
1
Forth stage
Obstetric
Lec-1
.د
هبة
1/1/6112
Anatomical and physiological changes during pregnancy
Anatomical and physiological changes during pregnancy:
Every maternal organ adapts to pregnancy, each at different time and way to accommodate
the increasing demand of fetal growth and development.
In early pregnancy the developing fetus , the placenta and the corpus luteum produce
large quantities of hormones ,growth factors and other substances in to the maternal
circulation that triggers the maternal systems to transfer from nonpregnant to pregnant
form.
This changes report usually by the end of the 6th weeks after the LMP, this adaptations are
to:
1. Increase the availability of precursors for hormonal production.
2. Improve transport capacity.
3. Maternal –fetal exchange of oxygen and various nutrient.
4. Removal of additional risk factors.
Volume homeostasis
Blood volume expands during pregnancy to allow adequate perfusion to the vital maternal
organs , placenta and fetus
The increase mainly involve the extracellular fluid volume especially plasma and begun at 6-
8wk, plateau at 32-34wks.
The total body water increase from 6.5 to 8.5L by the end of pregnancy.
Factors contributing to fluid retention:
1. Sodium retention.
2. Decrease thirst threshold.
3. Decrease plasma oncotic pressure.
4. Decrease plasma albumin as a result of hemodilution.
Consequence of fluid retention
1. Decrease Hemoglobin concentration and hematocrit
2. Decrease serum albumin level
3. Increase stroke volume.
4. Increase renal blood flow

2
Hematology (blood)
Hemoglobin concentration fall from 13.3 to 10.9 g/dL because of the discrepancy
between the 1000-1500 ml increase in the plasma volume and the increase in the
erythrocyte mass 280ml.
Iron demand increases leading to increase iron absorption from GIT.
Increase in TIBC (iron transporting mechanism).
Pregnancy without iron supplementation may lead to depletion of the iron
stores (serum ferritin, bone store).
Plasma folate decrease due to increase GFR but RBC folate do not to decrease to the
same extend.
Maternal platelet count usually unchanged or it may be reduced due to aggregation,
increase platelet count in postpartum period so increase thromboembolic event at this
period.
WBC count increase in pregnancy this mainly the poly morph nuclear cells from the
3
rd
weeks of gestation and more pronounced in the postpartum.
ESR is increased.
Haemostasis and coagulation
Pregnancy is a hyper coagulable state and return to normal after 4 weeks
postpartum , at term about 500 ml of blood pass to the placental bed every
minutes so without effective hemostatic mechanism woman may rapidly die from
blood loss.
Almost all clotting factors including and serum fibrinogen are increased.
Reduction in plasma fibrinolytic activity.
Respiratory system
Anatomical changes
The neck, oropharyngeal tissues, breasts and chest wall are affected by weight gain
during pregnancy and may lead to difficult intubation during general anesthesia.
The vascularity of the respiratory tract mucosa increases leading to nasal congestion
and bled easily.
As pregnancy progresses the diaphragm is elevated 4cm by the enlarging uterus.
The lower ribcage circumference expands by 5 cm.
Respiratory muscle function unaffected.
Increase pulmonary blood flow.
3
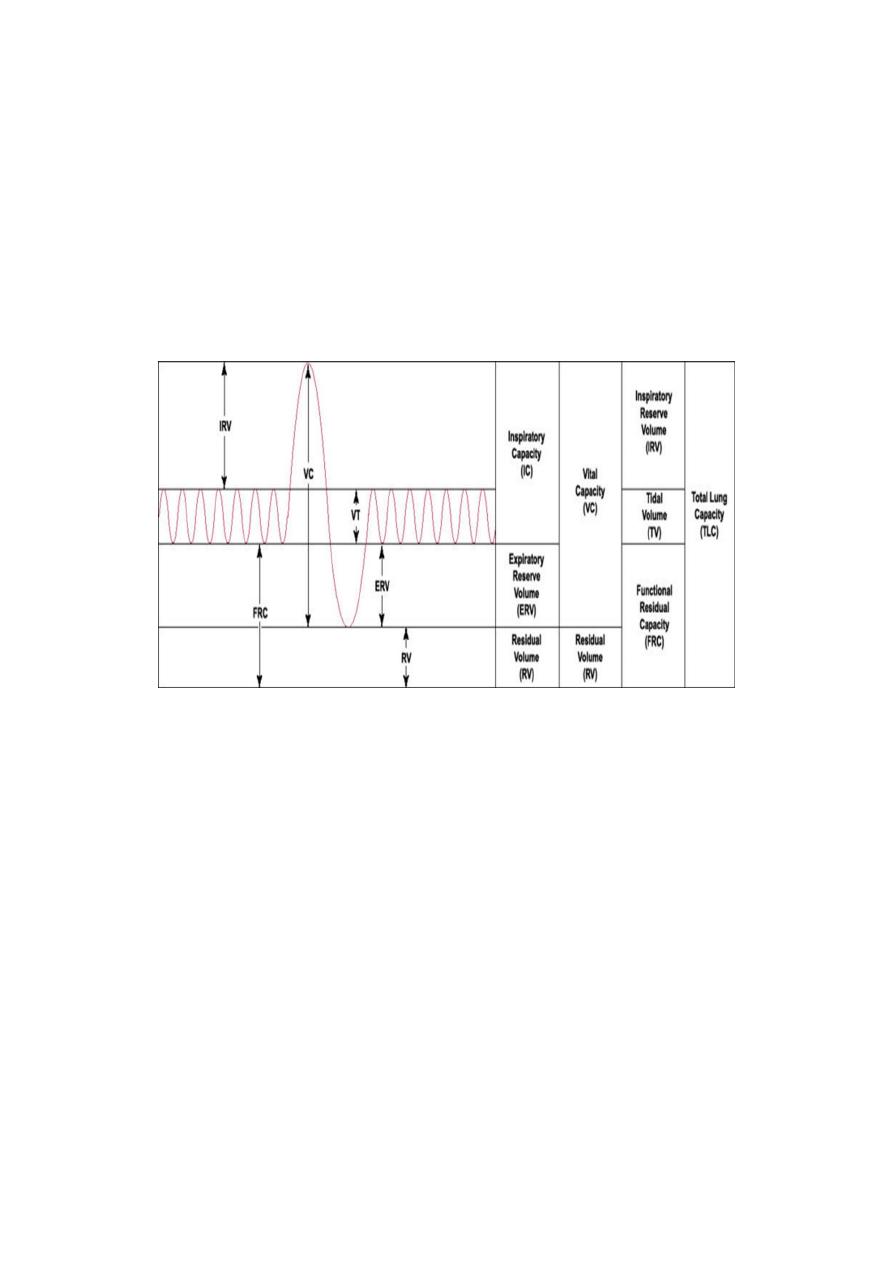
Physiological changes
Increase in the tidal volume from 8 weeks ( in response to progesterone And
increase metabolic demand ).
Increase minute ventilation by 40% (amount of air move in and out of lungs in 1minute)
which is the results of tidal volume and respiratory rate.
Mild physiological dyspnea common in 5 0%of women.
Vital capacity unchanged or slightly increase.
Decrease residual volume of the lung as a result of elevation of the diaphragm.
All these changes don’t affect the interpretation of the tests of the ventilation (forced
expiratory volume in 1 second and peak expiratory flow rate).
Blood gas changes
Decrease pco2.
Increase po2.
Increase o2 availability to tissues and placenta.
Increase production of 2,3 diphosphoglcerate ( 2,3 DPG ) within the maternal RBCs
to facilitated oxygen delivery to the fetus .
Cardiovascular system
Increase heart rate 10-20% since early gestation and together with the increase
stroke volume 10 % lead to an increase in the cardiac output by ( 30-50% ) as the
cardiac output =stroke volume X heart rate.
A reduction in the diastolic pressure by about 10-15 mmHg are more than systolic
pressure which about 5-10 mmHg leading to increase pulse pressure , later on
diastolic pressure increase to pre regnancy level measuring by korotkoff 5 which is the
disappearance of sound during blood pressure measurement.

4
Findings on cardiovascular examination:
Palpitation are common (Premature atrial and ventricular ectopic beats are common)
Decrease in mean arterial pressure (10%) as a result of decline in the peripheral
vascular resistance.
Large pulse volume.
First heart sound loud and may be spliting.
Audible third heart sound 80%.
Ejection systolic murmur 90%.
Continuous systolic murmur 10% due to increase mammary blood flow.
Diastolic murmur 20%.
ECG Changes
Increased heart rate
Left axis deviation.
Inverted T-wave in lead ІІІ.
Q in lead ІІІ & AVF.
Nonspecific ST segment changes.
Aortocaval Compression
From mid-pregnancy, the enlarged uterus compresses both the inferior vena cava
and the lower aorta when the patient lies supine; Compression of the aorta may lead
to a reduction in uteroplacental and renal blood flow.
Compression of the inferior vena cava by the gravid uterus impairs venous return to
the heart in supine position . A women will develop significant supine hypotension,
and loss of consciouseness is possible. By rolling over on to the left side, cardiac output
is return to normal.
Gut
Progesterone causing decrease lower esophageal sphincter tone together with elevation of
the diaphragm increase the chance of reflux esophagitis.
Also progesterone delay stomach and bowel motility leading to constipation, hemorrhoid,
and increase the risk of aspiration of the gastric content during general anesthesia
Liver
Increase hepatic blood flow.
Liver function unchanged.
Increase protien production especialy albumin.
Serum ALT and AST are slightly reduced.
Serum alkaline phosphatase increase due to placental production.

5
The kidney and urinary tract
Anatomical changes
Kidney increase in size with 1-2cm.
Increase in the length , there is dilatation of pelvic calycesis systems under the
influence of progesterone and return to normal by 6 weeks postpartum.
Increase renal blood flow by 80% in the 2nd trimester.
Physiological changes
Increase glomerulofilteration rate by 50% after conception.
Creatinine clearance increased by 25%.
Plasma renin and angeotensin 2 activity are increased.
plasma urea , creatinine , uric acid are decreased due to increase renal excretion
.
Sodium and potasium metabolism remain unchanged.
Renal excretion of calicium, proteins and folic acid increase.
Glycosuria are common and normal in uncomplicated pregnancy due to increase
GFR and exceeding renal threshold for the tubular absorption.
Reproductive organs
Uterus
High level of maternal oestradiol and progesterone stimulate both hyperplasia
and hypertrophy of the myometrial cells , increasing the weight of the uterus from
70 gm prior to pregnancy to 1000gm by term.
In early pregnancy, uterine growth is independent of the growing fetus, and occurs
equally rapidly with an ectopic pregnancy.
As well as changes in the size and number of myometrial cells, specialized cellular
connections also develop with increasing gestation. (the intercellular gap junctions
)allow changes in membrane potential to spread rapidly from one cell to another ,
facilitating the spread of membrane depolarization , and subsequent myometrial
contraction. These allow the pacemaker activity of the uterine fundus to promote the
coordinated, fundal dominant contractions necessary for labour.
Normally the uterus is anteverted but become more axial and vertical when enlarged
and rotate in its long axis, usually to the right.
Cervix
Early in pregnancy the cervix become soft and its color change to purple due to
increase vascularity .
The cervix become soft inconsistancy (Hegirs sign)
Hypertrophy & hyperplasia of the cervical glands.

6
Cervical mucosal cells produce large amounts of thick mucus that obstructs the
cervical canal soon after conception ( mucus plug ) , it has abundance of leucocytes
and acts as antibacterial and mechanical barrier.
Vagina
Increased vascularity of the vagina resulting in the violet color characteristic of
pregnancy.
Estrogen cause thickening of the vaginal epithelium with increase rate of
desquamation , glycogen storage and lactic acid production , transudation of the
fluid resulting in increase in the acidic vaginal discharge .
Breast
Tenseness and pain in the breast are the symptoms of pregnancy.
The breast progressively increase in size as result of the proliferation of the
glands and deposition of fat within the breast with the dilatation of the
superfascial veins .
The primary areola become larger and darkly pigmented.
Secondary pigmented areola develops around the primary areola.
The sebaceous gland appear as a small rounded papules (Montgomery's tubercules).
Estrogen causing increase glandular ducts formation while Progesterone and
human placental lactogen increase glandular alveoli proliferation.
Skin Changes
Chloasma or the mask of pregnancy is hyperpigmentation with irregular areas on
the cheeks and nose , it may be due to melanocyte stimulating hormone produced
by the placenta and estrogen and progesterone which may also have a melanocyte
stimulating effect.
Striae gravidarum : Reddish to purple depressed lines develop in the skin of
the abdomen , breasts and thighs , after pregnancy becomes silvery white due to
stretching of the skin and breaking of the underlying tissue.
Linea nigra: The midline of the abdominal skin that extending from the umbilicus to
the symphysis pubis becomes pigmented, brownish-black color.
Sebaceous glands activity increase.
Pruritus and hirsuitism are common.