Upper respiratory tract infection
By:Dr. Wael Thanoon
C.A.B.M.
College of medicine ,Mosul University.
The vast majority of these illnesses are caused by viruses , of which acute coryza (common cold) is by far the most common. Immunity is short-lived and virus-specific. Bacterial infection is the usual cause of acute tonsillitis, otitis media and epiglottitis.

Respiratory infections caused by viruses
Usual cause (other causes in parentheses)Clinical syndrome
Influenza A and B
Epidemic influenza
Adenoviruses, rhinoviruses (enteroviruses)
'Influenza-like' illness
Adenoviruses (enteroviruses, parainfluenza viruses, influenza A and B in partially immune)
Pharyngitis
Rhinoviruses (coronaviruses, enteroviruses, adenoviruses, respiratory syncytial virus)
Common cold (coryza)
Rhinoviruses, enteroviruses (influenza A and B, parainfluenza viruses, respiratory syncytial virus)
'Feverish' cold
Parainfluenza 1, 2, 3 (rhinoviruses, enteroviruses)
Croup
Rhinoviruses, adenoviruses (influenza A and B)
Bronchitis
Respiratory syncytial virus (parainfluenza 3)
Bronchiolitis
Influenza A and B, chickenpox (respiratory syncytial virus, parainfluenza, measles and adenoviruses)
Pneumonia
Acute epiglottis represents a medical emergency because of the risk of asphyxia, requiring prompt diagnosis and treatment, but those with other upper respiratory tract infections recover rapidly and specific investigation is rarely warranted. Viruses can be isolated from exfoliated cells collected on throat swabs, and may be identified retrospectively by serological tests. Throat swabs may also be helpful if streptococcal pharyngitis is suspected, and a blood film and serological testing will identify infectious mononucleosis. X-rays of the sinuses may be required if an underlying chronic sinusitis is suspected.
Common upper respiratory tract infections:
Acute coryza (common cold) :Clinical features :Rapid onset. Sneezing.
Sore throat. Watery nasal discharge.
Cough (Similar features in nasal allergy)
Complications :Sinusitis, bronchitis, pneumonia. Hearing impairment, otitis media due to blockage of Eustachian tubes
Management :Treatment not usually required. Paracetamol 0.5-1 g 4-6-hourly. Nasal decongestant. Antibiotics not necessary if uncomplicated .
Acute pharyngitis:
Clinical features:More severe sore throat. Hoarse voice or loss of voice with pain on speaking. Painful and unproductive cough. Stridor in children, caused by inflammatory oedema leading to partial obstruction of a small larynxComplications:Rare. Chronic laryngitis, tracheitis, bronchitis or pneumonia
Management:Rest voice. Paracetamol 0.5-1 g 4-6-hourly for relief of discomfort and pyrexia. Steam inhalations may help. Antibiotics not necessary if uncomplicated.
Sinusitis:
Clinical features: Fever. Severe unilateral pain over maxillary or other sinus. Purulent nasal discharge. Commonly viral, but bacterial (e.g. Strep. pneumoniae, H. influenzae) likely if persists 7-10 daysComplications: CNS or orbital spread of infection
Management: Steam inhalation and nasal decongestants. Co-amoxiclav if bacterial cause suspected.
Acute laryngo-tracheobronchitis (croup):
Clinical features: Sudden paroxysms of cough accompanied by stridor and breathlessness. Contraction of accessory muscles and indrawing of intercostal spaces. Cyanosis and asphyxia in small children
Complications: Death from asphyxia. Superinfection with bacteria, especially Strep. pneumoniae and Staph. aureus. Viscid secretions may occlude bronchi.
Management: Steam inhalations and humidified air/high concentrations of oxygen. Endotracheal intubation or tracheostomy may be required to relieve laryngeal obstruction and allow clearing of bronchial secretions. Intravenous co-amoxiclav or erythromycin for serious illness. Maintain adequate hydration .
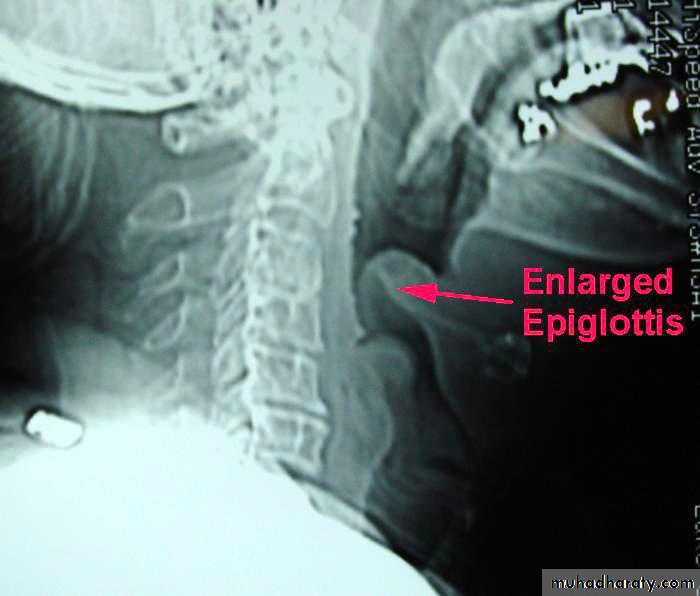
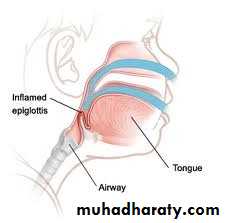
Acute epiglottitis:
Clinical features :Mostly affects young children. Fever and sore throat, progressing to stridor and dysphagia caused by swelling of epiglottis and surrounding structures. Due to H. influenzae type bComplications: Death from asphyxia, which may be precipitated by attempts to examine the throat-avoid using a tongue depressor or any instrument unless facilities for endotracheal intubation or tracheostomy are immediately available
Management: I.v. co-amoxiclav or chloramphenicol therapy essential.Urgent endotracheal intubation or tracheostomy may be necessary
Acute bronchitis and tracheitis:
Clinical features: Often follows acute coryza. Initial dry, painful cough with retrosternal discomfort in tracheitis. Chest tightness, wheeze and breathlessness if bronchitis develops. Sputum is initially scanty or mucoid, then becomes mucopurulent, more copious and, in tracheitis, often blood-stained. Acute bronchitis may be associated with a pyrexia of 38-39°C. Spontaneous recovery occurs over a few daysComplications: Bronchopneumonia. Exacerbation of asthma or COPD which, if severe, may result in type II respiratory failure
Management: Specific treatment rarely necessary in previously healthy individuals. Amoxicillin 250 mg 8-hourly should be given to those developing bronchopneumonia. Cough may be eased by pholcodine 5-10 mg 6-8-hourly. In COPD and asthma, aggressive treatment of exacerbations may be required .
Influenza:
Clinical features: Range from mild to rapidly fatal. Sudden onset of pyrexia with generalised aching, headache, anorexia, nausea and vomiting, and harsh unproductive cough. Most recover within 3-5 days, but may be followed by 'post-viral syndrome' with debility that persists for weeks. During epidemics, diagnosis is usually obvious. Sporadic cases diagnosed by virus isolation, fluorescent antibody techniques or serological tests for specific antibodies
Complications: Tracheitis, bronchitis, bronchiolitis and bronchopneumonia. Secondary bacterial invasion by Strep. pneumoniae, H. influenzae and Staph. aureus may occur. Rarely, toxic cardiomyopathy (may cause sudden death), encephalitis, demyelinating encephalopathy and peripheral neuropathy
Management: Bed rest. Paracetamol 0.5-1 g 4-6-hourly. Pholcodine 5-10 mg 6-8-hourly for cough. Specific treatment for pneumonia may be necessary. Antiviral agents (e.g. zanamivir) reduce the rate of viral replication and may be effective when used as an adjunct to vaccination. Antiviral resistance is a potential problem.