
1
4th stage
باطنية
Lec-8
د.ظاهر
6/12/2015
Pulmonary Embolism
Introduction to Pulmonary embolus
Pulmonary embolism is a life-threatening condition that
occurs when a clot of blood or other material blocks an artery
in your lungs.
This is an extremely common and highly lethal condition that
is a leading cause of death in all age groups.
One of the most prevalent disease processes responsible for
in-patient mortality (30%)
Overlooked diagnosis.
Pulmonary Embolism back ground
Prompt diagnosis and treatment can dramatically reduce the
mortality and morbidity rate.
Majority of the cases are unrecognised clinically.
One third of the patients who survive an initial PE die of a
future embolic episode.
Many patients who die of PE have not had any diagnostic
workup nor have they received any prophylaxis for the disease.
In most cases the CLINICIANS have not even considered the
diagnosis of PE.
Pathophysiology of pulmonary embolism
It is often a fatal complication of underlying venous
thrombosis.
Normally microthrombi (RBC,Platelets and Fibrin) are formed
and lysed with in the venous circulatory system.
Under pathological condition these microthrombi may escape
and propagate and will block the pulmonary blood vessels
causing PE

2
Predisposing factors
Patients on prolonged bed rest for > a week. Prolonged
immobilization.
Patients in ICU, CCU.
After bypass surgery or any surgery.
All trimesters of pregnancy and puerperium.
Older patients – Age no bar still.
Predisposing factors
1-CCF.
2-Fractures.
3-Oral Contraceptives.
4-Drug abuse.
5-MI.
6-Obesity.
7-Old age.
8-Malignancy.
9-Catheter
Patient presentation
Haemoptysis, Dyspnoea and Chest pain –
o (Virchows Triad)
Back pain, Abdominal pain, wheezing, SOB, Seizures,
Productive cough, Hiccoughs, Fever……
Can be asymptomatic.
3
Diagnostic Modalities in PE
ECG***
D Dimer assay test
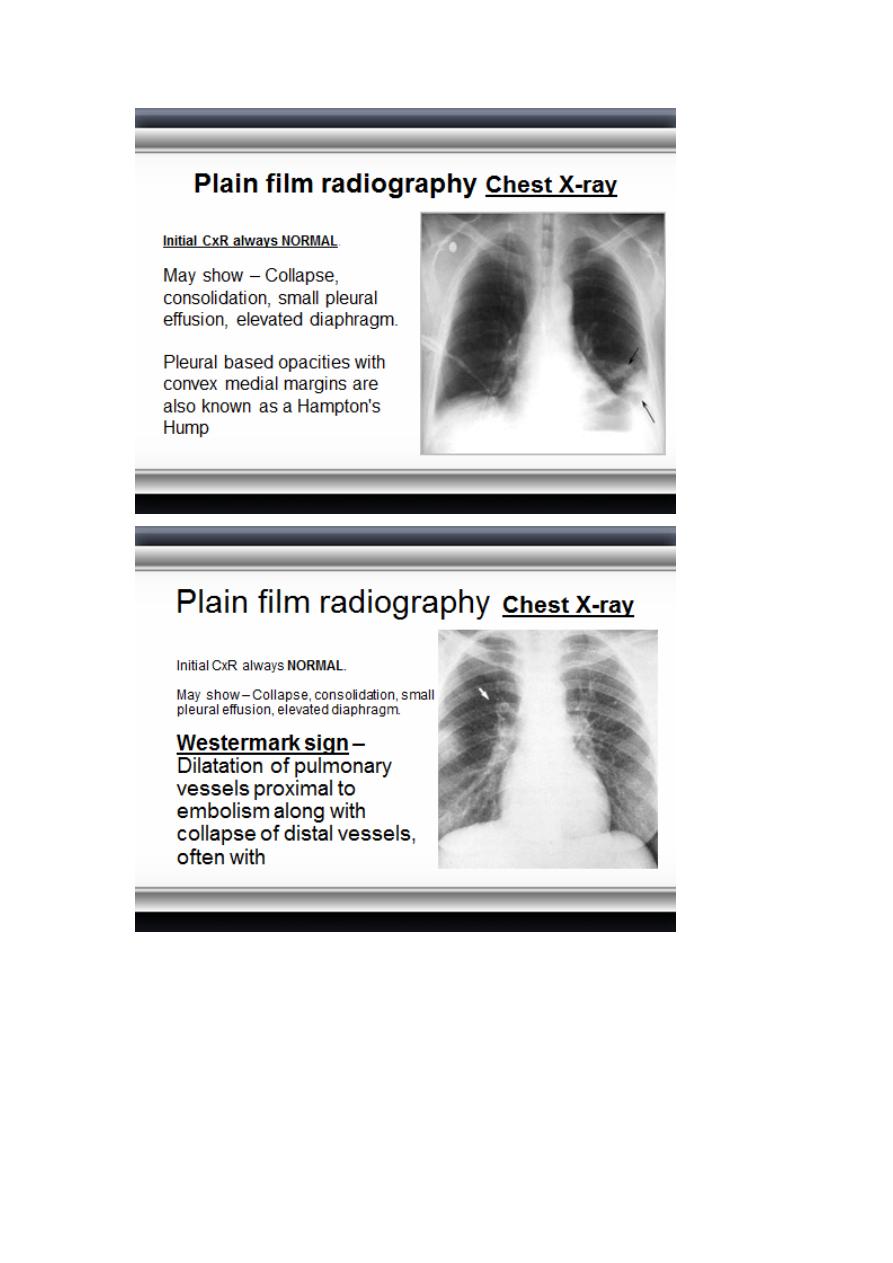
Plain film radiography
Radionuclide imaging (VQ Scan)
CT Angiography
Pulmonary angiography
Echocardiography Ultrasound(DVT)***
MRI & MRA0
D-Dimer Assays
Gainfully employed to select patients for further radiological
imaging.
It is a cross linked fibrin degradation product and a plasma
marker of fibrin lysis.
Serum level less than 500ng/L excludes PE with 90-95%
accuracy.
Unfortunately a positive test is non specific (specificity only 25
– 67% and occurs in about 40 – 69% of the patients
4
5
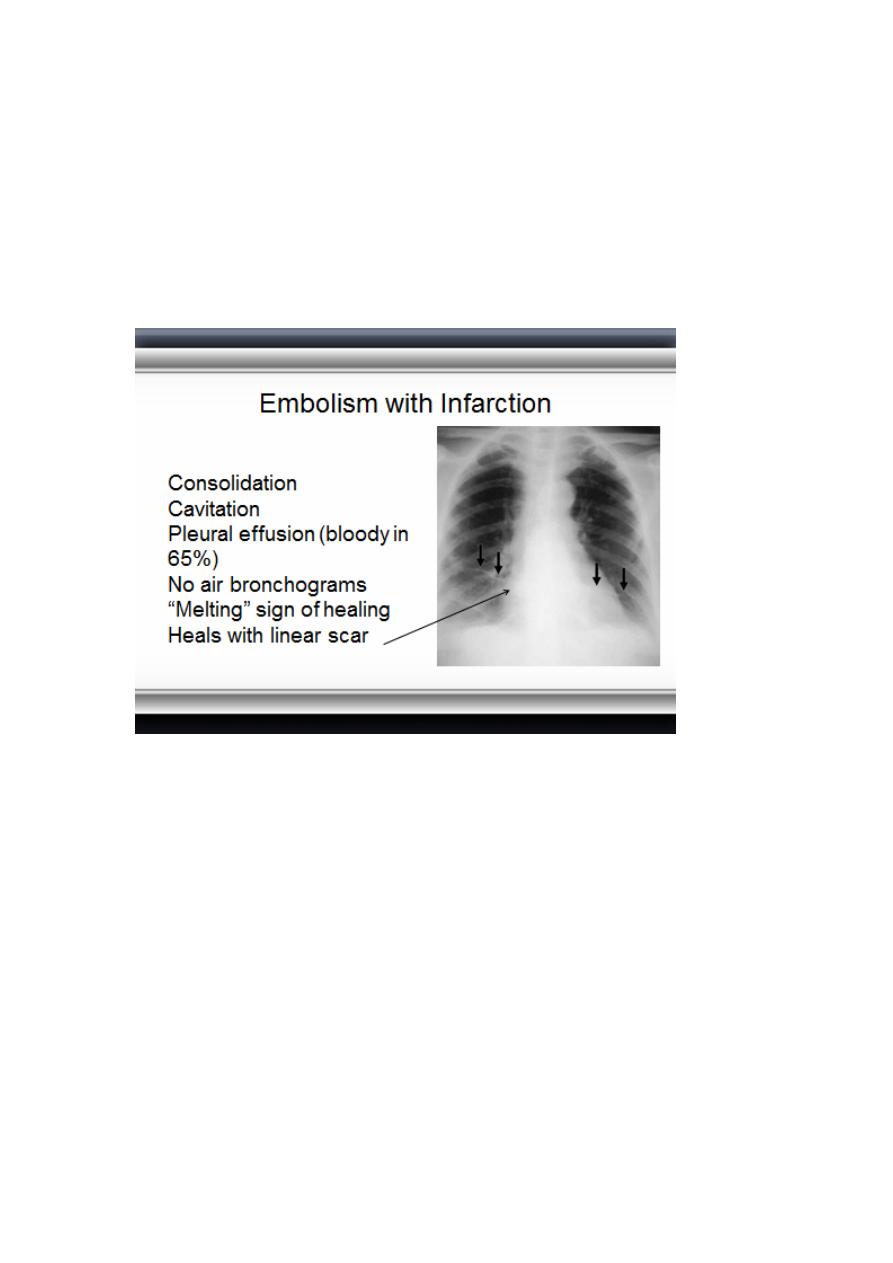
Embolism without Infarction
Most PEs (90%)
Frequently normal chest x-ray
Pleural effusion
Westermark’s sign
“Knuckle” sign abrupt tapering of an occluded vessel distally
Elevated hemidiaphragm
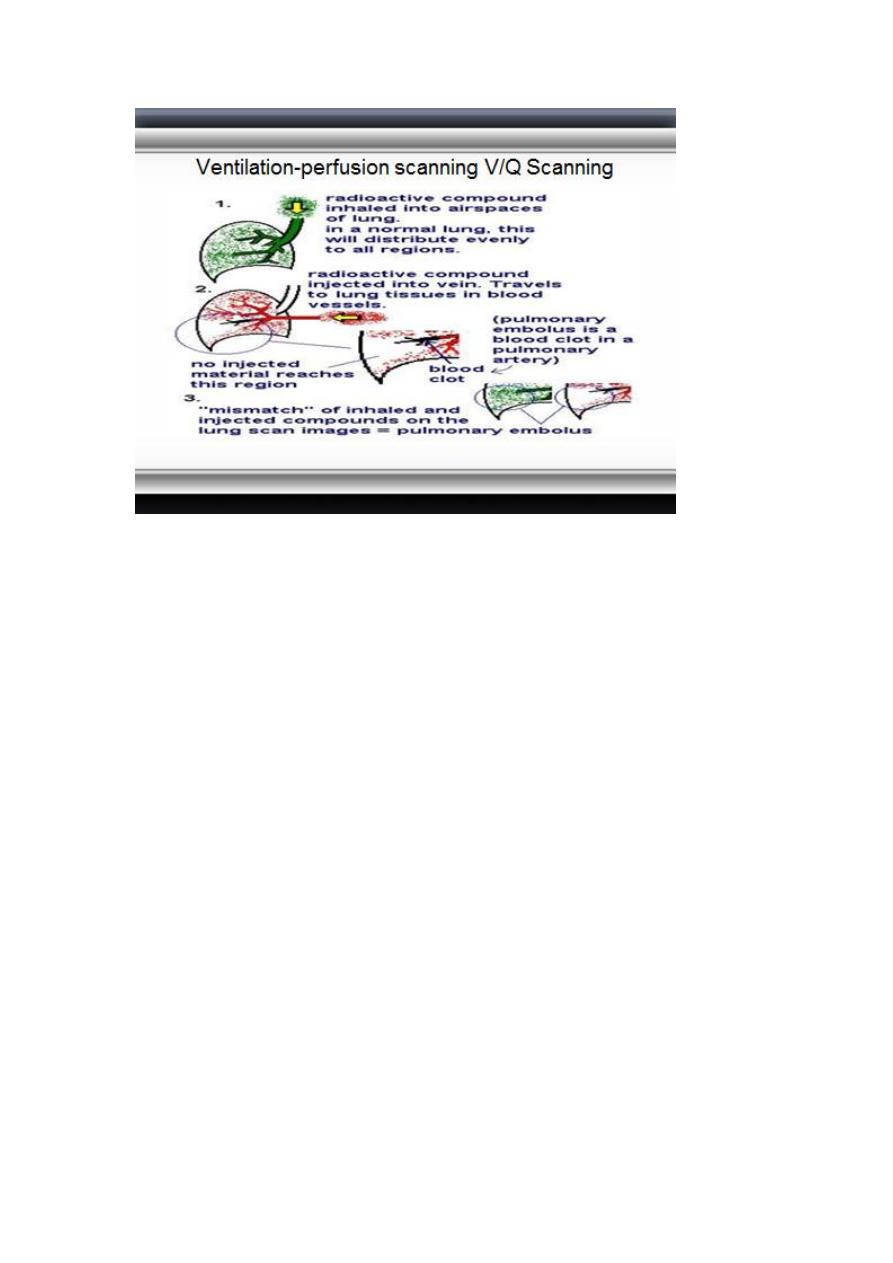
Ventilation-perfusion scanning V/Q Scanning
Single most important diagnostic modality for detecting PE.
Always indicated when PE is suspected and there is no other
diagnosis.
1 in every 25 pts sent home after a normal V/Q scan actually
has a PE that has been MISSED
6
Ventilation-perfusion scanning V/Q Scanning
Radiological procedure which is often used to confirm or
exclude the diagnosis of pulmonary embolism. It may also be
used to monitor treatment.
The ventilation part of the scan is the inhalation of Krypton
81m, which has a short half life and is a pure gamma emitter.
Ventilation is assessed under a gamma camera.
Ventilation-perfusion scanning V/Q Scanning
The perfusion part of the scan is achieved by injecting the
patient with technetium 99m, which is coupled with macro
aggregated albumin (MAA). This molecule has a diameter of
30 to 50 micrometres, and thus sticks in the pulmonary
capillaries.
An embolus shows up as a cold area when the patient is placed
under a gamma camera. The MAA has a half life of about 10
hours
7
Spiral CT
HRCT (spiral) CT with CT angiography is a promising
technique.
CT unlikely to miss any lesion.
CT has better sensitivity, specificity and can be used directly to
screen for PE.
CT can be used to follow up “non diagnostic V/Q scans.
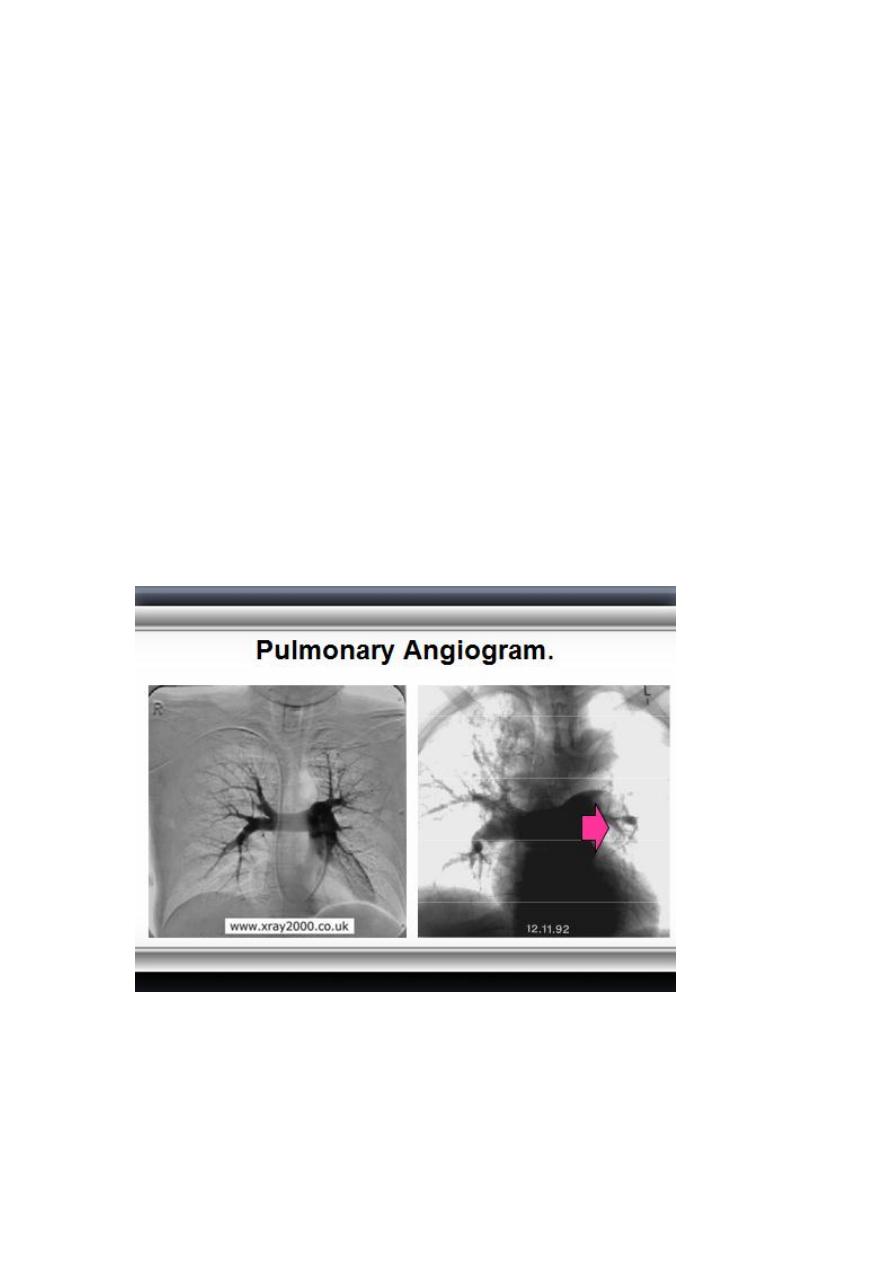
Pulmonary Angiogram
Positive angiogram provides 100% certainty that an obstruction
exists in the pulmonary artery.
Negative angiogram provides > 90% certainty in the exclusion
of PE.
Catherterisation of the Subclavian vein – Superior vena cava
– right atrium – right ventricle – main pulmonary artery

8
.
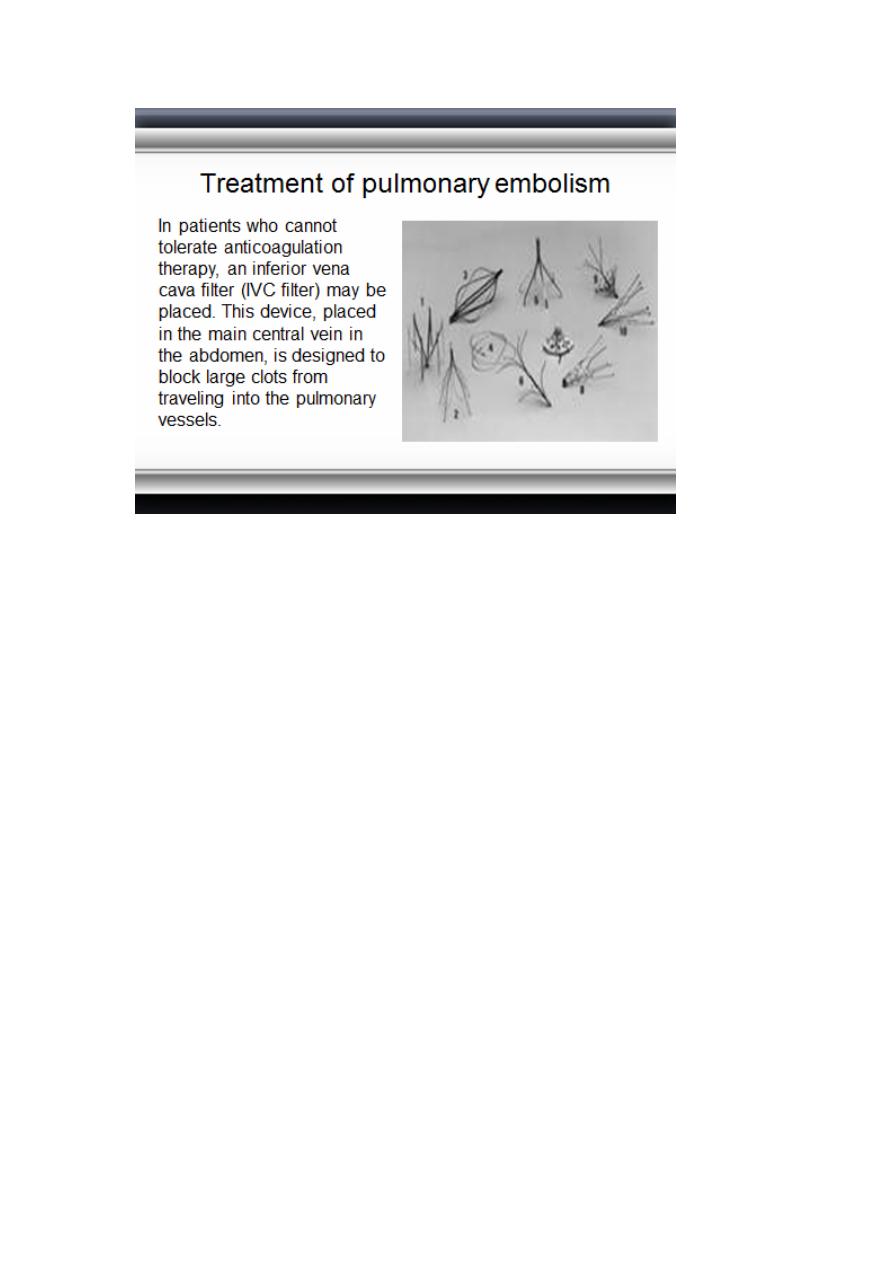
Treatment of pulmonary embolism
Emergency treatment and hospitalization are necessary. In
cases of severe, life-threatening pulmonary embolism,
definitive treatment consists of dissolving the clot with
thrombolytic therapy. Anticoagulant therapy prevents the
formation of more clots and allows the body to re-absorb the
existing clots faster.
Treatment of pulmonary embolism
Thrombolytic therapy (clot-dissolving medication) includes
streptokinase, urokinase, or t-PA.
Anticoagulation therapy (clot-preventing medication) consists
of heparin by
infusion initially, then oral warfarin
(Coumadin).
low-molecular weight heparin is
often substituted for intravenous heparin in many
circumstances
9