Acute pancreatitis
Definition:An acute inflammatory process of the pancreas with variable involvement of regional tissues and remote organ systems.
Pathogenesis
Premature activation of zymogen granules, releasing proteases which digest the pancreas and surrounding tissue.The severity of pancreatitis depend on the balance between activity of released proteolytic enzymes and antiproteolytic factors.
Causes
Common (90%)- Gallstones
- Alcohol
- Idiopathic
- Post-ERCP
Rare:
- Drugs: thiazide, azathioprine, sodium valproate- Metabolic: hypercalcemia,hypertriglyceridemia - Infection: mumps
- Congenital: pancreas divisum
- Hereditary
- Trauma
Clinical approach
Aims:
- To establish the diagnosis
- To assess and stratify patients according to severity and to treat accordingly
- To identify and treat complications
- To prevent recurrences
Diagnosis
Two of three of the followings:1. Characteristic clinical features
2. Elevated pancreatic enzymes
3. Imaging evidence of pancreatic swelling
Clinical features
• Symptoms:• Pain: Almost all patients with acute pancreatitis have acute upper abdominal pain at the onset .
• The pain is steady and may be in the mid-epigastrium, right upper quadrant, diffuse, or, infrequently, confined to the left side.
• One characteristic of the pain that is present in about one-half of patients, is band-like radiation to the back
The abdominal pain is typically accompanied by nausea and vomiting, which may persist for many hours.
Restlessness, agitation, and relief on bending forward are other notable symptoms.
Patients with fulminant attacks may present in shock or coma
Signs
Marked epigastric tenderness
- Guarding and rebound tenderness are absent in the early stages (because the inflammation is retroperitoneal).
- Diminished or absent bowel sounds (localized paralytic ileus)
Grey-Turner's sign (ecchymotic discoloration in the flank )
or Cullen's sign (ecchymotic discoloration in the periumbilical region) occurs in 1 percent of cases but is not diagnostic.
These signs reflect intraabdominal hemorrhage and are associated with a poor prognosis.
- Jaundice due to obstruction of the common bile duct or edema of the head of the pancreas
Pancreatic enzymes
Serum amylase — Serum amylase is the most frequently ordered test to diagnose acute pancreatitis. It rises within 6 to 12 hours of onset, and is cleared fairly rapidly from the blood (half-life approximately 10 hours). In uncomplicated attacks, serum amylase is usually elevated for three to five days.Amylase must be measured early (within 24-48 hrs)
It is usually more than three times the upper limit of normal. However, the serum amylase may be normal or minimally elevated
It is nonspecific finding.
Question
What are the causes of high serum amylase?Serum lipase:
The sensitivity of serum lipase for the diagnosis of acute pancreatitis ranges from 85 to 100 percentLipase measurement is more specific than serum amylase
lipase measurements have been difficult to perform
Imaging studies
1. Abdo.USG:
Values:
- To exclude biliary pancreatitis (may show gallstones, biliary obstruction).
- Diagnosis: not sensitive,a diffusely enlarged, hypoechoic pancreas is the classic ultrasonographic image of acute pancreatitis
- Complications: pseudocyst
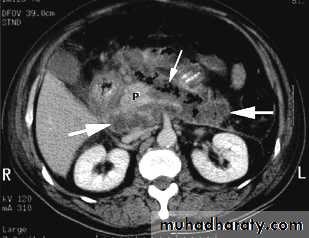
2. CT
- Early:To rule out other causes of acute abdomen
Late (3-8 days):
To define the viability of the pancreas (to detect pancreatic necrosis which manifest as decreased enhancement after iv contrast)
-
Abdominal plain film
To exclude other causes of abdominal pain such as obstruction and bowel perforation.The radiographic findings in acute pancreatitis range from unremarkable in mild disease to localized ileus of a segment of small intestine ("sentinel loop")
Chest Films
Approximately one-third of patients with acute pancreatitis have abnormalities visible on the chest radiograph such as elevation of a hemidiaphragm, pleural effusions, basal atelectasis, pulmonary infiltrates, or acute respiratory distress syndrome.Left-sided or bilateral pleural effusions suggest increased risk of complications
Assessment of severity
1. Mild: with minimal organ dysfunction and uneventful recovery.
Most attacks of AP are mild with recovery occurring within five to seven days.
Death is unusual (less than 3 percent)
2. Severe (necrotising pancreatitis): 15 to 25 percent
It is associated with a high rate of complications (local and systemic) and mortality (approximately 17 percent)
Bedside Index of Severity in Acute Pancreatitis(BISAP score)
Patients are assigned 1 point for each of the following during the first 24 hours: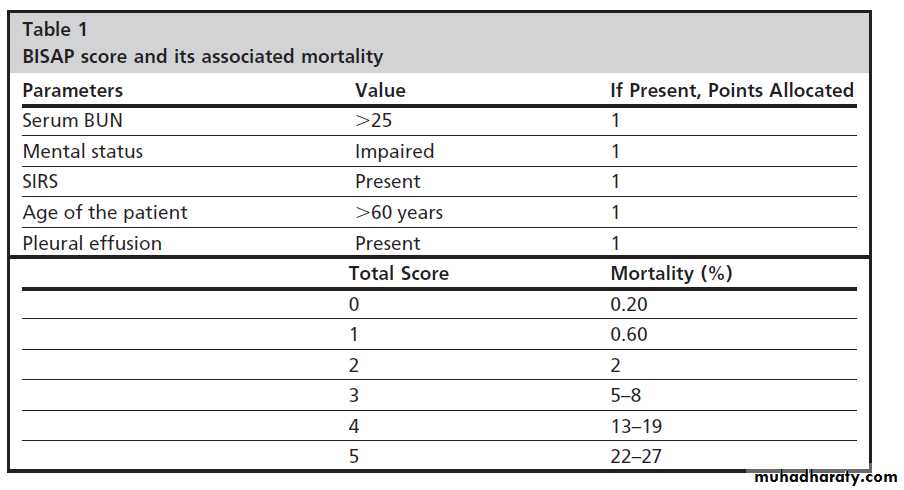
Question?
What are SIRS criteria?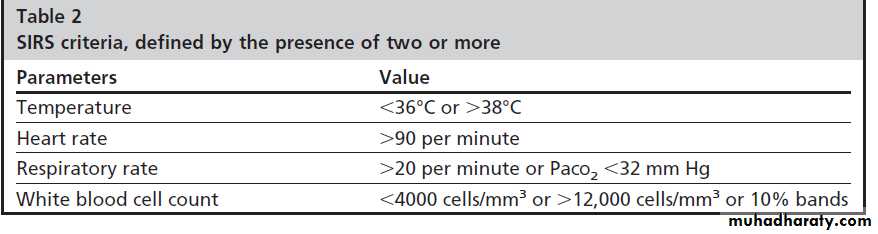
DD
- Acute MI
- Acute cholecystitis
- Perforated DU
Treatment
- Early treatment according whether the disease is mild or severe.- Detection and treatment of complications
- Treating the underlying cause – specifically gallstones
Initial management
1. Analgesia2. Correction of hypovolemia using aggressive
fluid resuscitation (targeting hematocrit 35%)
Type of iv fluid:
Use of the more pH-balanced lactated Ringer’s solution led to greater reduction in SIRS compared to the use of normal saline.
Vigorous fluid replacement is important because patients with necrotizing pancreatitis develop vascular leak syndrome .
Approximately 250 to 300 cc of intravenous fluids per hour are typically required for 48 hours if the cardiac status permits
Inadequate hydration can lead to hypotension and acute tubular necrosis.
In addition, fluid depletion damages pancreatic microcirculation and results in further pancreatic necrosis.
3. Correction of hypoxia if present, ventilatory support in patients who develop ARDS
4. NG tube: if paralytic ileus is present
5. Entral feeding should be started as soon as tolerated in patients with severe pancreatitis because they are in severe catabolic state and need nutritional support.
Enteral feeding also decrease endotoxaemia.
``
4. Prophylactic heparin
5. Prophylactic antibiotics:
Indications:
`It is only indicated in patients with infected pancreatic necrosis. Its use to prevent infection of necrosis is controversial.
6. Cholecystectomy should be performed within 2 weeks following resolution of pancreatitis in patients with biliary pancreatitis to prevent further attacks of pancreatitis.
7. Urgent endoscopic or surgical necosectomy in patients with necrotising pancreatitis or pancreatic abscess to debride all cavities of necrotic material.
8. Pancreatic pseudocysts are treated by drainge into the stomach, duodenum or jejunum
Complications(A): Local
1. Acute fluid collections: occur early in the course of acute pancreatitis, are located in or near the pancreas and always lack a wall of granulation of fibrous tissue.
In about half of patients, spontaneous regression occurs.
In the other half, an acute fluid collection develops into a pancreatic abscess or pseudocyst
2.Pancreatic necrosis: diffuse or focal area(s) of non-viable pancreatic parenchyma,

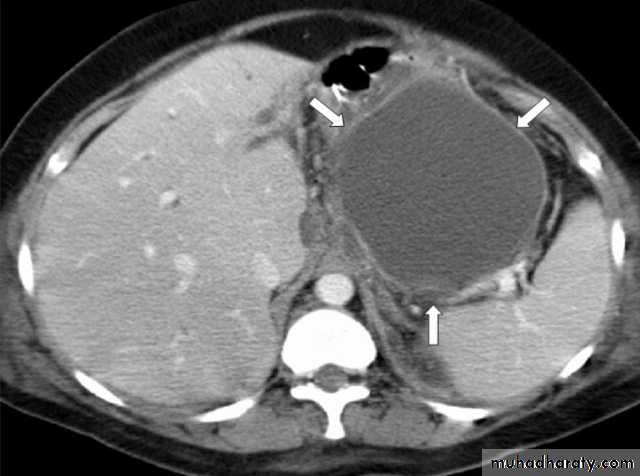
3. Acute pseudocyst: collection of pancreatic juice enclosed by a wall of fibrous or granulation tissue, occurring at least 4 weeks after onset of symptoms, is round or ovoid and most often sterile; when pus is present, lesion is termed a ‘pancreatic abscess’
4. Pancreatic abscess: circumscribed, intra-abdominal collection of pus, often 4 weeks or more after onset
B.Systemic complications
1.Shock : systolic blood pressure <90 mmHg2.Pulmonary insufficiency: PaO2 ≤ 60 mmHg
3.Renal failure: creatinine ≥177 μmol/l
4.Gastrointestinal bleeding
5.Disseminated intravascular coagulation :
platelets ≤100, 000/mm3, fibrinogen <1・0 g/l and fibrin-split products >80 μg/l
6.Severe metabolic disturbances :
( Calcium ≤1・87 mmol/l ( ≤7・5 mg/dl
Identification & treatment of underlying cause
1. History.
2. Physical examination
3. Blood tests
4. Imaging studies (USG, CT, MRI, MRCP, Endo.uss)
5. Genetic studies
Prevention of recurrence
- Can be achieved only after establishing the cause.- Total abstinence from alcohol is mandatory.
Cholecystectomy: it is imperative in patients with acute biliary pancreatitis
- Patients with acute biliary pancreatitis discharged from the hospital without a cholecystectomy, 30 to 50 percent develop recurrence of pancreatitis
Role of ERCP
1. Urgent ERCP—within 24 hours—is indicatedIn patients who have severe acute biliary pancreatitis with organ failure or cholangitis or both.
2. Elective ERCP with sphincterotomy can be considered in patients with :
a. Persistent or incipient biliary obstruction
b. Those deemed to be poor candidates for cholecystectomy
c. Those in whom there is strong suspicion of bile duct stones