
1
Forth stage
Obstetric
Lec-7
.د
ا
سماء
1/1/2016
RH -ALLOIMMUNIZATION
The Rh factor (ie, Rhesus factor) is a red blood cell surface antigen. Rhesus family include
these antigen D ,C ,E ,d ,c ,e .
A person is Rh-positive if they possess the D allele and Rh negative if it is absent .
Rh isoimmunization: is an immunological condition that occurs in a pregnant , Rh-negative
patient carrying an Rh positive fetus .
The incidence of Rh –ve individuals varies by race .In north america caucasian ,the
incidence of Rh –ve genotype is 15%.
Alloimmunization may occur to other antigen As Kidd antigen and less common as Kell,
and Duffy
Rh antigen is inherited as two set of three alleles ,each seat is Inherited from one parent.
These alleles are : Cc,Dd,Ee,
An individual may be homozygous or heteroozygous for each of these alleles.
The presence of the D antigen determines whether an individual is Rh positive or
negative.
Individual genotype can be directly determined by Polymerase chain reaction technology.
Alloimmunization of the Rh negative mother to the fetal Rh positive antigen occurs by :
Transplacental fetal to maternal haemorrhage (most common(
most commonly after delivery (90%) and may be after abortion , trauma in pregnancy
,obstetric procedure .
Heterologous blood transfusion (second common).
Type of immune response to the D antigen:
Primary immune response occurs over six weeks to twelve months ,weak response ,
predominantly of IgM ,1st pregnancy is not affected by haemolysis.

2
The secondary immune response is rapid ,IgG .
Once maternal Rh immunoglobulin G (IgG) antibodies are produced ,they may cross freely
from the placenta to the fetal circulation, where they form antigen-antibody complexes
with Rh-positive fetal erythrocytes and eventually are destroyed, resulting in a fetal
alloimmune hemolytic anemia.
Although the Rh blood group systems consist of several antigens (D, C, c, E ,e), the D
antigen is the most immunogenic; therefore , it most commonly is involved in Rh
Incompatibility .
All the sequelae of Rh alloimmunization are the result of haemolytic anaemia and may
develops slowly or rapidly .
There is
:
Anemia
-
Raise in the retic count .
- Erythroblastosis (nucleated RBC are released into the circulation) .
Hyperbilirubinaemia : all the bilirubin in the fetus is indirect ,the albumine unbound
fraction may penetrate the lipid neuronal membrane cause cell death ,development
of encephalopathy (kernicterus) ,profound neurosensory deafness ,and
chorioathetoid spastic cerebral palsy in survivors.
Hydrops fetalis result from :
-Hb deficit .
-portal hypertension Liver and spleen are enlarged because of extramedullary
hematopoiesis and congestion.
-Hypoalbuminaemia secondary to liver dysfunction.
-Cardiac dysfunction .
The incidence of Rh alloimmunization has declined dramatically due to:
Immunoprophylaxis
smaller families.
Management of Rh negative unsensitized women during pregnancy:
The patient should have two records of blood group and Rh that are in agreement.
Test the father if Rh positive or negative .

3
Rh positive father could be homozygous and all the off spring will be Rh positive.
if he is heterozygous there is 50% chance that the fetus will be Rh negative .
if the father is Rh negative nothing should be done.
Indirect coombs test performed at booking
, and repeated at monthly intervals
from 18 -20weeks to predict sensitization.
level < 1:4 is unsensitized.
Cover any potential sensitizing event during pregnancy as vaginal bleeding or trauma
during pregnancy with Anti-D immunoglobulin
05 microgram (250 IU) before 22 weeks.
100 microgram (500 IU) after 22weeks
Anti-D immunoglobulin prophylaxis should be
administered to all non sensitized Rh –ve women at 28 weeks gestation.
At delivery cord blood is obtained to determine the neonatal ABO and Rh type and
direct coomb’s test to detect antibody attached to the fetal RBC.
Anti-D immunoglobulin 300 microg should be administered to the mother to prevent
maternal sensitization to < 30 ml of fetal Rh positive blood .
Larger dose of Anti -D immunoglobulin should be given in cases of larger fetal to
maternal haemorrhage ,such as in cases of C.S. ,manual removal of the placenta , trauma
,APH, IUD ,twin .
Maternal blood is screened by Kleihauer - Betke test to assess the volume of fetal to
maternal haemorrhage.
The maternal blood is fixed on a slide by ethanol and treated with citrate phosphatebuffer
which readily remove the adult HB but not the fetal Hb .
After staining the fetal cells can readily distinguished and counted from the empty
maternal cells.
N. of fetal cells = X .
N. of maternal cells estimated maternal blood vol.(ml)
X : is the estimated fetal blood volume
4
Management of sensitized Rh negative women :
Non – invasive evaluation :
We should predict the fetal risk in this pregnancy by :
Past obstetric history : the magnitude of fetal and neonatal disease typically progress
from one pregnancy to another .
Maternal indirect coombs antibody titer ,should be assessed monthly ,there is a
critical titer below which sever haemolytic disease does not occur and any invasive
fetal monitoring is deferred until the critical titer is exceeded .
level <= 1:32 should be followed by non invasive method .
Level >= 1:64 should be followed by invasive method
In subsequent pregnancies once the threshold is crossed ,titer and history are inadequate
measures upon which to base management.
PCR is used to determine the fetal genotye and whether the fetus is antigen positive
Rh negative baby obviate the need for further follow up.
High resolution ultrasonography for monitoring of the fetus to predict haemolytic
anemia and hydrops ,amniotic fluid volume, liver and spleen length and
thickness,placental thickness, cardiac biventricular thickness ( not proven to be
reliable ).
Doppler blood flow velocities used for screening for fetal anemia.
Invasive evaluation:
Two invasive methods are used to search for fetal anemia secondary to haemolytic disease
after the indirect coombs test exceed the local threshold.
These are :
Indirect : spectrophotometry ( delta OD 450) on amniotic fluid sample gained by
ultrasound guided technique (amniocentesis).
PCR to detect the blood group and Rh of the fetus .
Direct : fetal blood studies by cordocentesis.
Hb , Bd group and Rh, retics ,serum bilirubin,
serology (direct coombs test) .
The method chosen depend on facility available and doctor experience .
5
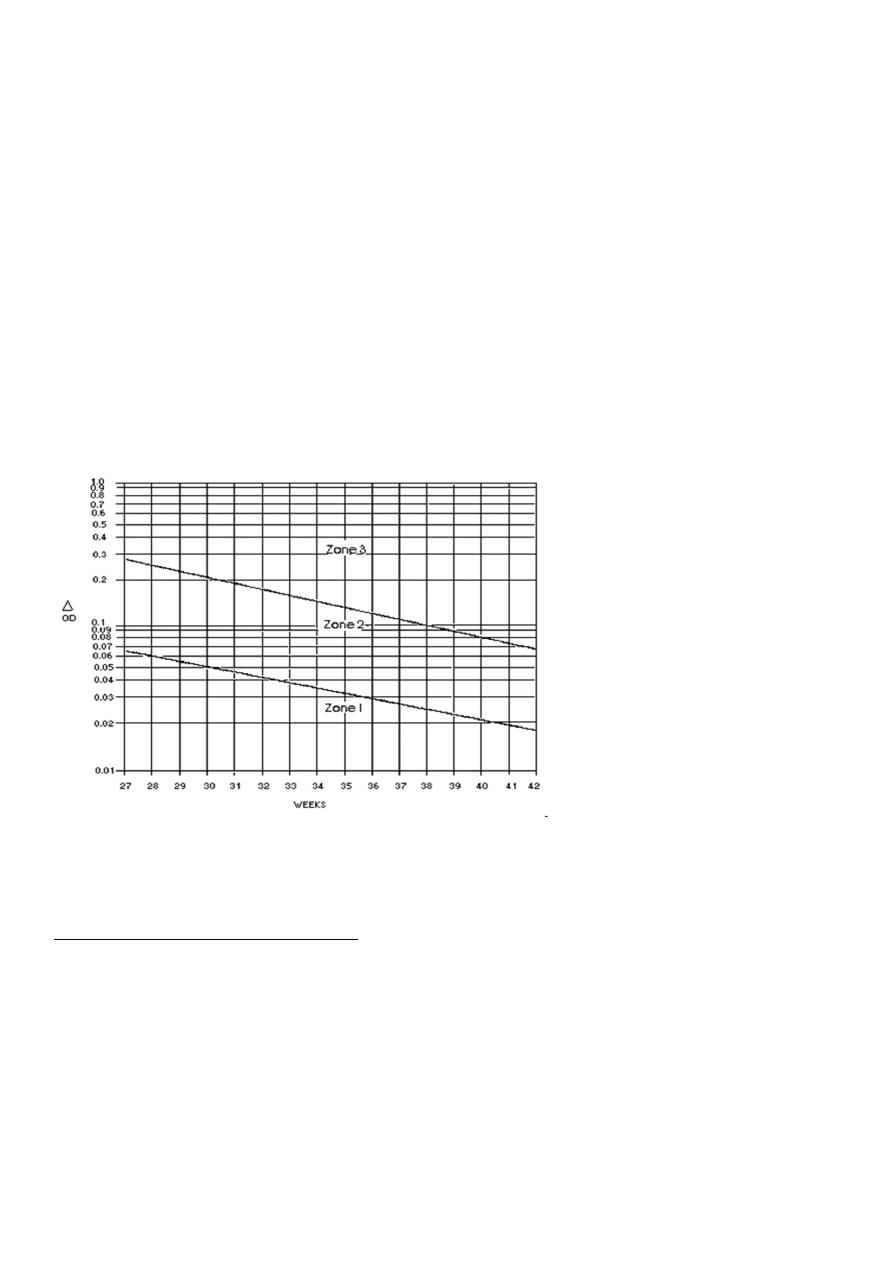
By amniocentesis Liley observed that the delta OD450 normally declined with
advancing gestational age (opposite to the bilirubin concentration) .
The Liley’s chart is divided into 3 zones:
zone 1 :mild or no fetal disease.
zone 2 :moderate disease.
zone 3 :sever disease with the possibility of fetal hydrops with in 7 days .
Amniocentesis repeated every 1-2 weeks depending on the severity ,and intrauterine
fetal blood transfusion or delivery is decided in zone 3 or with a progressive raise in the
upper zone 2 ,depending on the gestation of pregnancy .
Treatment
Fetal intrauterine blood transfusion :
It’s the treatment of significant fetal haemolytic anaemia prior to 34 week gestation .
Transfusion should be undertaken only if the fetal haematocrit is below 30% or in hydrops.
We use blood compatible with the mother and the fetus (O negative) ,fresh ,tested to
exclude infectious agents ,haematocrit of 70%.
There are two types of blood transfusion :
1. Intraperitoneal transfusion .
2. Intravascular transfusion .

6
-Transfusion should be repeated every 3-4 weeks
.
-There is no justification for routine preterm delivery
-The last transfusion should be performed at 34-35 weeks and labour induced at 37-38
weeks.
-Mode of delivery in non anaemic transfused fetus depend on obstetric indication .
Neonatal surveillance :
Infants received intrauterine transfusion
usually do well postnatally .
-Hyperbilirubinaemia can be managed by:
Phototherapy.
Double volume exchange transfusion.
-Neonatal small transfusion for correction of anaemia