1
Forth stage
Obstetric
Lec-6
.د
امنة
1/1/2016
Shock in obstetrics
Shock is a condition resulting from inability of the circulatory system to provide the tissues requirements
from oxygen and nutrients and to remove metabolites.
Types & causes
1.Haemorrhagic shock excessive blood loss may be due to:
...Causes of bleeding early in pregnancy.
...Causes of antepartum haemorrhage.
...Causes of postpartum haemorrhage.
2.Neurogenic shock painful conditions my be due to:
...ectopic pregnancy.
...Concealed accidental haemorrhage.
...Forceps or breech extraction before full cervical dilatation.
...Rough internal version.
...Rupture uterus.
...Acute inversion of the uterus.
...Rapid evacuation of the uterine contents as in precipitate labour and rupture of membranes in
polyhydramnios. This is accompanied by rapid accumulation of blood in the splanchnic area due to sudden
relief of pressure (splanchnic shock).
3.Cardiogenic shock: ineffective contraction of the cardiac muscle due to
...Myocardial infarction.
...Heart failure.
4.Endotoxic shock: generalised vascular disturbance due to release of toxins.
5.Anaphylactic shock: caused by sensitivity to drugs.
6.Other causes:
...Embolism: amniotic fluid, air or thrombus.
...Anaesthetic complications: as Mendelson's syndrome.
The shock may be caused by more than one factor as:*Incomplete abortion: leads to haemorrhagic and
endotoxic shock. *Disturbed ectopic and rupture uterus: lead to haemorrhagic and neurogenic shock.
2
Classic Clinical Picture of Shock
1~Low blood pressure.
2~Rapid weak (thready) pulse.
3~Pallor.
4~Cold clammy sweat.
5~Cyanosis of the fingers.
6~Air hunger.
7~Dimness of vision.
8~Restlessness.
9~Oliguria or anuria.
1--Haemorrhagic shock
Classification of hemorrhagic shock
Class . blood loss . clinical pictures
1 . 15% Norma pulse & normal bl pressure.tilt test +'ve.
2 . 20-25% tachycardia, tachypnoea, low systolic pressure
3 . 30-35% skin:cold,clammy,pale. severe drop in bl.press.
oligurea,metabolic acidosis ..
4 . 40-45% profound hypotension, irreversible shock .
Tilt test
It is done in patient with considerable bleeding but the blood pressure and/ or pulse rate are normal.
When this patient is in a sitting position, she develops hypotension and / or tachycardia.
Phases of Haemorrhagic Shock
The normal pregnant woman can withstand blood loss of 500 ml and even up to 1000 ml during delivery
without obvious danger due to physiological cardiovascular and haematological adaptations during
pregnancy.
1-Phase of compensation
Sympathetic stimulation:Its the initial response to blood loss leading to peripheral vasoconstriction to
maintain blood supply to the vital organs. Clinical picture: Pallor, tachycardia, tachypnoea.
3
2-Phase of decompensation
Blood loss exceeds 1000 ml in normal patient or less if other adverse factors are operating.
Clinical picture: is the classic clinical picture of shock (see before).
Adequate treatment at this phase improves the condition rapidly without residual adverse effects.
3-Phase of cellular damage and danger of death
Inadequately treated haemorrhagic shock results in prolonged tissue hypoxia and damage with the
following effects:
°Metabolic acidosis: due to anaerobic metabolism initiated after lack of oxygen.
°Arteriolar dilatation: caused by accumulation of metabolites leading to pooling and stagnation of blood
in the capillaries and leakage of fluid into the tissues.
°Disseminated intravascular coagulation: caused by release of thromboplastin from the damaged tissues.
°Cardiac failure: due to diminished coronary blood flow.
In this phase death is imminent, transfusion alone is inadequate and if recovery from acute phase occurs
residual tissue damage as renal &/or pituitary necrosis will occur.
Management
Urgent interference is indicated as follow:
1-Detect the cause and arrest haemorrhage.
2-Establish an airway and give oxygen by mask or endotracheal tube.
3-Elevate the legs to encourage return of blood from the limbs to the central circulation.
4-Two or more intravenous ways are established for blood, fluids and drugs infusion which should be given
by IV route in shocked patient. If the veins are difficult to find a venous cut down or intrafemoral
canulation is done.
5-Restoration of blood volume by:Whole blood: cross-matched from the same group, if not available,
group O-ve may be given as a life-saving.Crystalloid solutions: as ringer lactate, normal saline or glucose
5%. Colloid solutions: as dextran , plasma protein fraction or fresh frozen plasma.
6-Drug therapy:
..Analgesics: 10-15 mg morphine IV if there is pain, tissue damage or irritability.
..Corticosteroids: Hydrocortisone 1gm or dexamethasone 20 mg slowly IV. Its mode of action is
controversial; it may decrease peripheral resistance and potentiate cardiac response so it improves tissue
perfusion.
..Sodium bicarbonate: 100 mEq IV if metabolic acidosis is demonstrated.
..Vasopressors: to increase the blood pressure so maintain renal perfusion.
..Dopamine: 2.5m g/ kg/ minute IV is the drug of choice.

4
..ß -adrenergic stimulant: isoprenaline 1mg in 500 ml 5% glucose slowly IV infusion.
7.Monitoring
..Central venous pressure (CVP): normal 10-12 cm water.
..Pulse rate.
..Blood pressure.
..Urine output: normal 60 ml/hour.
Clinical improvement in the: pallor, cyanosis, air hunger, sweating and consciousness .
Complications
1-Acute renal failure.
2-Pituitary necrosis (Sheehan’s syndrome).
3-Disseminated intravascular coagulation.
2--Endotoxic (septic or bacteraemic shock )
Sepsis induced hypotension that persists despite treatment with IV . fluid. It's systemic response to
infection+>2 SIRS criteria.
Systemic inflammatory response syndrome(SIRS) manifested by 2 or more of the following ;
※Temperature>38C°or <36C°.
※Heart rate>90 beats/min.
※Respiratory rate>20 breaths/min or PaCo²<32mmHg.
※WBC>12000/mm³ or<4000/mm³.
Obstetric Causes;
..Septic abortion.
..Prolonged rupture of membranes.
..Manipulations and instrumentations.
..Trauma.
..Retained placental tissues.
..Puerperal sepsis.
..Severe acute pyelonephritis.
5
Causative Organisms
Gram-negative bacilli: E.coli, proteus, pseudomonas and bacteroids. The endotoxin is a
phospholipopolysaccharide released by lysis of its cell envelope.
A similar picture is produced from exotoxin of ß-haemolytic streptococci, anaerobic streptococci and
clostridia.
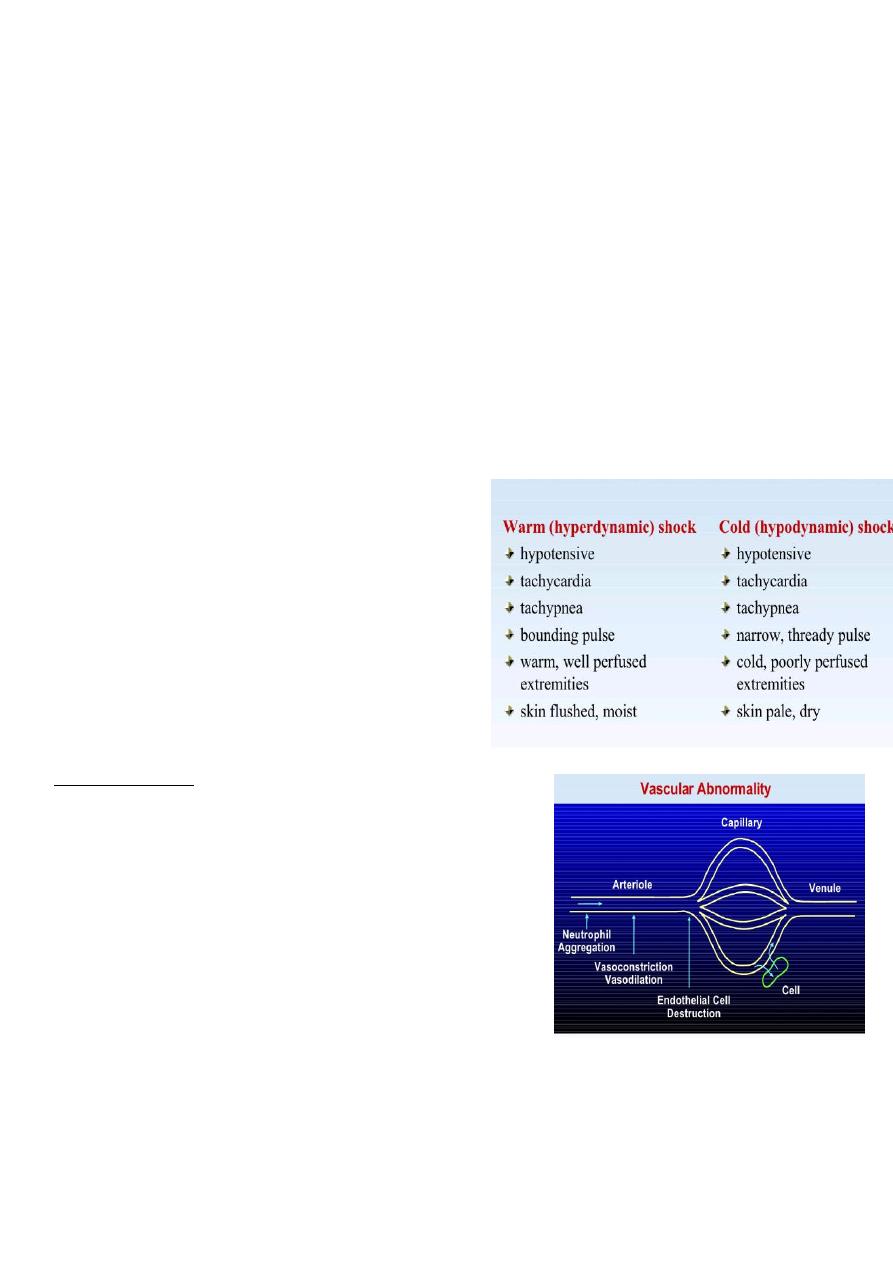
Pathology
Release of endotoxin results in increased lysosomal permeability and cytotoxicity. The sequence of events
thereafter may occur in few minutes and include:
Stimulation of the adrenal medulla and sympathetic nervous system → constriction of arterioles and
venules → local acidosis → arteriolar dilatation but with continuing constriction of the venules → capillary
pooling of blood → haemorrhagic engorgement of bowel, liver, kidneys and lungs.There is associated
extensive disseminated intravascular coagulation . See fig.1
Fig.1
Clinical features
1....Reversible stage,
It has 2 phases:
2....Irreversible stage,
Prolonged cellular hypoxia leads to:
metabolic acidosis,
acute renal failure,
cardiac failure,
pulmonary oedema,
adrenal failure and ultimately death.
Differential diagnosis
*Amniotic fluid embolism.
*Pulmonary embolism.
6
*Pulmonary aspiration syndrome.
*Myocardial infarction.
*Incompatible blood transfusion.
Management
It includes 3 major lines of treatment:
1-Restoration of circulatory function and oxygenation
…Replacement of blood loss: by whole blood, if not available start with colloids or crystalloids. The CVP
measurement is essential to guard against circulatory overload.
...Corticosteroids: as; Hydrocortisone 1gm IV / 6 hours or Dexamethasone 20 mg initially followed by 200
mg/day by IV infusion.
...β-adrenergic stimulants: as isoprenaline cause arteriolar dilatation, increase heart rate and stroke
volume improving tissue perfusion. Blood volume must be normal prior to its administration.
...O2 if respiratory function is impaired .
...Aminophylline: improves respiratory function by alleviating bronchospasm.
...Correction of fluid & electrolyte deficits .
...Treatment of DIC.
2-Eradication of infection
…Swabs for culture and sensitivity are taken first.
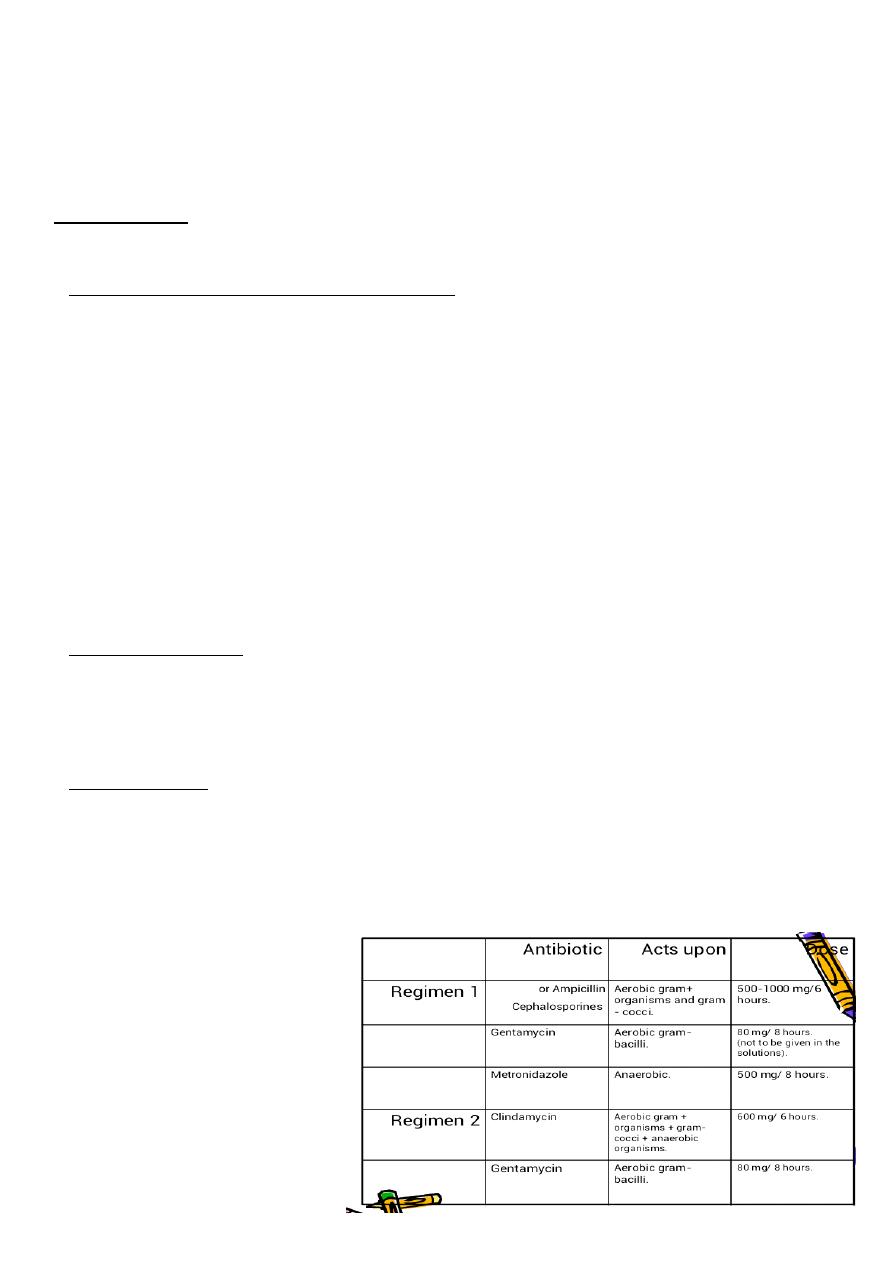
…Antibiotic therapy is starting immediately till the result of culture & given by IV route. The therapy
should cover the wide range of organisms: in fig.2
3-Surgical treatment
is indicated when there is retained infected tissues as in septic abortion. It should be removed as soon as
antibiotic therapy and resuscitative measures have been started by:suction evacuation,
digital evacuation, or hysterectomy in advanced infection with a gangrenous (clostridium welchii) or
traumatised uterus + fresh blood transfusion in case of active bleeding.
Fig.2
7
AMNIOTIC FLUID EMBOLISM
Definition
Passage of amniotic fluid into the maternal circulation leads to sudden collapse during labour but can only
be confirmed at necropsy.
Pathology
The condition is more common with strong uterine contraction occurs after rupture of membranes
particularly when there are open maternal blood vessels in the placental site or in cervical lacerations.The
embolism passes to the pulmonary vessels leads to:sudden death, shock, or later death due to DIC and PPH
Clinical Picture
The onset is acute with sudden collapse, cyanosis and severe dyspnoea. This is soon followed by twitching,
convulsions and right side heart failure, with tachycardia, pulmonary oedema and blood stained frothy
sputum. If death does not occur in this stage, DIC develops within 1 hour leading to generalised bleeding.
Investigations
*ECG: evidence of right side heart failure.
*X-ray: non-specific mottled chest appearance.
*Lung scan: with technetium-99m albumin shows perfusion defect.
*Laboratory tests: evidence of DIC.
Differential Diagnosis
*Acute pulmonary oedema.
*Pulmonary aspiration (Mendelson’s) syndrome.
*Other coagulation defects.
Treatment
Urgent treatment includes:
1-Oxygen: endotracheal intubation and positive pressure respiration is usually indicated as the patient is
often unconscious.
2-Drugs as:
..Aminophylline: 0.5 gm slowly IV to reduce bronchospasm.
..Isoprenaline:0.1gm IV to improve pulmonary blood flow and cardiac activity.
..Digoxin and atropine: if CVP is raised and pulmonary secretions are excessive.
..Hydrocortisone: 1 gm IV followed by slow IV infusion causes vasodilatation and improves tissue perfusion.
..Bicarbonate solution: if there is respiratory acidosis.
..Low molecular weight dextran: reduces platelets aggregation in vital organs.
..Heparin: for treatment of DIC if there is no active bleeding.
..Vaginal delivery: is safer than CS if the baby is not yet delivered.