1
Forth stage
Medicine
Lec-5
د.جاسم محمد
9/11/2015
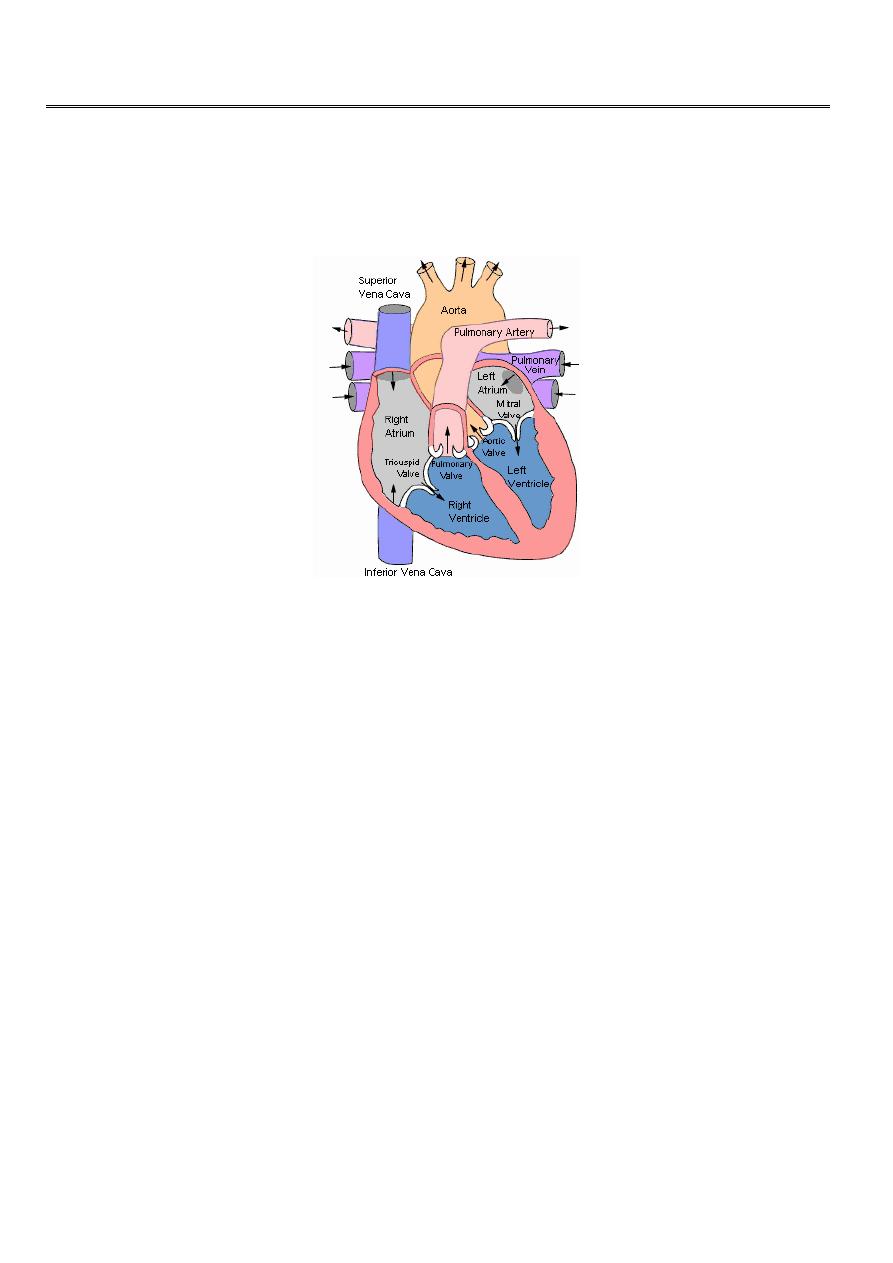
Aortic Stenosis
Overview:
• Normal Aortic Valve Area: 3-4 cm
2
• Symptoms:
Occur when valve area is 1/4th of normal area.
• Types:
Supravalvular
Subvalvular
Valvular
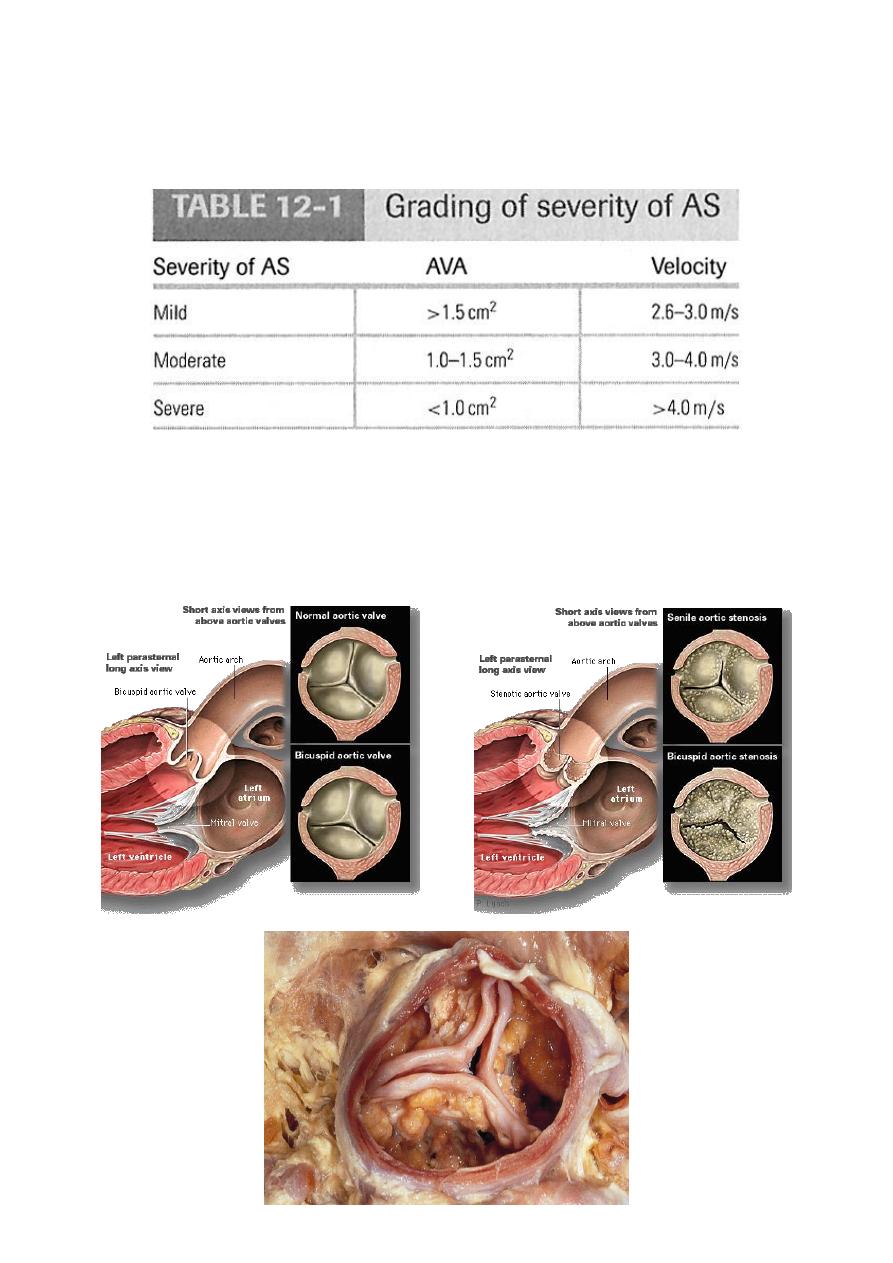
Etiology of Aortic Stenosis
• Congenital (Bi-cusped).
• Rheumatic.
• Degenerative/Calcific.
Patients under 70: >50% have a congenital cause
Patients over 70: 50% due to degenerative
2
Evaluation of AS:
Cardiac catheterization
:
Should only be done for a direct measurement if symptom severity
and echo severity don’t match OR prior to replacement when replacement is planned.

3
Pathophysiology of Aortic Stenosis
A pressure gradient develops between the left ventricle and the aorta. (Increased
afterload)
LV function initially maintained by compensatory pressure hypertrophy
to maintain the cardiac output
When compensatory mechanisms exhausted, LV function declines and pulm.edema
supervenes.
Presentation of Aortic Stenosis:
1. Asymptomatic mild/moderate
2. Syncope: (exertional)
3. Angina: (increased myocardial oxygen demand; demand/supply mismatch)
4. Dyspnea: on exertion due to heart failure (systolic and diastolic)
5. Sudden death
Physical Findings in Aortic Stenosis
Slow rising carotid pulse (pulsus tardus)
Thrusting apex beat (LV pressure overload)
Narrow pulse pressure
Heart sounds- soft and split second heart sound, S4 gallop due to LVH.
Systolic ejection murmur- cresendo-decrescendo character. This peaks later as the
severity of the stenosis increases.
Loudness does NOT tell you anything about severity
4
Investigations
ECG Left ventricular hypertrophy ,LBBB
Chest X-ray May be normal; sometimes enlarged LV and dilated ascending aorta on
PA view, calcified valve on lateral view.
Echo Calcified valve with restricted opening, hypertrophied LV) Doppler
Measurement of severity of stenosis Detection of associated aortic regurgitation.
Cardiac catheterization Mainly to identify associated coronary artery disease May
be used to measure gradient between LV and aorta.
Management of AS
General- IE prophylaxis in dental procedures with a prosthetic AV or history of
endocarditis.
Medical - limited role since AS is a mechanical problem. Vasodilators are relatively
contraindicated in severe AS
Aortic Balloon Valvotomy- shows little benefit.
Surgical Replacement: Definitive treatment
Simplified Indications for Surgery in Aortic Stenosis
Any SYMPTOMATIC patient with severe AS (includes symptoms with exercise)
Any patient with decreasing EF
Any patient undergoing CABG with moderate or severe AS
5
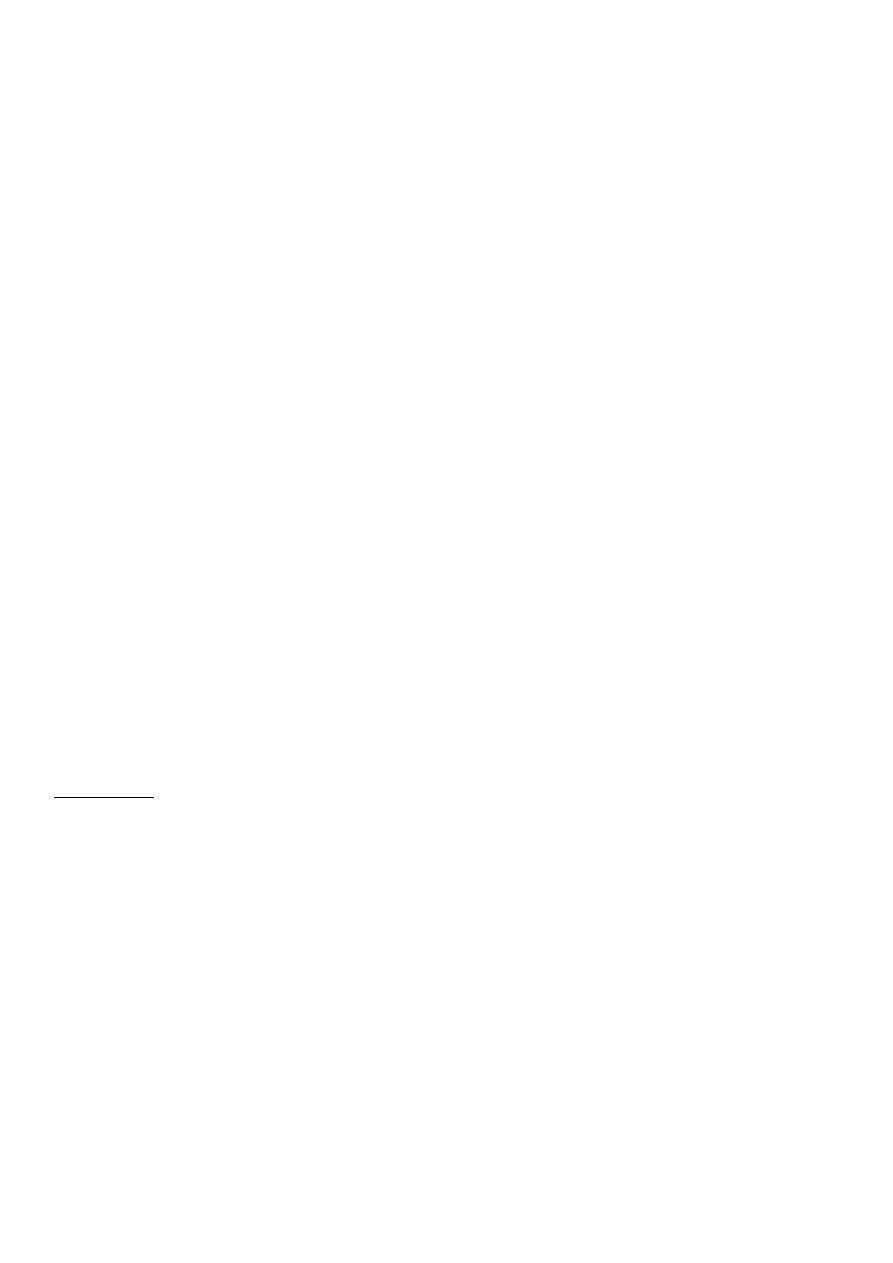
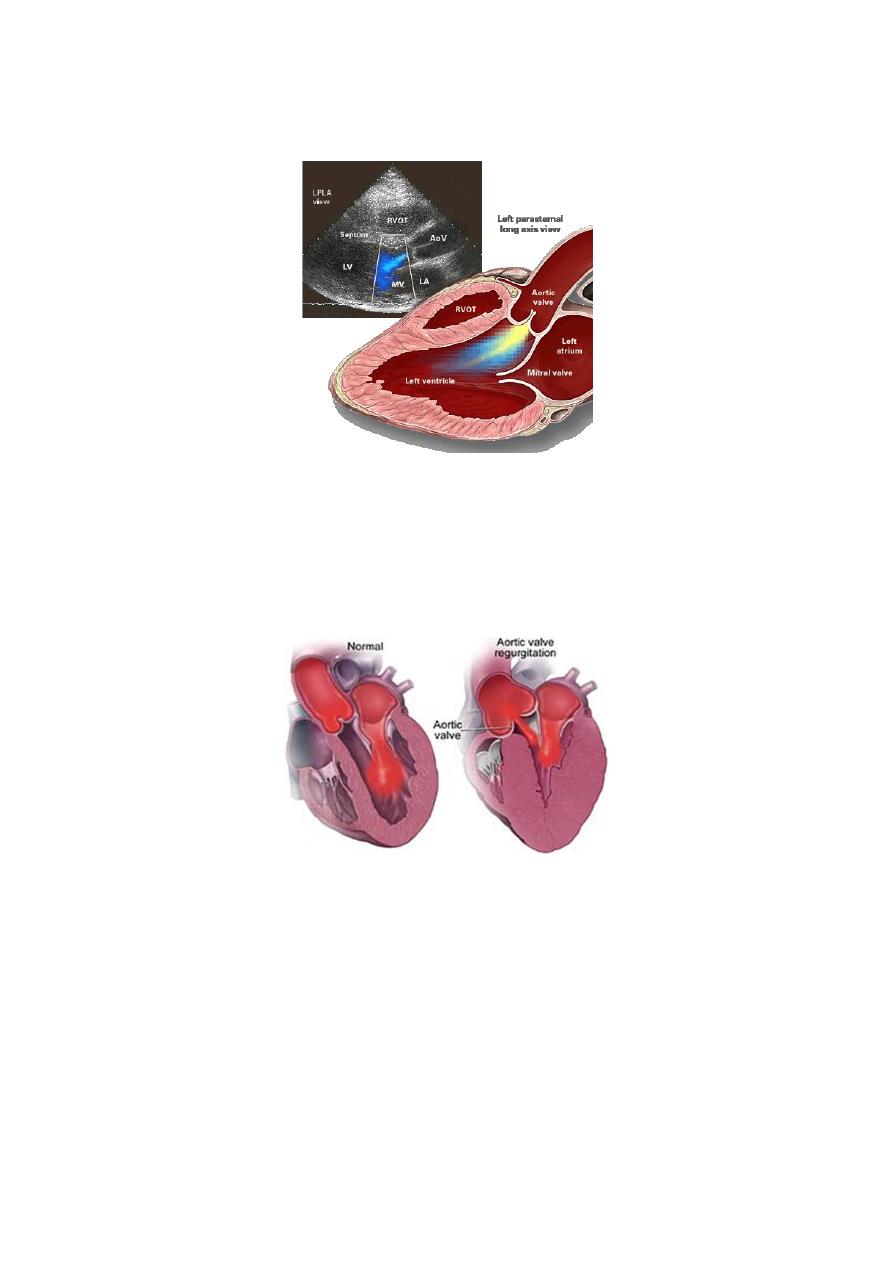
Aortic Regurgitation
Overview:
Definition:
Leakage of blood into LV during diastole due to ineffective coaptation of the
aortic cusps.
Etiology of Acute AR
Endocarditis
Aortic Dissection
Physical Findings:
Wide pulse pressure
Diastolic murmur
Florid pulmonary edema
6
Treatment of Acute AR
True Surgical Emergency:
Positive inotrope: (e.g., dopamine, dobutamine)
Vasodilators: (e.g., nitroprusside)
Avoid beta-blockers
Do not even consider a balloon pump
Etiology of Chronic AR
Cusps defects
Congenital -Bicuspid aortic valve
Rheumatic
Infective endocarditis
Aortic root dilatation Marfan.
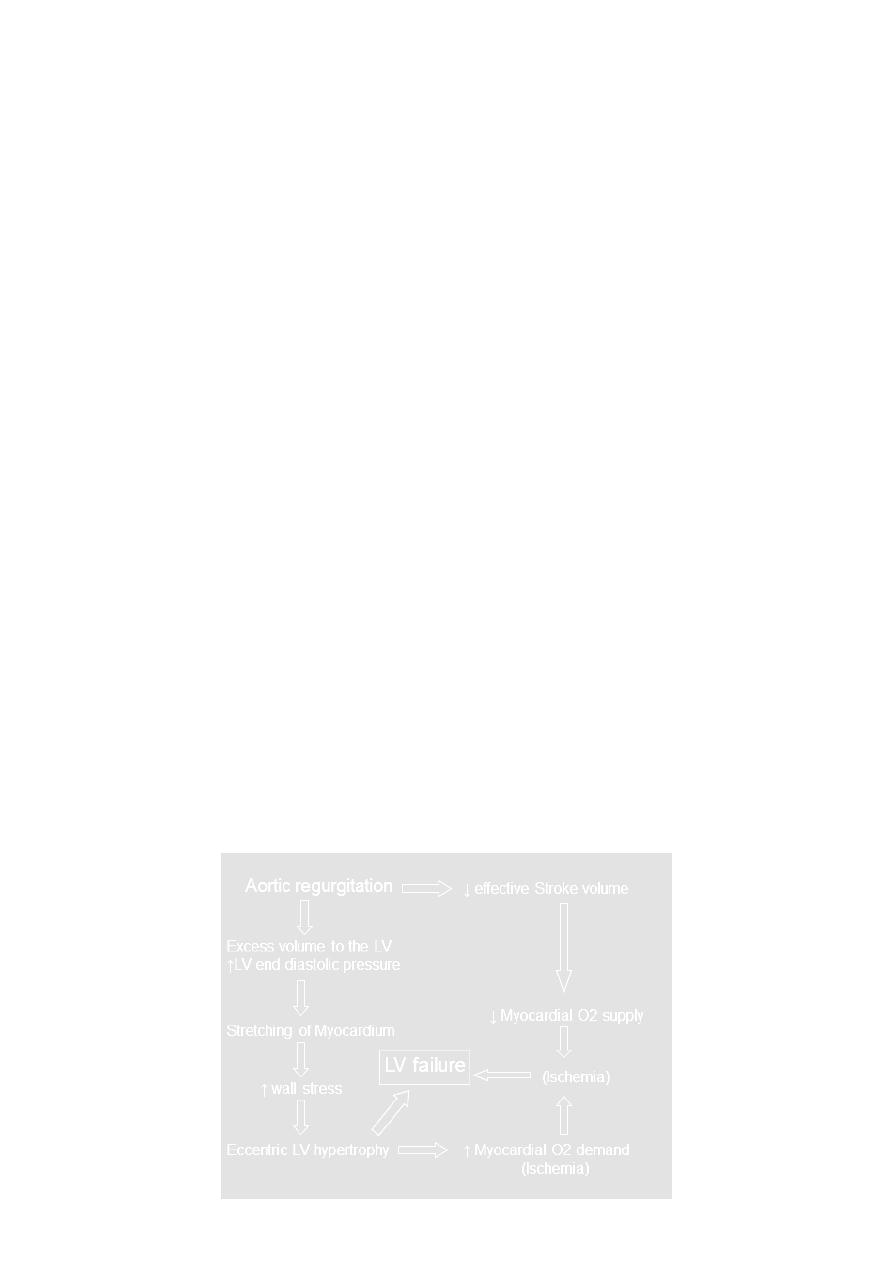
Pathophysiology of AR
Combined pressure AND volume overload
Compensatory Mechanisms: LV dilation, LVH. Progressive dilation leads to heart
failure.
7
Symptoms
Asymptomatic until 4th or 5th decade
Progressive Symptoms include:
Dyspnea: exertional, orthopnea, and paroxysmal nocturnal dyspnea
Nocturnal angina: due to slowing of heart rate and reduction of diastolic blood
pressure.
Palpitations: due to increased force of contraction.
Signs
Peripheral signs
• Pulses Large volume or ‘collapsing’ pulse.
• Corrigan pulse
• Increased pulse pressure
• Bounding peripheral pulses
• Capillary pulsation in nail beds: Quincke’s sign Femoral bruit (‘pistol shot’)
• Duroziez’s sign
• Head nodding with pulse: de Musset’s sign.
• Hill’s sign
• JVP may be normal or elevated
Central Signs
• Apex: Hyperdynamic and displaced apical impulse.
• Diastolic thrill.
Auscultation
•
High pitched, blowing, decrescendo diastolic murmur at LSB, best heard at end-
expiration & leaning forward.
• Austin-Flint murmur indicates severity (mid to late diastolic murmur)
• Systolic murmur related to high flow state
8
Investigations
• ECG Initially normal, later left ventricular hypertrophy and T-wave inversion
• Chest X-ray Cardiac dilatation, maybe aortic dilatation Features of left heart failure
• Echo Dilated LV Hyperdynamic, LV Doppler detects reflux , Fluttering anterior mitral
leaflet
• Cardiac catheterization (may not be required) , Dilated LV , Aortic regurgitation ,
Dilated aortic root.
Management of AR
• General: IE prophylaxis in dental procedures with a prosthetic AV or history of
endocarditis.
• Medical: Vasodilators (ACEI’s), Nifedipine improve stroke volume and reduce
regurgitation only if pt. symptomatic or HTN.
• Serial Echocardiograms: to monitor progression.
• Surgical Treatment: Definitive Rx
Simplified Indications for Surgical Treatment of AR
• ANY Symptoms at rest or exercise
• Asymptomatic treatment if:
• EF drops below 50% or LV becomes dilated.
9
Tricuspid Regurgitation
CLASSIFICATION OF TR
PRIMARY: Intrinsic abnormality of the valve apparatus
SECONDARY OR FUNCTIONAL : Caused by RV pressure or volume overload.
Aetiology
Primary
Rheumatic fever
Endocarditis
Ebstein anomaly
Secondry
Right venytricular dilatation
Right ventricular infarction
Pulmonary hypertension
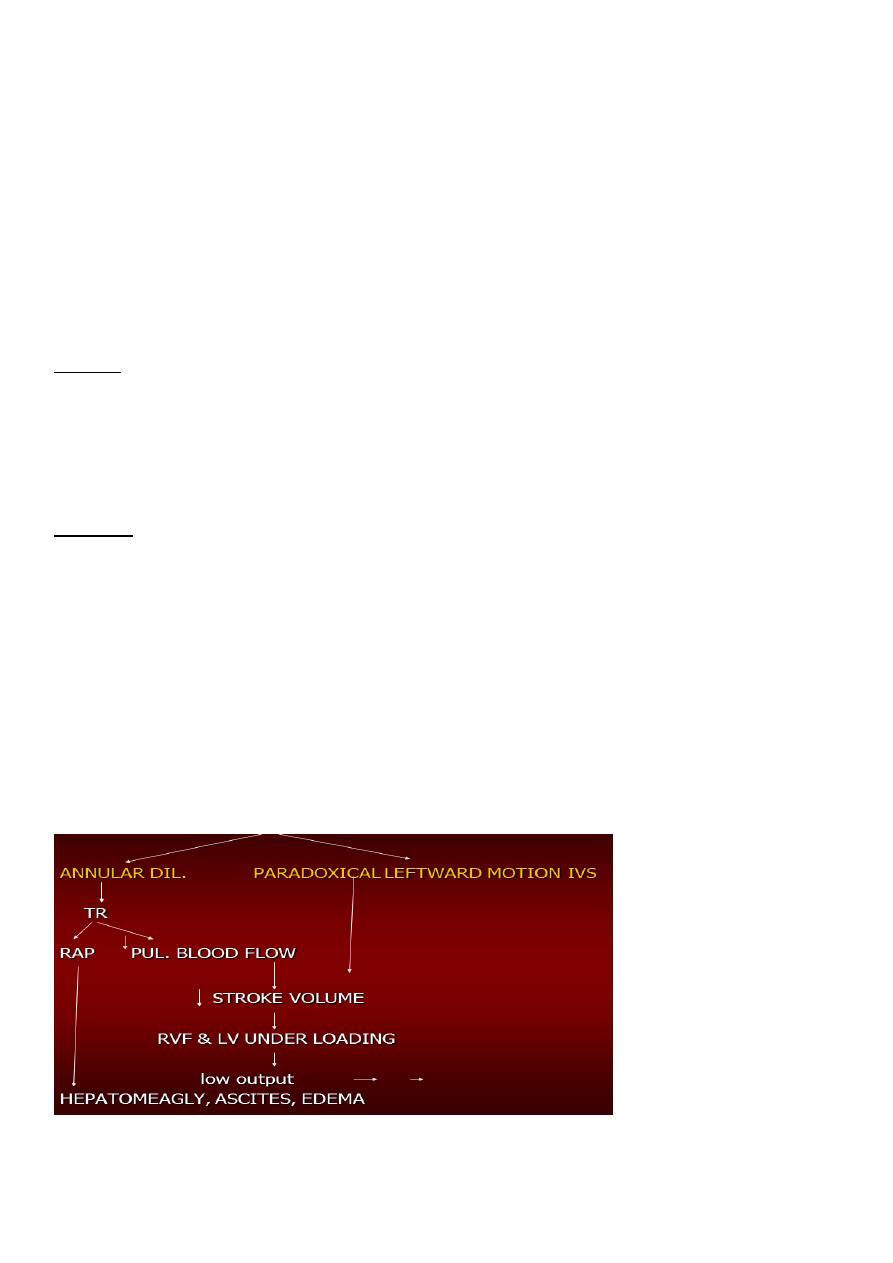
Pathophysiology
primary structural abnormalities of the leaflets and chordae
- secondary to myocardial dysfunction and dilatation.
Symptoms
presents with the signs and symptoms of right-sided heart failure.
11
The spectrum includes
Tirdness
Jaundice, loss of wt and appetite
ascites
peripheral edema.
Concomitant valve lesion
Signs
Jugular venous distention with a prominent V wave cv .
Atrial fibrillation
RV heave and gallop
Pansystolic murmur ,S3
Ascites, peripheral edema, cachexia, cyanosis, systolic pulsation of liver and jaundice
INVESTIGATION
o Chest radiography
Marked cardiomegaly is evident.
Pulmonary arterial and venous hypertension is common.
o Echocardiography
The right ventricle is dilated.
Paradoxical motion of the ventricular septum ..
Prolapse of the tricuspid valve
Vegetations if endocarditis is present.
o Electrocardiography
Findings are usually nonspecific.
Incomplete right bundle-branch block,
o Cardiac catheterization
Right atrial pressure and RV end-diastolic pressure are elevated.
The use of angiography in this setting is controversial.
Lab Studies:
abnormal liver function and hyperbilirubinemia secondary to liver congestion.
Management
Treatment of failure symptoms.
TR associated with mitral valve disease and pulmonary hypertension ,Severe
regurgitation -- tricuspid annuloplasty.
Damged valve may need TVR

11
Tricuspid Stenosis
Almost always rheumatic in origin
Usually accompanied by mitral stenosis
The valve leaflets become thickened and sclerotic as the chordae tendineae become
shortened. Right atrial enlargement occurs due to the increased pressure build-up.
Other causes:
Carcinoid heart disease
Congenital tricuspid atresia
Infective endocarditis
Right atrial myxoma
SYMPTOMS
Usually symptoms of associated lesion (mitral) predominates
Features of right side heart failure
abdominal discomfort ,peripheral edema
SIGNS
JVP raised with prominent a wave
Mid diastolic murmur at left lower sternal edge
Right sided heart failure features
INVESTIGATION
ECG
CHEST –X ray
ECHO
TREATMENT
During surgery on other valves,the tricuspid valve either replaced or valvotomy
Ballon valvuloplasty for isolated TS,

12
Pulmonary Stenosis
Majority of PS is congenital (accounts for 7.6% of CHD)
Rarely due to carcinoid disease,
Mild PS may be asymptomatic
Symptoms include shortness of breath, chest pain, fainting, or exertional syncope,
SIGNS
Systolic thrill
LPH
Ejectiom systolic murmur ,click,wide splitting of S2
INVESTIGATION
ECG RVH
CHEST –Xray poststenotic dilatation
ECHO –DOPPLER
TREATMENT
Mild to moderate no treatment
Sever (gradient more than 50mmHg)
Balloon valvuloplasty or surgical valvotomy
Pulmonary Regurgitation
Common complication after surgical or percutaneous relief of pulmonary stenosis
May occur secondary to a dilated pulmonary valve ring due to pulmonary
hypertension or Marfan's disease
PR occurs rarely as a congenital anomaly
PR leads to progressive right ventricular dilatation, right ventricular dysfunction,
Signs and Symptoms
Symptoms of underlying disease
Early diastolic murmue decrescendo (Graham steel)
Features of pulmonary hypertension
Treatment
Treatment of cause