1
Forth stage
Medicine
Lec-4
د.فاخر
1/1/6102
HYPOTHYROIDISM
Objectives
o What causes hypothyroidism?
o What are the clinical signs?
o How is it diagnosed?
o Can it be treated?
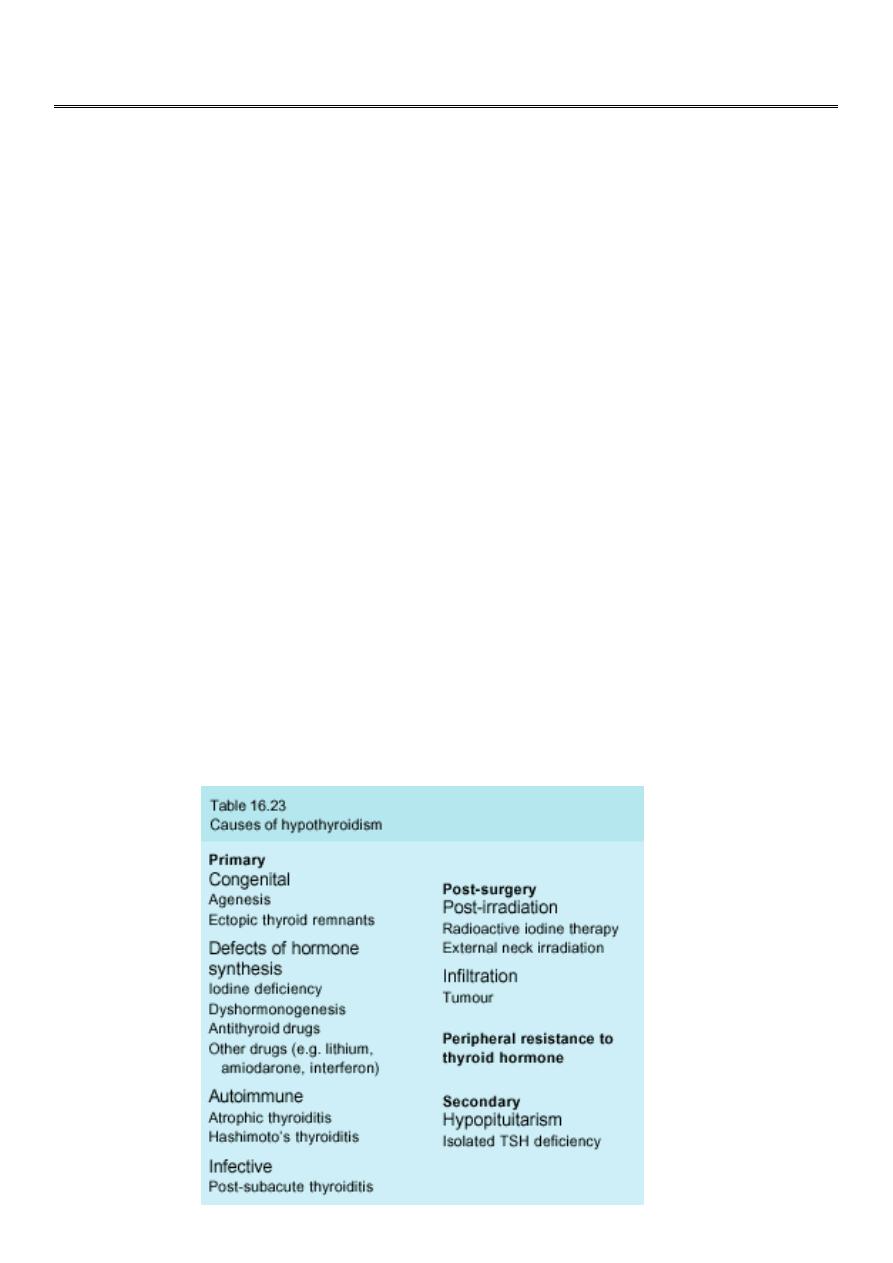
Hypothyroidism
Failure of the thyroid gland to produce adequate amounts of hormone.
1-Primary.
2-Secondary – decreased secretion of TSH from pituitary.
Thyroid gland normally releases thyroxine (T4) daily and small amounts of T3.
T4 half-life 7-10 days.
T4 (prohormone) converted to T3 in peripheral tissues.
Generally, thyroid disease is more common in females.
The prevalence of primary hypothyroidism is 1:100, The female:male ratio is
approximately 6:1.
2
HASHIMOTO'S THYROIDITIS
The nomenclature of autoimmune hypothyroidism. Some authorities reserve the term
'Hashimoto's thyroiditis' for patients with positive thyroid peroxidase autoantibodies and a
firm goitre who may be hypothyroid, and use the term 'spontaneous atrophic
hypothyroidism' for hypothyroid patients without a goitre in whom TSH receptor-blocking
antibodies may be more important.
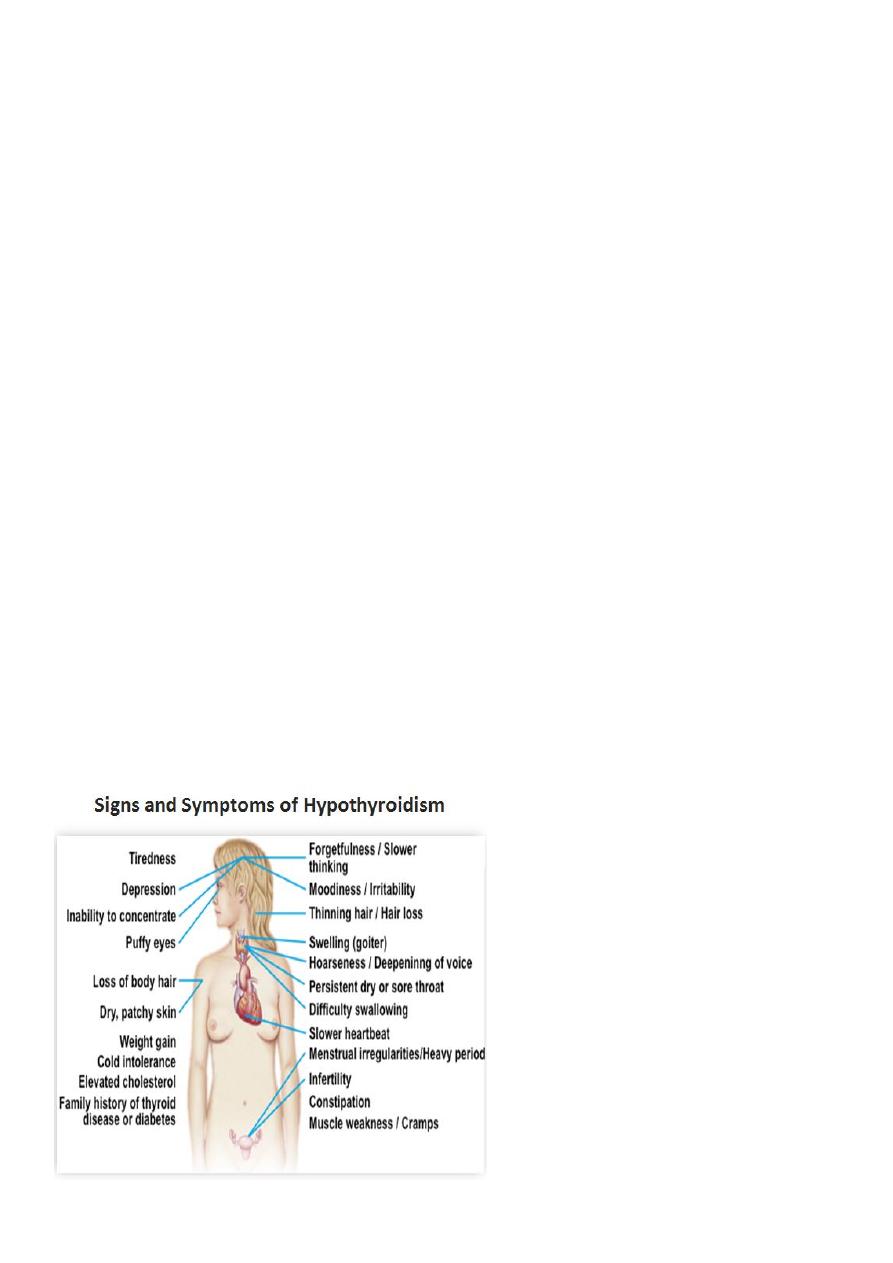
Clinical features
A consequence of prolonged hypothyroidism is the infiltration of many body tissues by the
mucopolysaccharides, hyaluronic acid and chondroitin sulphate, resulting in
1-a low-pitched voice.
2- poor hearing.
3- slurred speech due to a large tongue.
4- compression of the median nerve at the wrist (carpal tunnel syndrome).
5- Infiltration of the dermis gives rise to non-pitting oedema (i.e. myxoedema) which is
most marked in the skin of the hands, feet.
6-periorbital puffiness is often striking and, when combined with facial pallor due to
vasoconstriction and anaemia .
7- a lemon-yellow skin due to carotenaemia.
8-tiredness, weight gain.
3
INVESTIGATION OF PRIMARY HYPOTHYROIDISM
1-Serum TSH is the investigation of choice; a high TSH level confirms primary
hypothyroidism. A low total or free serum T
4
level confirms the hypothyroid state. 2-
Thyroid antibodies may be present.
3-anaemia, which is usually normochromic and normocytic in type but may be macrocytic
(sometimes this is due to associated pernicious anaemia) or microcytic (in women, due to
menorrhagia).
4-increased creatine kinase levels.
5- hypercholesterolaemia.
6-hyponatraemia due to an increase in ADH and impaired free water clearance.
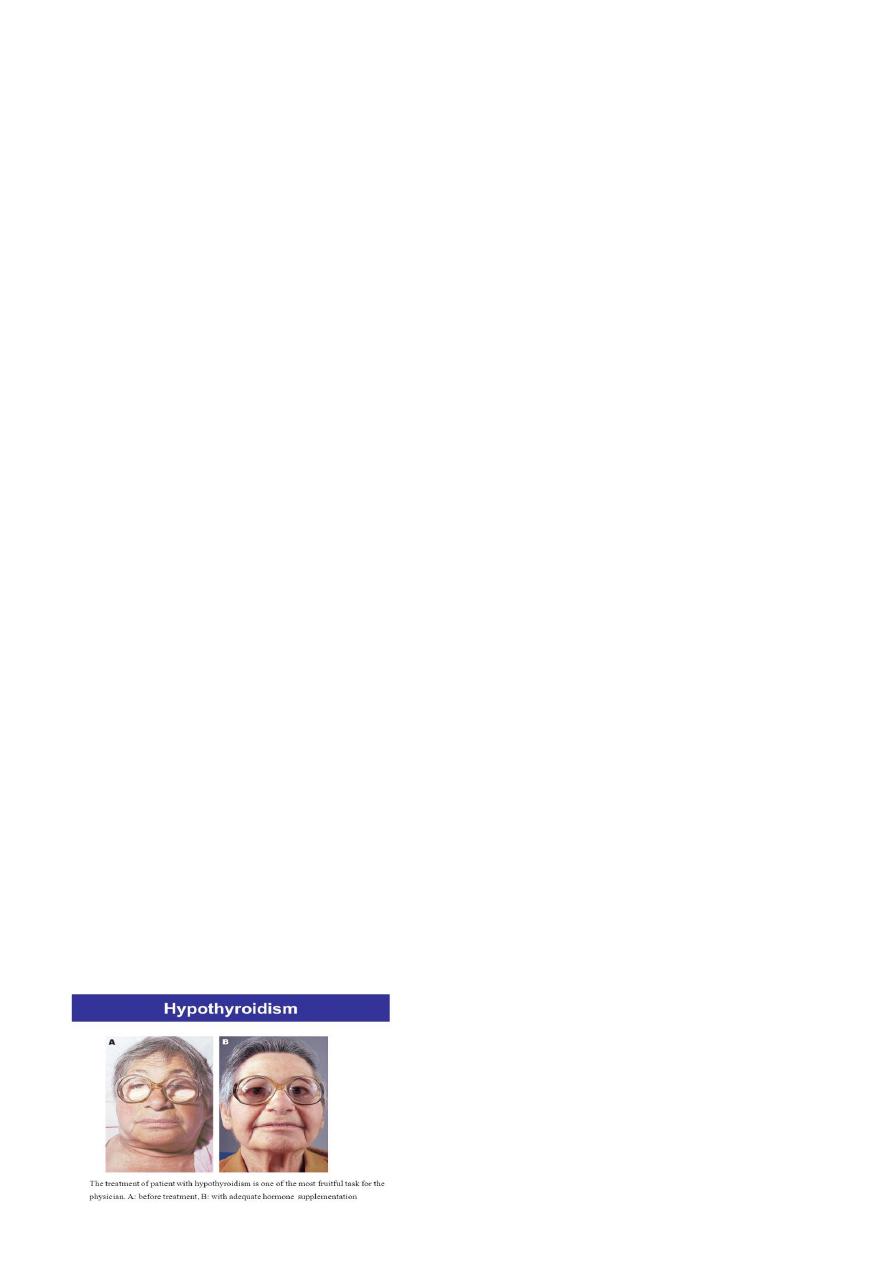
Management
Hypothyroidism should be treated with thyroxin it is available in 25 ,50, 100microgram
tablests the dose should be started50 mg then should be increased to 100mg after 3wks
&after another 3wks should raised to 150 mg &should be given single dose.
If the patient had ischemic heart disease or elderaly the dose should be reduse to 25 mg
daily . Serum TSH should be measured 8 weeks after starting the treatment to check
whether the dose needs to be increased and should be measured annually in patients on
established treatment to ensure continuing compliance.
Myxoedema coma
This is a rare presentation of hypothyroidism in which there is a depressed level of
consciousness, usually in an elderly patient who appears myxoedematous. Body
temperature may be as low as 25°C, convulsions are not uncommon and cerebrospinal fluid
(CSF) pressure and protein content are raised. The mortality rate is 50% and survival
depends upon early recognition and treatment .
Myxoedema coma is a medical emergency and treatment must begin before biochemical
confirmation of the diagnosis. Thyroxine is not usually available forparenteral use so
triiodothyronine is given as an intravenous bolus of 20 μg followed by 20 μg 8-hourly until
there is sustained clinical improvement.