
1
Forth stage
Surgery (Urology)
Lec- 0
2
د.محمد فوزي
5/11/2015
URINARY STONES
Calcular disease
Incidence
:-
Common, affecting 10-20% of population 1.
2. Males affected more than females.
3. Occurs mainly in middle age, but no age immune.
4. 2/3 patients have recurrence within 8 years.
Aetiology
:-
1. Geography: tropical area, mountainous and Mediterranean countries.
2. Climate: direct relationship between temp and stone incidence.
3. low Water intake.
4. Diet.
5. Socio-economic status.
6. Metabolic & endocrinal factors :-
I-Ca
++
oxalate & Ca
++
phosphate calculi:-
Hypercalcemia (hyperparathyroidism)
Hypercalciuria.
Hyperoxaluria: primary (congenital), secondary (enteric disease) or idiopathic
(dietary).
Hypocitraturia .
Hyperuricosuria .
Renal tubulal acidosis .
associated with hypercalciuria & hypocitraturia.
II-Uric acid calculi : Hyperuricemia and hyperuricosuria.
III-Cystine calculi:hereditary cystinuria.
IV-Xanthine calculi:hereditary xanthinuria .
7. Infection: UTI due to urea splitting MO (urease producing MO) causes urine
alkalinazation hence phosphate precipitation. (triple phosphate stones).
8. Congenital anomalies.
Types of renal calculi :-
l-Calcium stones: 70%, radio-opaque
a. Calcium Oxalate :
Calcium oxalate monohydrate: smooth, dark and hard.
2
Calcium oxalate dihydrate: granular, lighter in colour and fragment easily.
b. Calcium phosphate calculi: radio opaque.
They grow in alkaline urine and attain large size. Staghorn calculus.
II-Triple phosphate calculi (Struvite):
Grows very rapidly in alkaline urine, radio-opaque.
III-Uric acid calculi: hard, smooth and golden yellow.
Pure uric acid stones are radiolucent.
Symptoms :-
1. Asymptomatic.
2. Loin pain.
3. uretric colic.
4. Hematuria.
5. Infection or pyuria.
6. Renal failure.
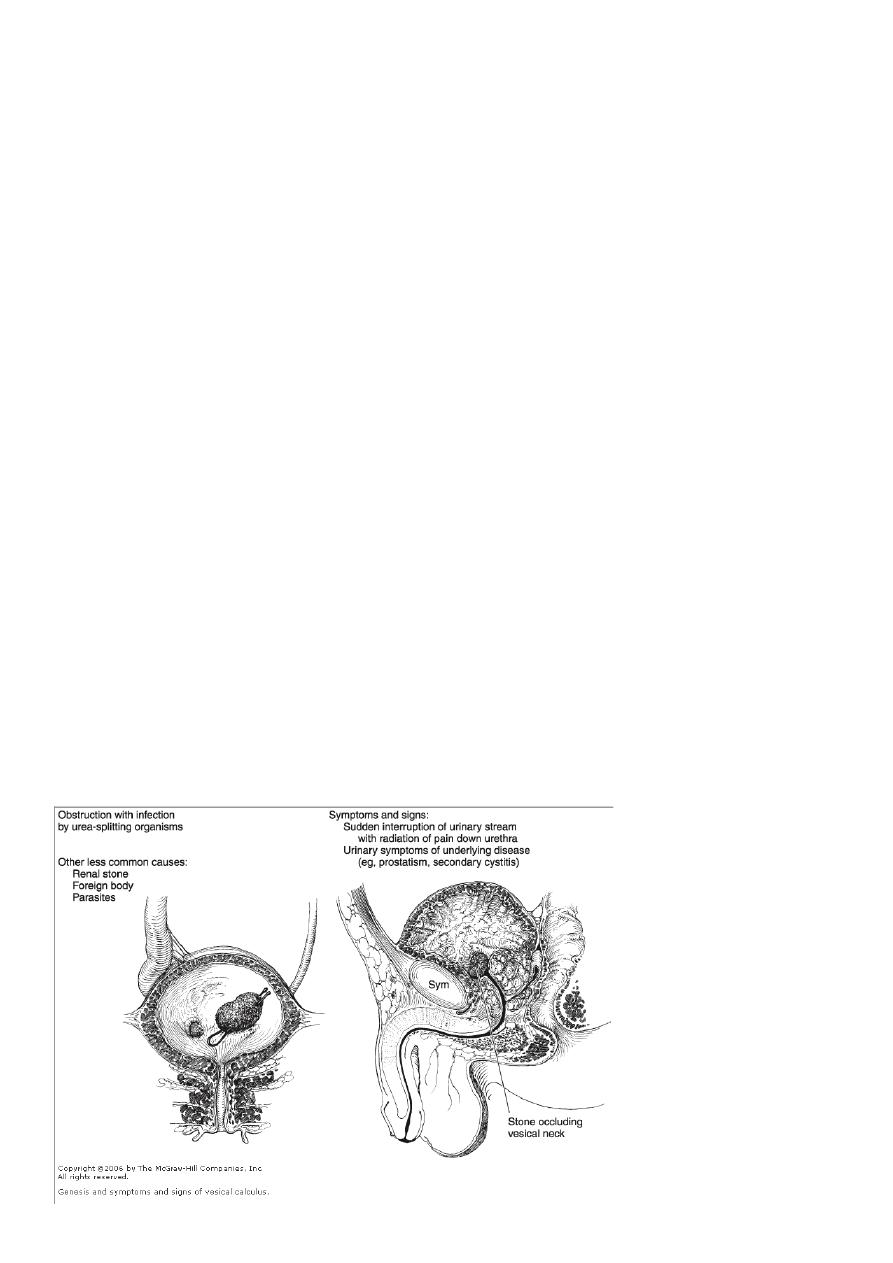
Urinary bladder stone :-(vesical)
Etiology
:-
Children: dehydration, low protein diet & UTI
Adult:
1. Urinary obstruction: BPH & stricture.
2. UTI.
3. Neurogenic bladder dysfunction.
4. Foreign body.

3
Clinical pictures :-
1. Pain: suprapubic pain, penile pain especially at the tip of the penis or labia majora at the
end of micturition.
2. Frequency of urination.
3. Difficulty in micturition or retention of urine.
4. Hematuria.
Urethral stones :-
Origin
:-
Most often migrated from the ureter and arrested in the prostatic or bulbous urethra.
Less commonly originated in the urethral diverticulum (Ca
++
phosphate).
Clinical pictures :-
1. Severe urethral pain during urination.
2. Interruption of urine stream.
3. Retention of urine.
4. Urethral ex.:induration of the stone.
5. Click felt by metal bougie.
Investigations :-
1. GUE: microscopic hematuria 90%, sterile pyuria and crystalluria.
2. U/S : stone shadow, hydronephrosis and hydroureter. The whole ureter cannot be
visualized.
3. KUB: 90% radio-opaque & soft tissue shadow of hydronephrotic kidney.
Differential diagn osis of radio opaque shadow in KUB :-
Gall stone, calcific LN,FB
Phlebolith, fecolith, calcified TB lesion
Chip # of transverse process, calcified rib tip
Calcified fibroid and ovarian dermoid cyst.
IVU: Hydronephrosis, renal function, site of obstruction and filling defects in
radiolucent stones.
Retrograde pyelography.
CT scan & MRI.
Endoscopic: urethroscope, cystoscope, ureteroscope and nephroscope.
Management of urinary stones :-
AIMS :
1. Relief pain and colic.
4
2. Eliminate or stone removal.
3. Prevention of recurrence.
Renal colic
:
strong analgesia, NSAID (Diclfenac 75 mg im) or narcotics (Pethidin 50-100
mg im).
Hydration in dehydration.
Antibiotics in renal infection.
Hospitalization may be needed.
Conservative treatment
:-
Stones less than 5mm have 50% chance of spontaneous passagE
High fluid intake,after pain relief and follow up by KUB ,ULS.CT.
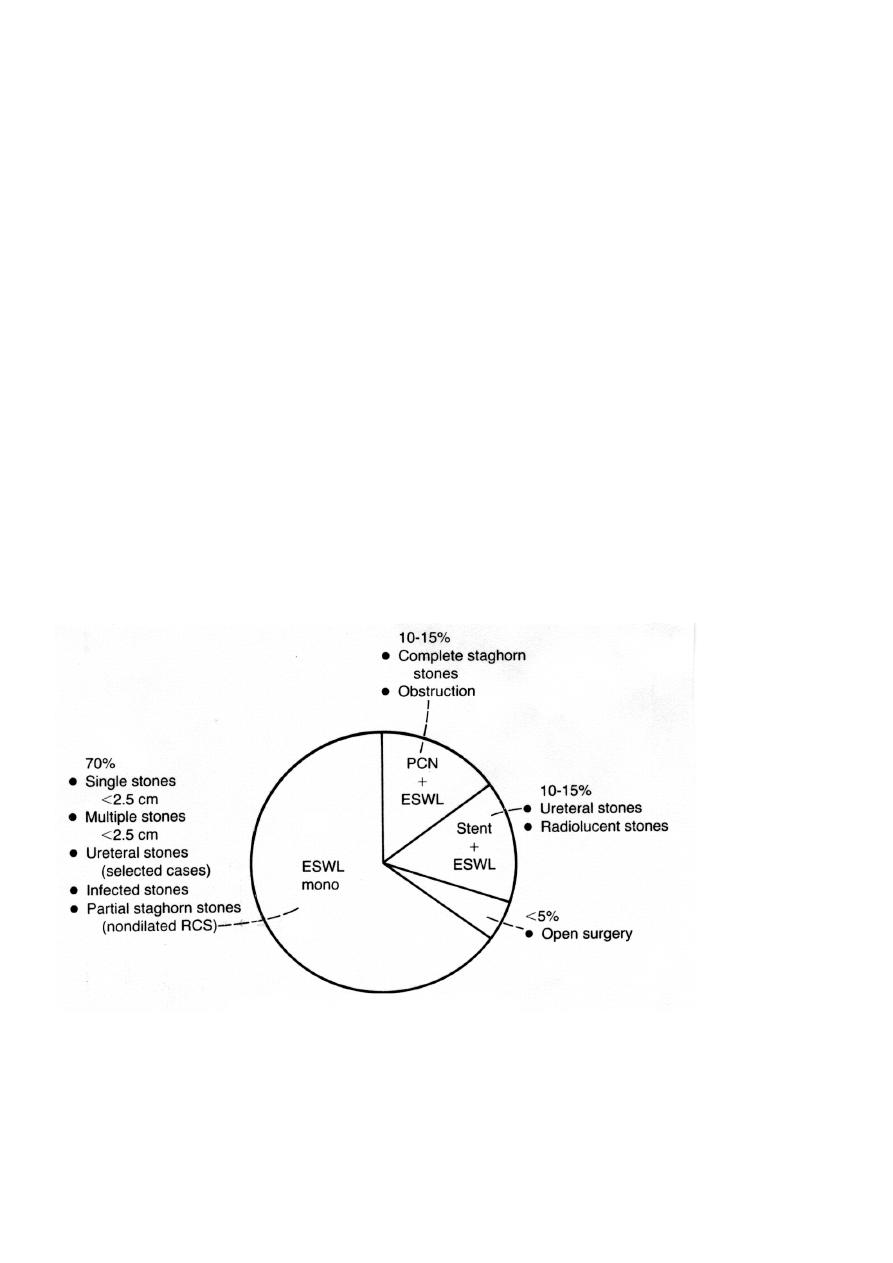
Methods of intervention :-
1. Extracorporeal shock wave lithotripsy (ESWL).
2. Percutaneous nephrolithotomy (PCNL).
3. Open surgery.
4. Chemolysis.
5. Combination.like ESWL AND PCNL.
6. Ureteronephroscopy with laser.
1- ESWL
Indications: all stones less than 2 cm in the kidney and ureter.
Contraindications: large stones, bleeding tendency, , ureteric obstruction, renal
insufficiency, pregnancy, skeletal anomaly and overweight.

5
Complications of ESWL:-
1. Failure of stone fragmentation.
2. Hematuria.
3.
Ureteric colic.
4. Ureteric obstruction (stone street). Stone in single kidney needs JJ stent.
5. Infection.
6. Rapid recurrence due to residual fragments.
Indication of jj stent in ESWL :
1. Large stone
2. Stone in a single kidney
2- PCNL :
Using electrohydrulic lithotripter through percutaneous nephroscope to retrieve the renal
stones.
Advantages :-
1. Small endoscopic wound
2. Mild post operative pain.
3. Short hospital stay.
3- Open surgery :
I
ndications :-If ESWL or PCNL are contraindicated or failed.
Methods :
1. Pyelolithotomy.
2. Nephrolithtomy.
3. Pyelonephrolithotomy.
4. Partial nephrectomy.
5. Nephrectomy.
4- Dissolution agents (chemolysis) :
oral alkalinizing agents for uric acid & cystine stones.
Acidification in struvite tone.
Methods of ureteric stones treatment :
1. Conservative
2. ESWL
3. Ureteroscopic manipulation.
4. Dormia basket stone extraction.
5. Ureterolithotomy:
Expectant treatment
-
conservative :
Spontaneous passage depends on stone size, shape, location
Ureteral calculi 4-5 mm in size have a 40-50% chance of spontaneous passage . In contrast,
calculi > 6 mm have a less than 5% chance of spontaneous passage.

6
Sites of stone impaction :
1. Pelviureteric junction.
2. Pelvic brim.
3. Ureterovesical junction.
Indications for intervention :
1. Repeated attacks of pain &the stone is not progressing.
2. Stone is enlarging with time.
3. Complete obstruction of the kidney.
4. Symptoms & signs of infection.
5. Stone is too large to pass.
6. Stone is obstructing solitary kidney or there is bilateral obstruction.
7. Impaired renal function( elevated urea & creatinine).
Ureteroscopic Stone Removal :
Small stones removed as one piece using forceps under direct vision. Large stones are
fragmented using pneumatic, electrohydraulic , or Laser Lithotripter then removed in
pieces.
Ureterolithotomy :
- Open Ureterolithotomy.
- Laparoscopic Ureterolithotomy.
Treatment of Vesical Stone :
1. Treat the underlying cause.
2. Cystolitholapaxy (Endoscopic) :Its minimally invasive technique allowing most stones to
be broken and subsequently removed through a cystoscope...stone crushing by
electrohydraulic, ultrasonic, laser, and pneumatic lithotrites . Mechanical lithotrites (stone
punch) & Elik evacuator.
3. Suprapubic cystolithotomy.
4. Laparoscopic cystolithotomy.
5. ESWL.
IN CHILDREN :
Suprapubic cystolithotomy
.
Treatment of urethral stone :
1. Treat the underlying cause.
2. Small stones may be grasped successfully and removed intact . 3.pushed back to the
bladder,and trated as vesical stone.
4. Long-standing, large impacted stones are best removed through a urethrotomy.