
Position
The relationship between selected part of the presenting part of the fetus to maternal
pelvis [the denominator]. With vertex presentation the denominator is the occiput, with
face presentation it is the chin [mentum] & with breech presentation it is the sacrum. For
each presentation 4 positions are described, in vertex presentation; left & right
occipitoanterior position [LOA&ROA]& left & right occipitoposterior position [LOP&ROP].
Attitude
Refers to the relation of different parts of the fetus to one another. Normally the head
‘back & limbs of fetus are flexed, in some abnormal presentation head or limbs may be
extended.
8
The mechanism of labour in vertex presentation;
Engagement.
Descent.
Flexion.
Internal rotation.
Extension.
Restitution.
External rotation.
Shoulder rotation.
Delivery of fetal body.
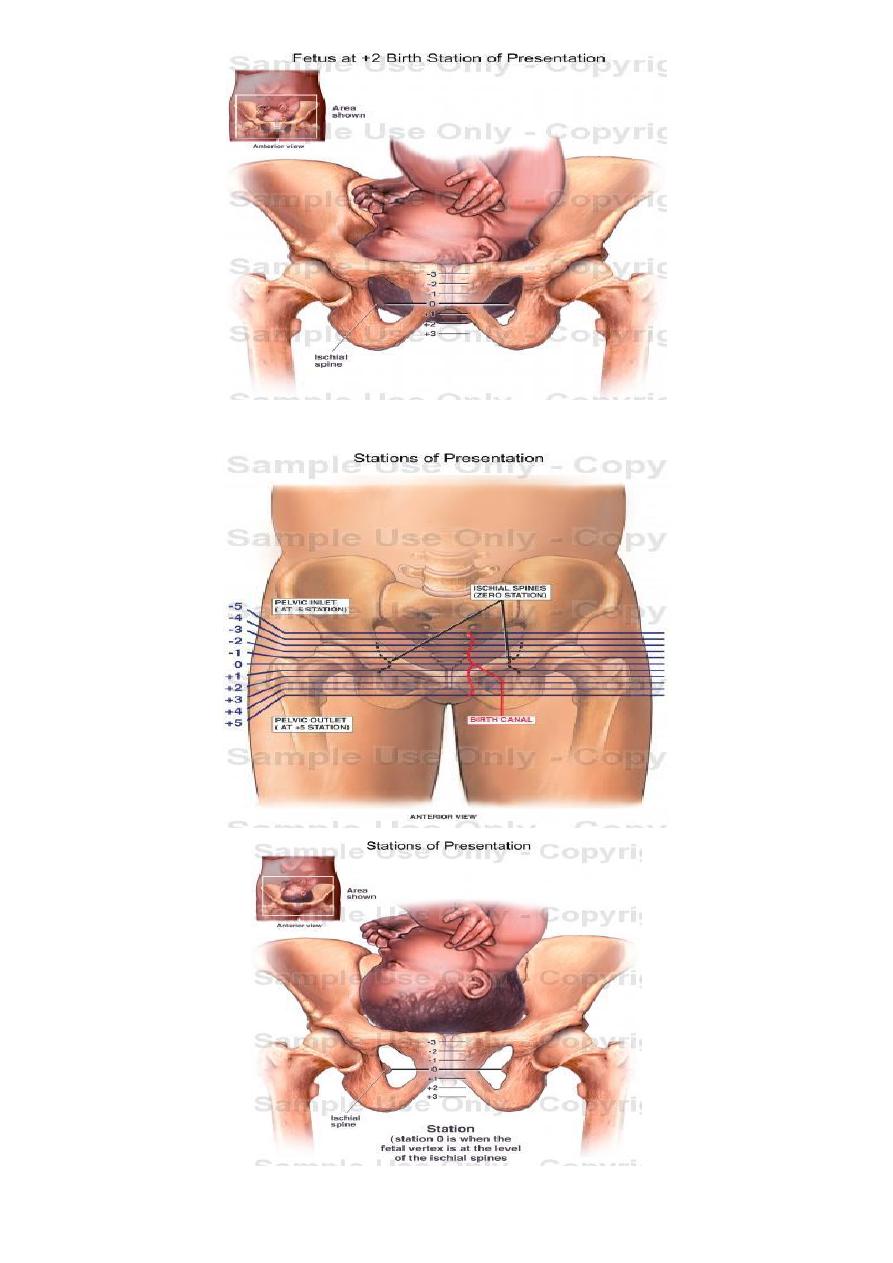
Engagement
The head normally enters the pelvis in the transverse position; engagement is occurred
when the widest part of the presenting part has passed through the inlet. It occurs in vast
majority of nulliparous women prior to labour, but not in multipara.
If more than two-fifths of the fetal head is palpable abdominally then the head is not said to
be engaged.
9

11
Descent
During the first stage & first phase of the second stage of labour descent of the fetus is
secondary to uterine action.
In the second phase of the second stage of labour descent of fetus is helped by voluntary
use of abdominal musculature.
Flexion
The fetal head may not always be completely flexed when it enters the pelvis. As the head
descends into the narrower mid cavity, flexion should occur.
This is probably as a passive movement in part due to the surrounding structures.
Internal rotation
This occurs because with a well- flexed head the occiput is leading & meets the sloping
gutter of the levator ani muscles, which by their shape direct it anteriorly; the occiput
rotate forward from the LOA or LOT position to lie under subpubic arch, with the sagittal
suture in the anteroposterior diameter of the pelvic outlet.
Extension
The well flexed head now extends with the occiput escaping from underneath the the
symphysis pubis & starting to distend the vulva, this is known as crowning of the head.
The head extends further & the occiput underneath the symphysis pubis almost acts as a
fulcrum point as the bregma, face & chin appear in succession over the posterior vaginal
opening & perineal body.
Restitution
When the head is delivering, the occiput is directly anterior. As soon as it escapes from the
vulva, the head aligns itself with the shoulders, which have entered the pelvis in the oblique
position. The slight rotetion of the occiput through one-eighth of a circle is called
restitution.
External rotation
In order to be delivered, the shoulders have to rotate into direct anterior-posterior plane.
When this occurs, the occiput rotate through a further one-eighth of a circle to the
transverse position.
11
Shoulder rotation
When restitution & external rotation have occurred ,the shoulders will be in the anterior-
posterior position. The anterior shoulder is under the symphysis pubis & delivers first & the
posterior shoulder delivers subsequently.
Delivery of fetal body
Normally the rest of fetal body is delivered easily occasionally aided by lateral movement.
A.L.Y