
1
4th stage
Obstetrics
Lec-
Dr.Ahmad
3/16/2016
Prolonged Pregnancies
Prolonged Pregnancies ( post-term, post-dates) :
defined as pregnancies persists beyond 42 completed weeks or more than 294 days
from the onset of the last normal menstrual period (LMP).
It occurs in 10% of all pregnancies.
Term is defined as 37-42 weeks gestation.
Dating by LMP alone has a tendency to overestimates the gestational age.
The routine use of early ultrasound to calculate gestational age significantly reduces
incidence of post-term pregnancy.
Ultrasound measurements of crown –rump length of fetus up to about the 14th weeks
and of biparietal diameter of fetal head up to about the 28th weeks give a reliable
indication of duration of gestation.
Risk factors for actual post-term pregnancy include:
1. Primiparity.
2. male gender of the fetus.
3. Obesity .
4. prior post term pregnancy( 30 %).
5. Genetic factors.
Aetiology of prolonged pregnancy
The cause of postdate pregnancy is not clear and it may represent simple biological
variation.
Prolonged pregnancy is common in association with:
2
o an anencephalic fetus.
o placental sulphatase deficiency.
o extrauterine pregnancy.
Risks associated with prolonged pregnancy:
Post term pregnancy per se is not a pathological condition and should not be confused
with post maturity syndrome.
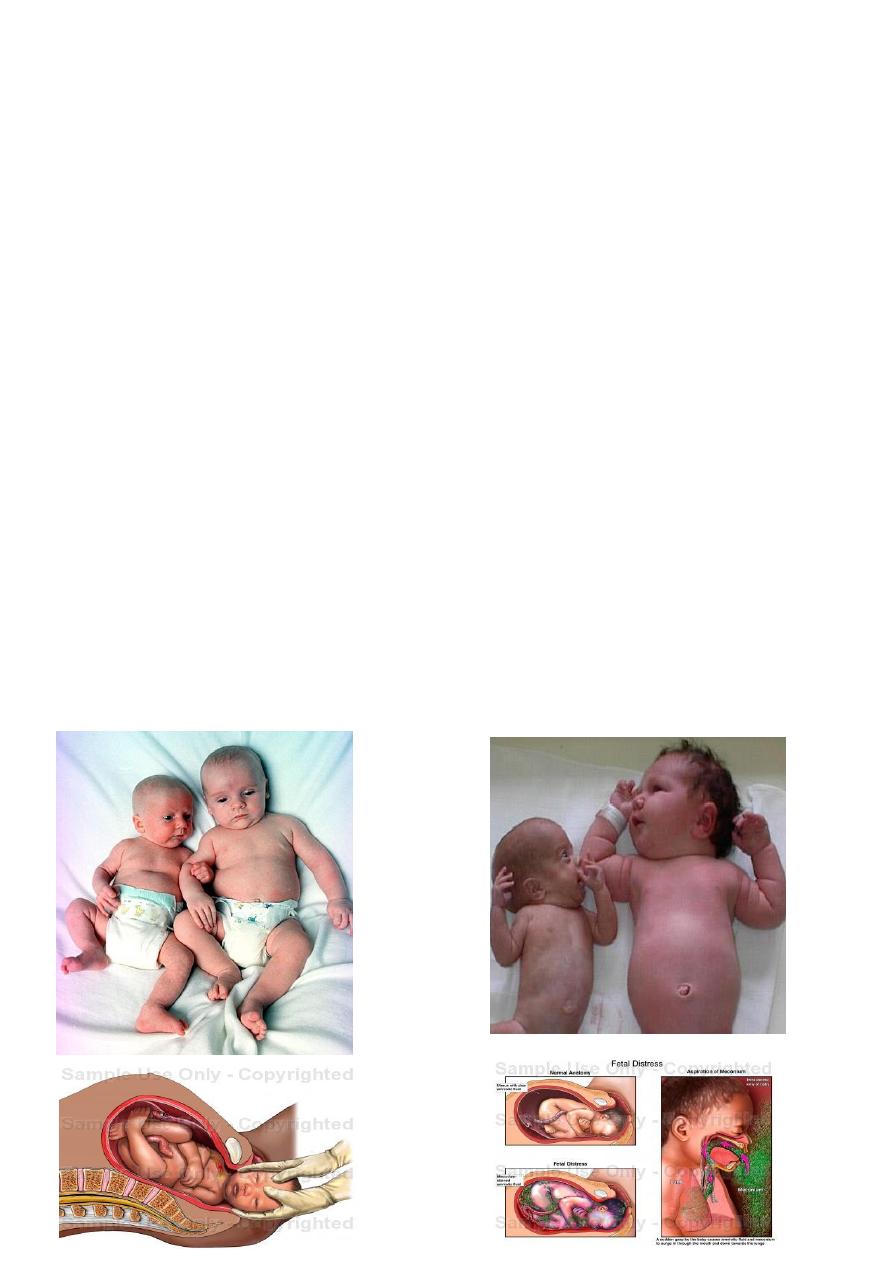
Fetal postmaturity syndrome
occurs in 20-30% of post-term pregnancies.
It is related to the aging and infarction of placenta resulting in placental insufficiency
with impaired oxygen diffusion and decreased transfer of nutrients to fetus.
Fetus is typically has loss of subcutaneous fat, long fingernails, dry, peeling skin, and
abundant hair.
Not every post-term pregnancy is complicated by post-maturity syndrome.
Majority of morbidities and mortality associated with post term pregnancies arises
because of post-maturity.

3
Fetal macrosomia:
1. 70-80% of postdates fetuses not affected by placental insufficiency continuo to grow in
utero, many to point of macrosomia (birth weight greater than 4000grams) this result
in :
abnormal labour
shoulder dystocia
birth trauma
increased incidence of caesarean birth.
2. Increase perinatal mortality(2-3 times higher).
3. Perinatal mortality (2-3 times increased risk of perinatal death).
4. Perinatal morbidity
a. Birth trauma (skull fracture, brachial plexus injuries, intracranial haemorrhage)
b. Shoulder dystocia
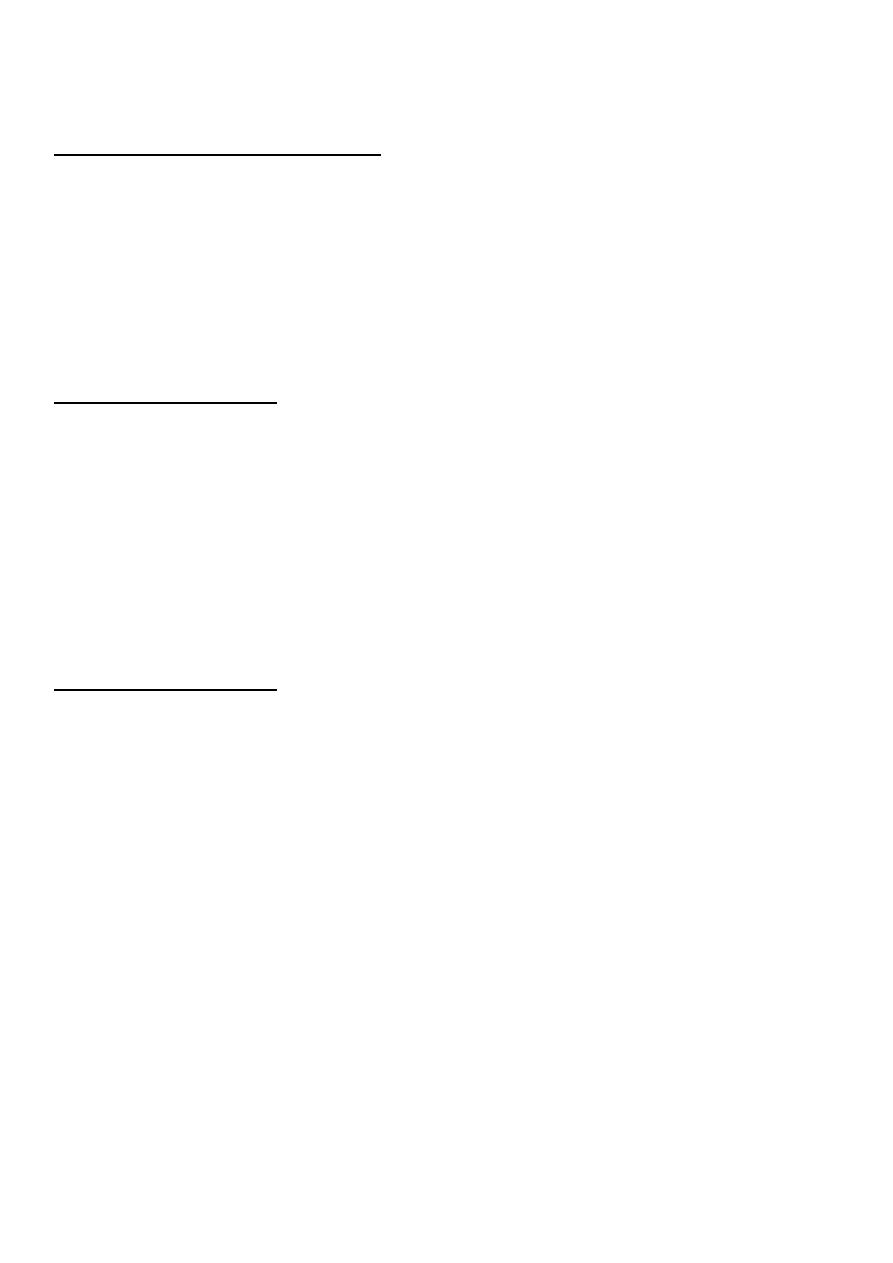
c. meconium aspiration increased Meconium aspiration syndrome refers to
respiratory compromise with tachypnea, cyanosis, and reduced pulmonary
compliance in newborns exposed to meconium in utero and is seen in higher
rates in postterm neonates
d. neonatal seizures.
e. neonatal sepsis.
f. h. respiratory distress syndrome.
g. Cerebral palsy.
Maternal risk:
1. Increased operative delivery.
2. Haemorrhage.
3. Maternal infection.
4. Psychological morbidities anxiety.
Diagnosis
The diagnosis of post-term pregnancy is often difficult. The accurate dating of gestation
is very important.
Gestational age unreliable in calculation of gestational age in women with:
Irregular cycle.
Lactataing women.

4
Recent cessation of birth control pill
Thus, not only the LMP date, but the regularity and length of cycles must be taken
into account when estimating gestational age.
Ultrasound to establish accurate gestational age . Estimation range varies. For example,
crown-rump length (CRL) is ± 3-5 days,
Ultrasound performed at 12-20 weeks of gestation is ±7-10 days,
at 20-30 weeks is ± 2 weeks, and after 30 weeks is ± 3 weeks.
If there is more than one week discrepancy between LMP and ultrasound
finding, then the ultrasound finding should be used to determine expected date
of delivery (EDD).
Women may not know her LMP and has no early first or second trimester ultrasound
we can use some points which can exclude risk of prematurity but can not calculate
gestational age accurately by it:
36 weeks have elapsed since documentation of a positive human chorionic
gonadotropin (+hCG) test finding.
20 weeks of fetal heart tones have been established by a fetoscope or 13 weeks by
A Doppler examination.
Antenatal records for bimanual examination of uterus at an early visit between
8th– 14th weeks an accurate assessment of uterine size can be made.
Management:
Management option depends on:
1. Gestational age.
2. cervical examination findings.
3. estimated fetal weight.
4. past obstetric history.
5. Absence or presence of maternal risk.
6. Factors or evidence of Fetal compromise.
7. Maternal preference and informed consent.

5
Indications of delivery:
Amniotic fluid index <5 cm or maximum pool depth <2 cm
Biophysical profile of 6/ 10 or less
Abnormal fetal heart rate (decelerations
Abnormal umbilical artery Dopplers
Management options are:
1. Elective induction of labour.
2. Expectant management with/ without antepartum testing
Simple monitoring with Non stress test (NST) cardiotocography (CTG) and liquor
assessment.
Assessment of post-dates pregnancy:
Many different tests of fetal well-being are performed for assessment of post-term fetus.
These include:
Cardiotocography (CTG).
Ultrasonographic testing.
Amniotic fluid index.
Biophysical profiles.
Umbilical artery Doppler waveform analyses.
Expectant management
it consists of:
1. daily fetal kick count
2. non stress test (NST) twice/ week to 42 weeks.
3. ultrasound to assess amniotic fluid volume twice/ week until 42 weeks.
4. if NST abnormal or amount of liquor is abnormal induce immediately.
5. induce at 42 weeks if NST is normal amniotic fluid volume is normal.
6. Take history examination and investigation (NST,CTG,amniotic fluid assessment)
6
Gestaional age :
40
0/7
- 40
6/7
weeks gestation:
A. In cases with Healthy , uncomplicated pregnancy, fetal growth and amount of liquor
was normal: Wait spontaneous labour and no need to serial investigations.
B. Presence of maternal risk factor or evidence of fetal compromise: Delivered by
Induction of labour if there is no obstetrical contraindication
41 weeks gestation:
After 41 weeks’ gestation, if the dates are certain, women should be offered elective
delivery.
routine induction at 41 weeks of gestation does not increase the cesarean delivery
rate and may decrease it without negatively affecting perinatal morbidity or
mortality. In fact, both the woman and the neonate benefit from a policy of routine
induction of labor in well-dated, low-risk pregnancies at 41 weeks' gestation.
42 weeks gestation:
delivery
there are multiple reasons not to allow a pregnancy to progress beyond 42 weeks.
Obstetricians re unable to offer complete reassurance to expectant mother who
continues to awaite spontaneous onset of labour.
Intrapartum management:
Continuous electronic fetal monitoring must be employed during induction of labour.
Fetal membranes should be ruptured as early as possible to see color of amniotic
fluid.casearean section is indicated for fetal distress and should not to be delayed
because of decreased capacity of postterm fetus to tolerate asphyxia and increased
risk of meconium aspiration.
If meconium is present neonatiologist should be present at time of delivery.
Be prepared for shoulder dystocia.

7
Prevention :
Stripping or sweeping of the fetal membranes refers to digital separation of the
membrane.
Unprotected sexual intercourse.