
1
Forth stage
Medicine
Lec-6
د.فاخر
1/1/6102
Diseases of the parathyroid glands
and
abnormalities in calcium metabolism
Parathyroid glands
Four parathyroid glands located behind the thyroid lobes secrete parathyroid hormone
(PTH) .
PTH is secreted from the chief cells of the parathyroid glands in response to a fall in plasma
ionized calcium concentration.
Function of parathyroid glands
PTH has a direct effect that promotes reabsorption of calcium from renal tubules and
resorption of calcium from bone.
It indirectly increases calcium absorption from food by enhancing renal conversion of
25(OH) vitamin D to 1,25(OH)2 vitamin D; the active vitamin D metabolite.
In combination, these effects result in a rise in serum calcium.
calcium metabolism
Around 99% of total body calcium is in bone, which is in a dynamic equilibrium with serum
calcium through a process of resorption and deposition.
Calcium in serum exists as:
50% ionized (Ca2+)
10% non ionized or complexed with organic acids
40% protein bound, mainly to albumin.
Most labs measure total calcium in serum, which should be corrected if the serum albumin
is low, by adjusting the value of calcium upward by 0.1 mmol/L (0.4 mg/dl) for each 5 gm/L
reduction in albumin below 40 gm/L.

2
Hypercalcaemia
Hypercalcaemia is one of the most common biochemical abnormalities, commonly
detected in asymptomatic patients. If symptoms are present, they may include:
Polyuria, polydypsia and renal colic
Anorexia, nausea, dyspepsia, constipation and peptic ulceration
Lethargy, drowsiness, impaired cognition and depression
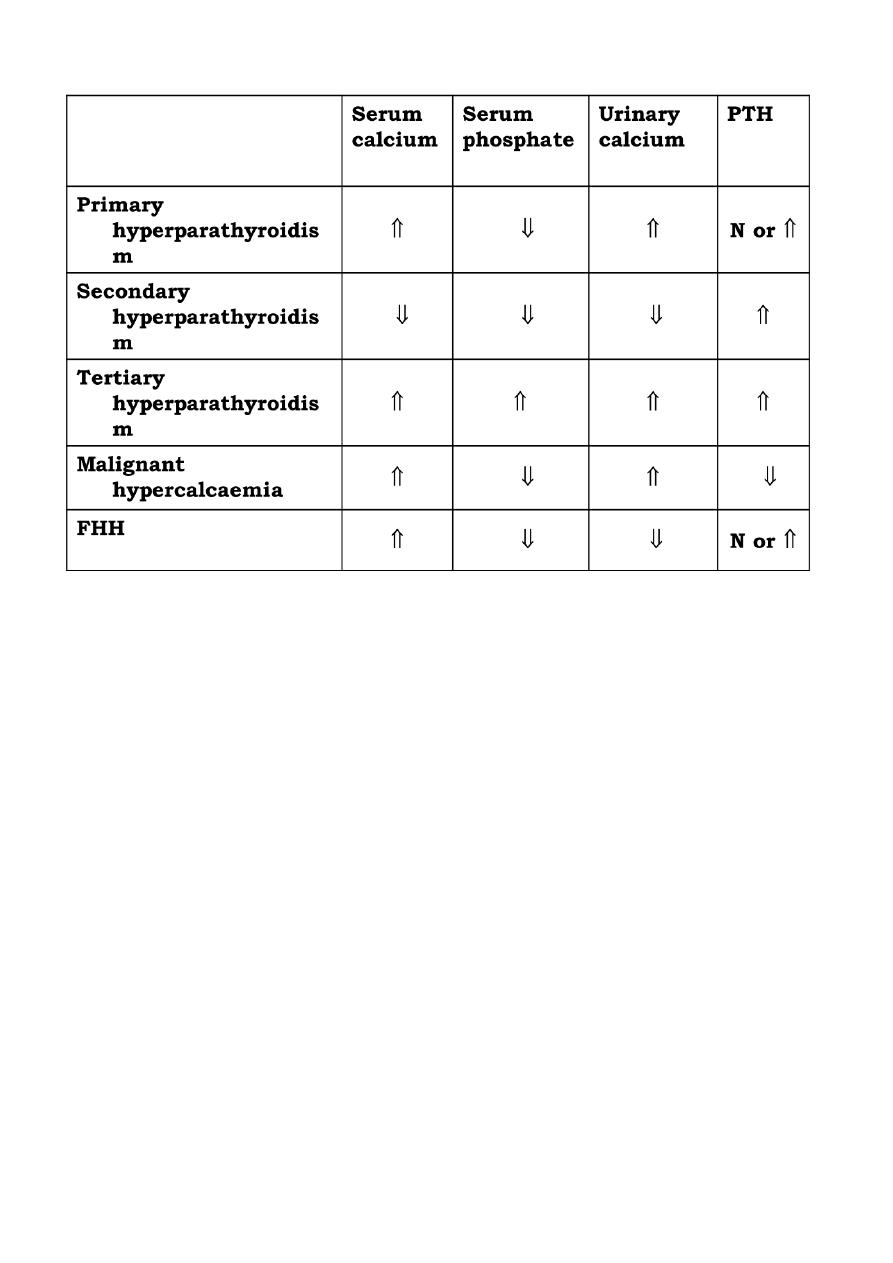
Causes of hypercalcaemia
1-Hyperparathyroidism (primary or tertiary)
2-Hypercalcaemia of malignancy
3-Familial hypocalciuric hypercalcaemia (FHH)
4-Elevated 1,25(OH)2 vitamin D (hypervitaminosis D and sarcoidosis)
5-Drugs (thiazide and lithium)
6-Other endocrine disorders (thyrotoxicosis and adrenal insufficiency)
7-Paget's disease of bone.
Hyperparathyroidism
There are three categories of hyperparathyroidism: primary, secondary and tertiary.
Primary hyperparathyroidism is characterized by autonomous secretion of PTH; usually
from parathyroid adenoma (90%)
Secondary hyperparathyroidism represents a compensatory increase in PTH secretion from
hyperplasia of all parathyroid tissue in response to prolonged hypocalcaemia caused by
diseases like chronic renal failure, malabsorption or osteomalacia.
In a very small proportion of cases of secondary hyperparathyroidism, continuous
stimulation of the parathyroids results in adenoma formation and autonomous PTH
secretion with resultant hypercalcaemia (tertiary hyperparathyroidism).
Primary hyperparathyroidism
It is 2 – 3 times more common in females
90% of patients are more than 50 years of age.

3
The disease also occurs in two autosomal dominant disorders called multiple endocrine
neoplasia syndromes (MEN 1 and 2).
MEN1 is characterized by primary hyperparathyroidism, pituitary tumour and pancreatic
neuro-endocrine tumour (e.g. insulinoma or gastrinoma).
MEN2 is the association of primary hyperparathyroidism with medullary carcinoma of the
thyroid and pheochromocytoma.
Clinical features of primary hyperparathyroidism
About 50% of patients are asymptomatic, and discovered accidentally after finding
hypercalcaemia on routine testing.
Symptomatic patients:
present insidiously with chronic symptoms of hypercalcaemia, or
manifest late with renal or bone disease (bones, stones and abdominal groans).
Hyperparathyroid bone disease:
Now rare due to early diagnosis and treatment
Caused by prolonged sustained effect of PTH on bone, resulting in increased osteoclastic
activity and extensive bone remodeling with associated osteoblastic activity and fibrous
tissue repair (osteitis fibrosa).
The patient may present with bone pain and tenderness, fracture and deformity.
Chondrocalcinosis is due to deposition of calcium pyrophosphate crystals within articular
cartilage (typically the menisci of the knees), with consequent degenerative arthritis and
episodes of pseudogout.
Renal disease:
Nephrocalcinosis: calcification of the renal parenchyma.
Renal calculi are other important manifestation of primary hyperparathyroidism. 5% of first
stone formers and 15% of recurrent stone formers have primary hyperparathyroidism.
Hypertension is more common in hyperparathyroidism.
Parathyroid tumours are almost never palpable.

4
Primary hyperparathyroidism
(Radiological features)
Characteristic changes on plane X ray are:
Demineralization, subperiosteal erosion and resorption of terminal phalanges
Pepper pot appearance of the lateral X ray of the skull
Scattered opacities within the renal outline (nephrocalcinosis)
renal stones
Soft tissue calcification affecting arterial walls, hands or cornea
Chondrocalcinosis
Very early changes of reduced bone mineral density is only evident on DEXA (deep energy X
ray absorptiometry) scanning
Hypercalcaemia of malignant disease
Common causes are lung, breast and renal carcinoma, and multiple myeloma
Hypercalcaemia can occur as a result of direct bone involvement or ectopic tumour
production of a paratharmone – related peptide (PTHrP).
The duration of symptoms of hypercalcaemia is characteristically short and renal stone
formation is consequently rare.
The main problem is dehydration due to the diuretic effect of elevated urinary calcium
Familial hypocalciuric hypercalcaemia (FHH)
A rare autosomal dominant disorder, characterized by reduced ability of the parathyroid
glands to sense ionized calcium
As a result, higher than normal calcium level is required to suppress PTH secretion.
The minor elevation of PTH may result in a misdiagnosis of hyperparathyroidism and
unnecessary surgery.
The presence of family history of hypercalcaemia and low urinary calcium excretion should
help to make the proper diagnosis.
5
Investigations of patients with hypercalcaemia
Localization of parathyroid tumours
If primary hyperparathyroidism is confirmed biochemically, pre-operative localization of the
adenoma is not necessary, as surgeons are able to locate the adenoma in 90% of cases.
However, there is a trend toward performing 99mTc-sestamibi scanning prior to surgery.
Unsuccessful surgical exploration can be helped by the same scanning or by CT or selective
neck vein sampling for PTH.
Management of hypercalcaemia
Severe hypercalcaemia associated with malignancy or other causes is treated as an
emergency with normal saline hydration (4 – 6 litres).
Bisphosphanates (like pamidronate 90 mg I.V. over 4 hours) cause a fall which is maximum
after 2 – 3 days and sustained for weeks. This can be followed by oral bisphosphanate.
In a very ill patient, normal saline hydration can be can be supplemented with frusemide,
corticosteroid (prednisolone 40 mg / day), calcitonin, or dialysis.

6
Management of primary hyperparathyroidism
Surgical excision of a solitary parathyroid adenoma or debulking of hyperplastic glands is
the long term treatment of first choice.
Post-operative hypocalcaemia can occur transiently after surgery, until suppressed
parathyroid tissues recover.
Indication for surgery:
patients younger than 50 years
very high serum calcium (more than 3 mmol/L)
documented complications, such as renal stones, renal impairment, osteopenia or peptic
ulceration.
When surgery is not indicated, patients can receive:
the bisphosphanate alendronte 10 mg daily as long term therapy to prevent osteoporosis.
calcimimetics (like cinocalcet) are recently introduced drugs which can reduce PTH
secretion by increasing sensitivity of the parathyroids to ionized calcium.
Hypocalcaemia
Before diagnosing hypocalcaemia, the reported serum calcium should be corrected for
albumin. Hypoalbuminaemia reduces total serum calcium without affecting the ionized
calcium; the biologically active fraction.
Conversely, symptoms of hypocalcaemia may occur in patients with alkalosis (commonly
due to hyperventilation or repeated vomiting) in the presence of normal serum calcium,
because alkalotic serum increases albumin binding and reduces ionized calcium.
Causes of hypocalcaemia
True hypocalcaemia occurs in the following conditions:
Vitamin D deficiency
Chronic renal failure
Hypoparathyroidism
Pseudohypoparathyroidism
Acute pancreatitis
Hypomagnesaemia

7
Vitamin D deficiency can be nutritional or caused by lack of sun exposure or malabsorption,
where hypocalcaemia is associated with hypophosphataemia, raised alkaline phosphatase
and secondary hyperparathyroidism.
Chronic renal failure is an important cause. Hypocalcaemia is accompanied by
hyperphosphataemia (because of phosphate retention), high alkaline phosphatase and
secondary hyperparathyroidism.
Hypomagnesaemia reduces PTH secretion and induces tissue resistance to its effect.
Hypoparathyroidism
In hypoparathyroidism, low serum calcium is associated with high phosphate and low PTH.
Post-thyroidectomy hypoparathyroidism: The most common cause of hypoparathyroidism
is damage to the parathyroid glands (or their blood supply) during thyroid surgery
(transient in 10% of cases and permanent in 1% of them).
Primary hypoparathyroidism: congenital or inherited.
Pseudohypoparathyroidism have tissue resistance to the effect of PTH, consequently PTH is
markedly elevated. The disease is hereditary, and characterized by a unique phenotype of
obesity, short stature, round face and short 4th metacarpals and metatarsals.
Pseudo-pseudohypoparathyroidism is used to describe patients with these clinical features
in whom serum calcium and PTH are normal.
Clinical features of hypocalcaemia
Tetany is the clinical syndrome of increased excitability of peripheral nerves caused by low
ionized calcium. In the absence of alkalosis, tetany occurs in adults when serum calcium
below 2 mmol/L.
Tetany is manifested by:
Tingling in the hands, feet and around the mouth.
Carpal spasm
Pedal spasm
Strider
Convulsions
8
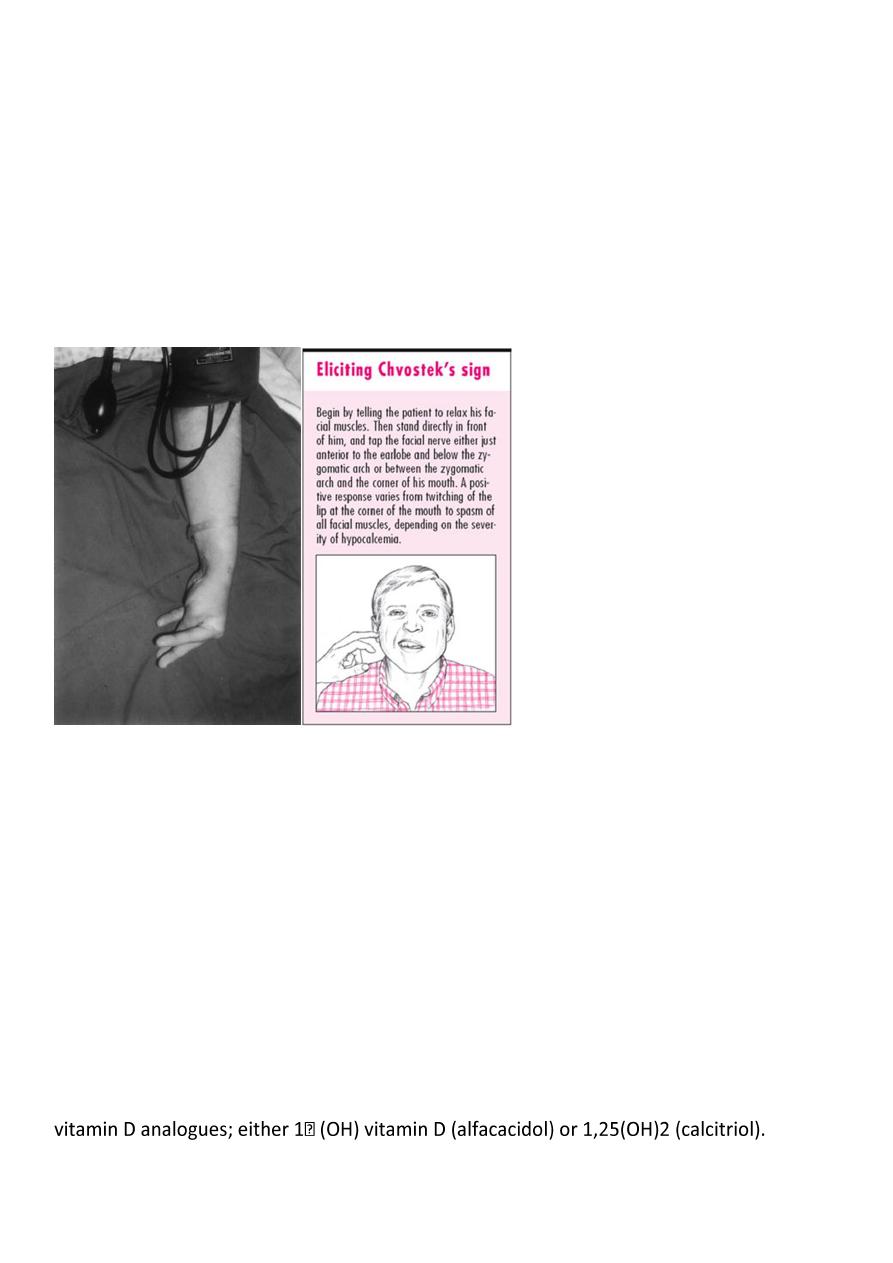
Clinical features of hypocalcaemia
Latent tetany may be present when signs of overt tetany are lacking
Trousseau's sign; inflation of a sphygmomanometer cuff on the upper arm to more than the
systolic blood pressure is followed by carpal spasm within 3 minutes.
Chvostek's sign is less specific; tapping over facial nerve branches as they emerge from the
parotid gland produces tingling of facial muscles
Latent tetany
Because of associated hyperphosphataemia, patients with hypoparathyroidism may
develop calcification of the basal ganglia, grand mal seizure, psychosis and cataract.
Management of hypocalcaemia
If tetany is caused by alkalosis with normal serum calcium, the condition can be rapidly
controlled by rebreathing expired air in a paper bag (to increase PaCO2).
Hypocalcaemia can be immediately corrected by slow IV injection of 20 ml of 10% solution
of calcium gluconate. An additional IM injection of 10 ml may also be given for a more
prolonged effect.
IV magnesium may be required to correct associated hypomagnesaemia.
Treatment of Hypoparathyroidism
Hypoparathyroidism and pseudohypoparathyroidism are treated with oral calcium salts and
The therapy needs careful monitoring to avoid hypercalcaemia and its consequences.