1
Forth stage
Obstetric
Lec-11
.د
ولدان
1/1/2016
Ectopic pregnancy
extrauterine pregnancy
Objectives:
Students will be able to:
– Define ectopic pregnancy.
– List risk factors.
– List differntial diagnosis of abdominal pain and vaginal bleeding in early pregnancy.
– Evaluate case and confirm diagnosis and justify treatment option.
Ectopic pregnancy:
It is an implantation of fertilized ovum on any site other than the endometrium of
uterus.
Ectopic pregnancy remains an important cause of maternal mortality worldwide.
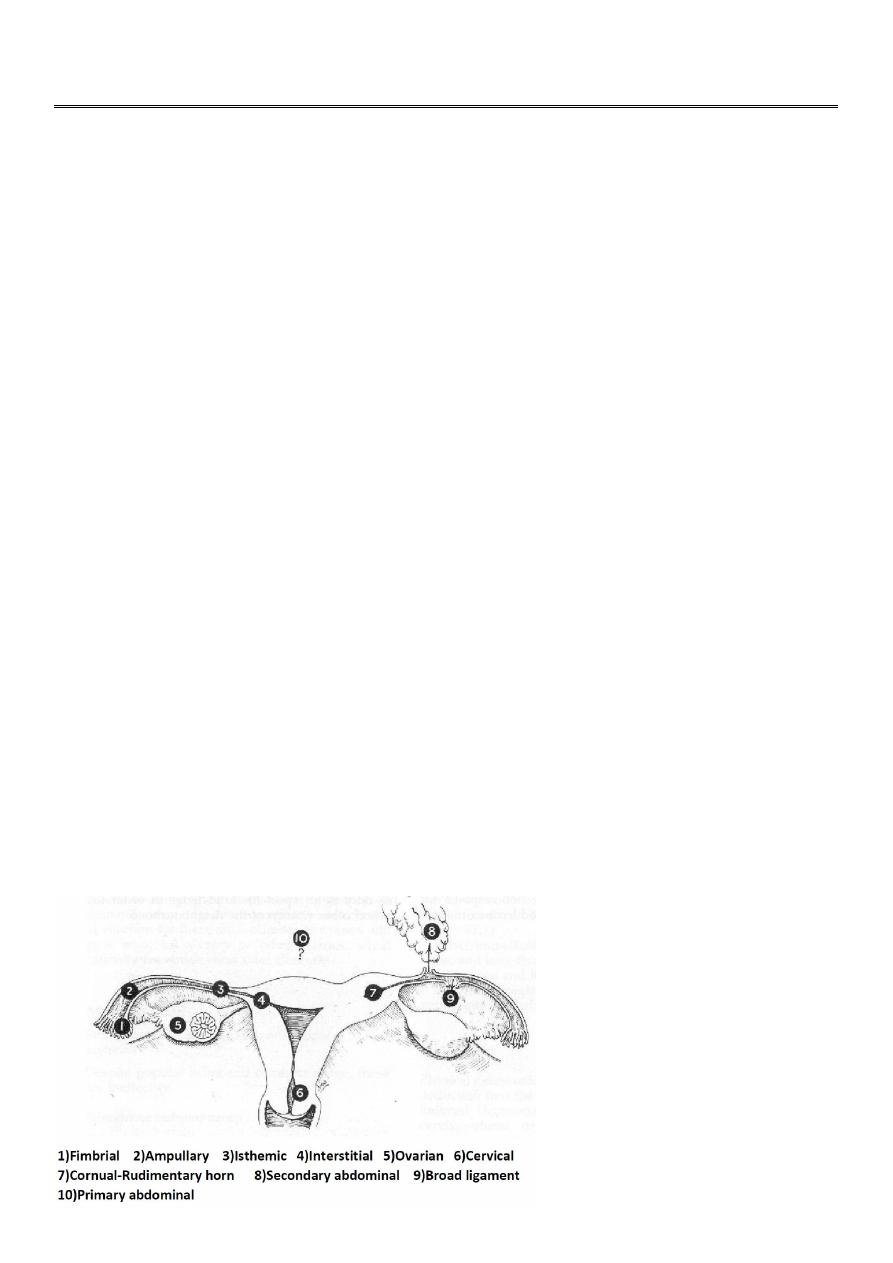
Sites of ectopic:
Fallopian tube is the most common site ( 98%), the ampulla (80%) is the most common
site of implantation.
Uterus.
Ovary.
Cervix.
Broad ligaments.
Elsewhere in peritoneal cavity.

2
Incidence:
It's incidence directly related to the prevalence of salpingitis and it is about 1% of all
pregnancy
Causes:
Any mechanical or functional factors that prevent or interfere with passage of fertilized
ovum into uterine cavity and delay it and include the following:
Pelvic inflammatory disease(PID): (Chlamydia, gonococcal, tuberculous).
Tubal surgery: (tubal sterilization, reversal of tubal sterilization).
Congenital abnormalities of fallopian tube: (diverticula, accessory ostia, hypoplasia,
Diethyl stillbesterol (DES) exposure in utero).
Peritubal adhesion: secondary to infection or surgery (appendicectomy).
Gross pelvic pathology (endometrosis).
Uterine fibroid at utero-tubal junction.
Intra uterine device (IUD) in situ (in uterus), 3-4% of pregnancy if occur, is ectopic.
Progesterone only pills.
Assisted reproductive technique (ART) increase risk of hetrotopic pregnancy(as IVF).
Risk factors for ectopic pregnancy:
History of previous ectopic pregnancy.(the risk of recurrent ectopic pregnancy is 12–
18%. The future risk increases further with every successive occurrence).
Intrauterine device (IUD) or sterilization failure.
Pelvic inflammatory disease.
Chlamydia infection.
Early age of intercourse and multiple partners.
History of infertility.
Previous pelvic surgery.
Increased maternal age.(35 years and more risk to have ectopic).
Cigarette smoking.
Strenuous physical exercise.
In utero diethylstilbestrol (DES) exposure.
Pathological anatomy:
In normal intrauterine pregnancy:
The ovum is fertilized in the Fallopian tube and then it is transported into the uterus where
there is thick deciduas (between trophoblast and uterine muscle) in which fertilized ovum
can be embeded.
In ectopic pregnancy:
in tube, there is only a very thin layer of connective tissue separating the epithelium from
muscle so it is easy for the trophoblast to erode into muscle of tube (as there is no decidual

3
formation) and no resistance to invading trophoblast and some of vessels which meet the
trophoblast opened and haemorhage occur around embryo and embryo die.
Uterus respond to hormonal changes and its enlarged and then endometrium undergoes
decidual changes.
Histologic Characteristics:
Chorionic villi, usually found in the lumen, are pathognomic findings of tubal pregnancy.
Gross or microscopic evidence of an embryo is seen in two thirds of cases.
The natural progression of tubal pregnancy (Course and outcome)
Tubal pregnancy may terminate in number of ways :
1. Tubal abortion: Part or all of the products of ectopic are expelled from the tube into
peritoneal cavity and collect in rectovaginal pouch.
2. Tubal rupture: Product of conception invade and expand the tube and cause rupture of
tube. If it occur in first few weeks, the pregnancy is situated in isthmic portion of tube. Later
rupture occur in interstial ectopic pregnancy.
3. Tubal mole: Dead embryo surrounded by clot retained in tube which may be absorbed
later on.
4. Secondary abdominal pregnancy (rare): Embryo is expelled from tube and acquires a
secondary attachment in peritoneal cavity and embryo continuo to grow.
Clinical presentation:
The clinical presentation of ectopic pregnancy is very variable.
It is largely determined by the location of pregnancy within the tube.
Asymptomatic: Discovered when patient attend antenatal clinic for booking and especially
for high risk group.
It is rare for ectopic pregnancy in tube to advance beyond 8 weeks without occurrence of
symptoms. On the other hand one third of interstitial tubal ectopics develop in a similar
way to healthy intrauterine pregnancies with evidence of a live embryo on ultrasound
examination. These pregnancies tend to be clinically silent until sudden rupture occurs.
Symptomatic:
Acute presentation (due to rupture ectopic and abortion).
Subacute presentation (due to non rupture ectopic).
Symptoms of ectopic pregnancy:
There is no pathognomonic symptoms of ectopic pregnancy but the classic triad consist of:

4
1. Abdominal pain nearly always precedes the bleeding. There is no pathognomonic pain
that is diagnostic of ectopic pregnancy.
2. vaginal bleeding.
3. Amenorrhoea.
severe continuous acute sharp abdominal pain typically referred to shoulder due to
diaphragmatic irritation intraperitoneal haemmorrhage occur in rupture ectopic and in
tubal abortion.
Discomfort and dull aching lower abdominal pain mainly on affected side in rupture
ectopic.
Amenorrhoea: most commonly symptom arise after miss period. Occasionally
symptoms arise before miss period. Sometimes 2-3 miss period in case of interstial
ectopic or ectopic in rudemintary horn of uterus.
Abnormal vaginal bleeding: the amount of bleeding varies
a.Usually bleeding is scanty and dark brown in colour.
b.in some women it can be quite heavy.
c. About 10–20% of ectopic pregnancies present without bleeding
Passage of a decidual cast may sometimes lead to an erroneous diagnosis of
miscarriage.
Examination:
Rupture ectopic pregnancy:
With rupture ectopic pregnancy and intrabdominal hemorrhage, the patient develops
tachycardia followed by hypotension (Shock state).
The abdomen is:
Distended to some degree.
Generalized tenderness and rigidity and rebound tenderness.
Bowel sounds are decreased or absent.
Pelvic examination:
Speculum examination has very little value in the detection of ectopic pregnancy. It
may help to diagnose miscarriage by the visualization of the products of conception
within the cervix or vagina.
Dark brown blood seen from cervix.
Soft cervix.
Cervical excitation (tenderness in movement of cervix) is positive although cervical
excitation is not a specific sign of an ectopic pregnancy.
Uterus slightly enlarged.
Tenderness in ectopic site.
Rarely palpable adnexal mass. Most ectopic pregnancies are very small and they
cannot be felt on palpation.

5
Unpurtured ectopic pregnancy:
Frequently, the findings before rupture and hemorrhage are nonspecific, and vital signs are
normal.
The abdomen may be not tender or mildly tender, with or without rebound.
Pelvic examination:
must be performed in an area where facilities for resuscitation are available as
examination may provoke rupture of tube.
Dark brown blood seen from cervix.
Soft cervix.
The uterus may be slightly enlarged, with findings similar to a normal pregnancy.
Cervical exitation (cervical motion tenderness) may or may not be present.
An adnexal mass may be palpable in up to 50% of cases, but the mass varies markedly
in size, consistency, and tenderness. (remember the palpable mass may be the corpus
luteum and not the ectopic pregnancy).
Differential diagnosis:
Gynecological disorder:
1. abortion.
2. ruptured corpus luteum cyst.
3. acute pelvic inflammatory disease (PID).
4. adnexal torsion.
5. degenerating fibroid.
Non gynecological disorder:
1. acute appendicitis.
2. pyelonephritis.
3. pancreatitis.
Investigation:
History and physical examination may or may not provide useful diagnostic information.
The accuracy of the initial clinical evaluation is less than 50% . Additional tests are
frequently required to differentiate early viable intrauterine pregnancy or suspected
ectopic or abnormal intrauterine pregnancy.
Ectopic pregnancy must be suspected when pregnant patient present with abnormal
bleeding and pelvic pain or in patient at risk of ectopic to prevent ruptured ectopic
pregnancy which is life threatening to mother.

6
1. ultrasound examination
detection of normal intrauterine pregnancy exclude diagnosis of ectopic pregnancy in
most of cases.
The spectrum of sonographic findings in ectopic pregnancy includes the following:
Live embryo (fetal heart positive) in adnexa which is gold slandered to diagnose
ectopic. it confirms ectopic.
Enlarged and empty uterus &/or adnexal mass &/or fluid in pouch of Douglas.
Negative pelvic ultrasound (20-30%) does not exclude ectopic pregnancy.
So wait it and repeat ultrasound in 4 days time provided there are no clinical sign of
intraperitoneal bleeding.
Transvaginal scanning provides much clearer images of pelvic structures in comparison
to transabdominal scanning and Intrauterine pregnancy can be diagnosed one week
earlier with transvaginal than with transabdominal ultrasonography
2. Serum human chorionic gonadotropin (hCG):
Serum B-hCG tests are positive in 100% of ectopic pregnancy.
Serial estimation of B-hCG concentration.
Serial serum hCG assay is particularly useful in the diagnosis of a symptomatic ectopic
pregnancy. It can distinguish between intrauterine and ectopic pregnancy as the level
of hCG doubles every 2 days in normal intrauterine pregnancy. Abnormally slow rise in
serum hCG and prolonged hCG doubling time is an indicator of an abnormal
pregnancy.
B-hCG with ultrasound scanning (Discriminatory zone):
With the use of transabdominal ultrasound, a normal pregnancy could be seen in most
cases when serum hCG exceeded 6500 IU/l .With the transvaginal ultrasound this
threshold can be lowered to 1000 IU/l.
3.
progesterone level :
progesterone level serial measurement may be helpful.
4.
Laparoscopy
It allow for direct visualization of tubes and ovaries and should be considered in women
with hCG above the discriminatory level and absence of intrauterine gestational sac on
ultrasound and if diagnosis is in doubt. Laparoscopy is the gold standard for the diagnosis of
ectopic pregnancy
5.
Culdocentesis
Used in past to diagnose rupture ectopic and not useful for diagnose of
early ectopic pregnancy. Not used nowadays as the results of culdocentesis do not always
correlate with the status of the pregnancy.
6.
uterine curttage :
not advised in routine investigation.
7. Surgery (laprotomy):
For women who present in shock, immediate surgery is both
diagnostic and therapeutic.

7
Treatment of ectopic pregnancy
Either :
1-Acute presentation (rupture ectopic) = surgery
- immediate resuscitation and intravenous fluid with blood transfusion as rapid as
possible and as needed.
- under general anesthesia laprotomy or laproscopy done.
- simple salpingectomy to affected tube with conservation of ovaries.
2-Subacute/asymptomatic presentation (unruptured ectopic)
Immediate treatment is essential and the aim to preserve tube and treat the condition before
rupture of tube .
Types of treatment:
1-medical treatment :
There is no role for medical management in the treatment of tubal pregnancy or suspected
tubal pregnancy when a patient shows signs of hypovolaemic shock.
- It can be chosen for patient who has (all of following):
1. size of ectopic pregnancy less than 4 cm.
2. unruptured tube.
3. Serum hCG level less than 1500 IU/lit.
4. No evidence of embryonic cardiac activity (fetal heart negative by ultrasound.chose
for patient
Women should be able to return easily for assessment at any time during follow-up ,
Drug used in medical treatment: methotrexate, prostaglandin( PGE2 ,PGF2α), potassium
chloride, mifipristone.
Route of administration:
- systemic methotrexate , mifipristone.
- Local injection of drug into gestational sac by laproscopy, transvaginal ,
transcervical).
Follow up:
The treatment need Follow up by Ultrasound combined with serial hCG which are essential
at interval of 1-2 days.
Active management are needed (switch to surgical treatment) if :
1. hCG level rise during follow up.
2. suspicious clinical symptoms.
3. sonographic finding develops.
2. surgery: either laparotomy or laproscope
8
The surgery of ectopic pregnancy were either conservative surgery (tubal conservation) or
radical surgery (removal of the tube) and the choice between them should be made
depending on the circumstances in each individual case. In general tubal conservation should
be attempted if a woman desires further pregnancies and there is evidence of contralateral
tubal damage.
1.Conservative surgery (removal of ectopic pregnancy and preserve affected tube) can be
done by one of following:
1. Salpingotomy (opening tube and left open to heal by secondary intention). It should be
considered as the primary treatment when managing tubal pregnancy in the presence
of contralateral tubal disease and the desire for future fertility. Women must be made
aware of the risk of a further ectopic pregnancy.
2. Fimbrial evacuation.
3. Mid tubal resection with or with out re-anastmosis.
2.Radical surgery for ectopic is salpingectomy which is indicated in :
1. severely damaged tube.
2. women who complete her family.
3. uncontrolled bleeding from implantation site.
4. large tubal pregnancy (>5 cm).
5. recurrent ectopic pregnancy in same tube
6. Persistent trophoblastic disease:
viable trophoblastic tissue remains after medical treatment and/or conservative surgical
treatment in about 5-10% and require further treatment either by methotrexate or surgery.
3.Expectant management (non-interventional ) methods:
not common to use and not suitable for all patient as it needs follow up by ultrasound and
hCG and may need active management at any time.
Remember:
If the woman is Rh-negative and her husband is Rh-positive or unknown Rh, (250unite) anti-
D immune globulin should be given intramuscularly to prevent anti-D isoimmunization.
Prognosis:
Significant factors affect future fertility after treatment of ectopic pregnancy which are:
1.Condition of controlateral tube.
2.history of infertility.
3.Extent of surgery.
Intrauterine pregnancy rates following ectopic pregnancy range between 50 and 70% .

9
Recurrent ectopic pregnancies occur in 6–16% of women with previous history of ectopics
and these women should be offered early scans in all future pregnancies to detect recurrent
ectopics before complications can occur.
Pregnancy rates are similar in patients treated by either laparoscopy or laparotomy.
In women with a damaged or absent controlateral tube, in vitro fertilization is likely to be
required if salpingectomy is performed.
Abdominal pregnancy (Non tubal pregnancy)
Rare condition and it is associated with high morbidity and mortality, with the risk for death
7 to 8 times greater than from tubal ectopic pregnancy and 90 times greater than from
intrauterine pregnancy.
Symptoms and signs:
1.history suggest ectopic pregnancy in early pregnancy sometimes.
2.a symptomatic and suspected from examination.
3.persistant abnormal lie.
4.fetal parts are readily palpated.
5.enlarged uterus felt separate from fetus.
Investigations:
1.ultrasound show no clear outline of gestational sac and oligohydramnios and early
intrauterine growth resriction (IUGR).
In women with a clinical suspicion of abdominal pregnancy a transvaginal scan should be
performed to assess the uterus and establish the continuity between the cervical canal, uterine
cavity and gestational sac
2.X-ray of abdomen showed maternal intestinal gas superimposed on fetus.
3.oxytocin infusion which cause uterine contraction which felt separately from fetal part
course:
1.alive fetus reaches viability.
2. fetus die and thrombosis of vessel at placental site gradually occur and there will be either
no symptome ,or complications could arise.

11
Treatment :
Treatment of abdominal pregnancy is surgical by laprotomy as soon as viability is achieved
because fetus will die once labour begin.
The fetus should be removed, the cord cut short and the placenta should be left in situ. Any
attempt to remove the placenta may result in massive uncontrollable haemorrhage. the
residual placental tissue will absorb slowly over a period of many months, sometimes a few
years.
Complications of abdominal pregnancy:
1.maternal complications:
A. complication arising due to placenta in situ:
- infection.
- adhesion.
- obstruction.
- coagulopathy.
B . complication arising due to fetal death in peritoneal cavity:
- Adhesion
- infection of sac and severe toxic effect
2- Fetal complications:
- Pressure deformity.
- Increase perinatal mortality to 75% or more.
Hetrotopic pregnancy:
Is combined ectopic and intrauterine pregnancy .
Treated by either:
1-injection of hyperosmolar glucose in ectopic site.
2-Surgical removal of ectopic.
Prognosis:
75% of intrauterine pregnancy reach term.
Don’t miss this---- Ectopic pregnancy in
women should be in mind i