1
Forth stage
Surgery
Lec-6
د
.
ليث
الحرباوي
4/18/2016
Rectal tumors
Benign tumour:
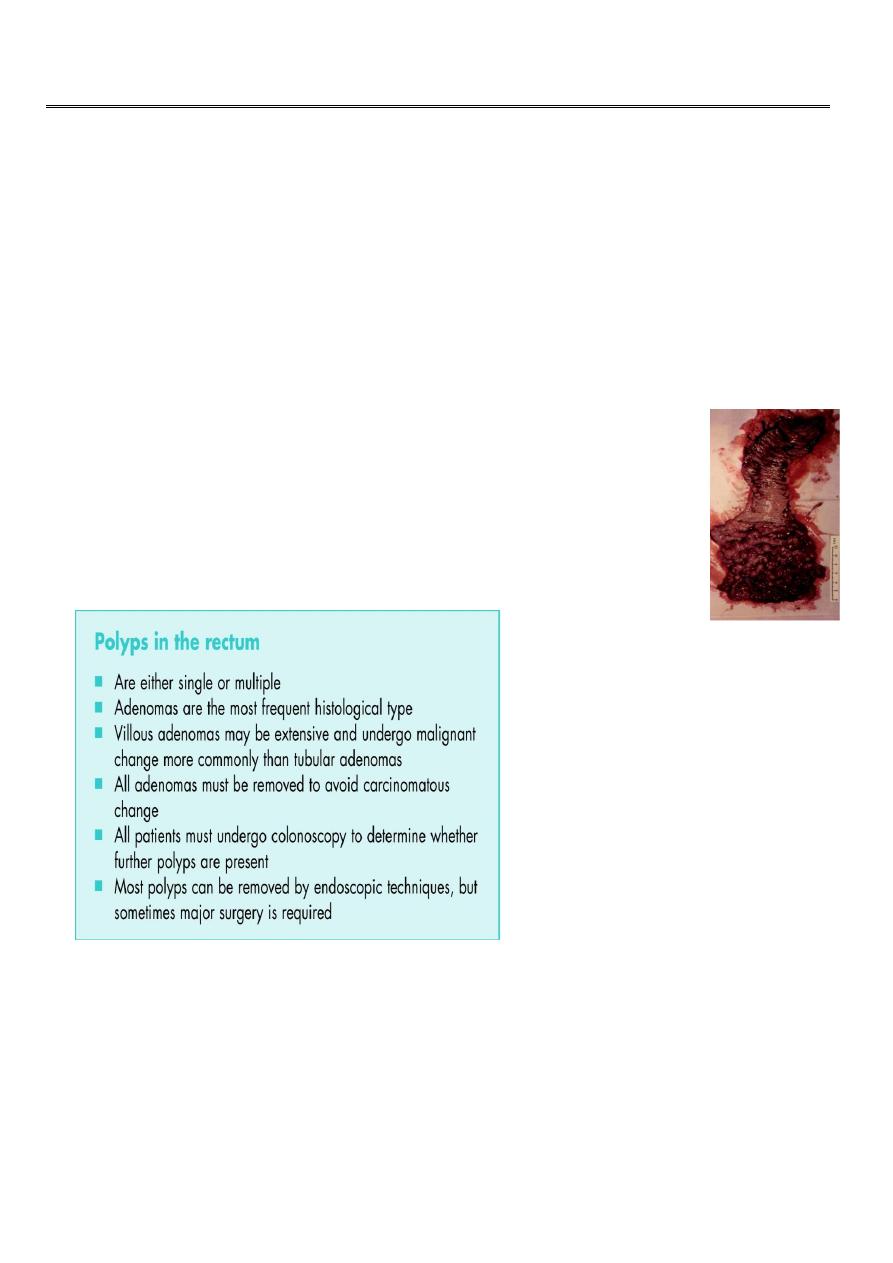
Villous adenomas:
These have a characteristic frond-like appearance. They may be very large, and
occasionally fill the entire rectum. These tumours have an enhanced tendency to
become malignant – a change that can sometimes be detected by palpation with the
finger; any hard area should be assumed to be malignant and should be biopsied.
Rarely, the profuse mucous discharge from these tumours, which is rich in potassium
Familial adenomatous polyposis
Hyperplastic polyps:
These are small, pinkish, sessile polyps, 2–4 mm in diameter and
frequently multiple. They are common and generally harmless.
Inflammatory pseudopolyps
Juvenile polyp
CARCINOMAS :
Types of carcinoma spread :
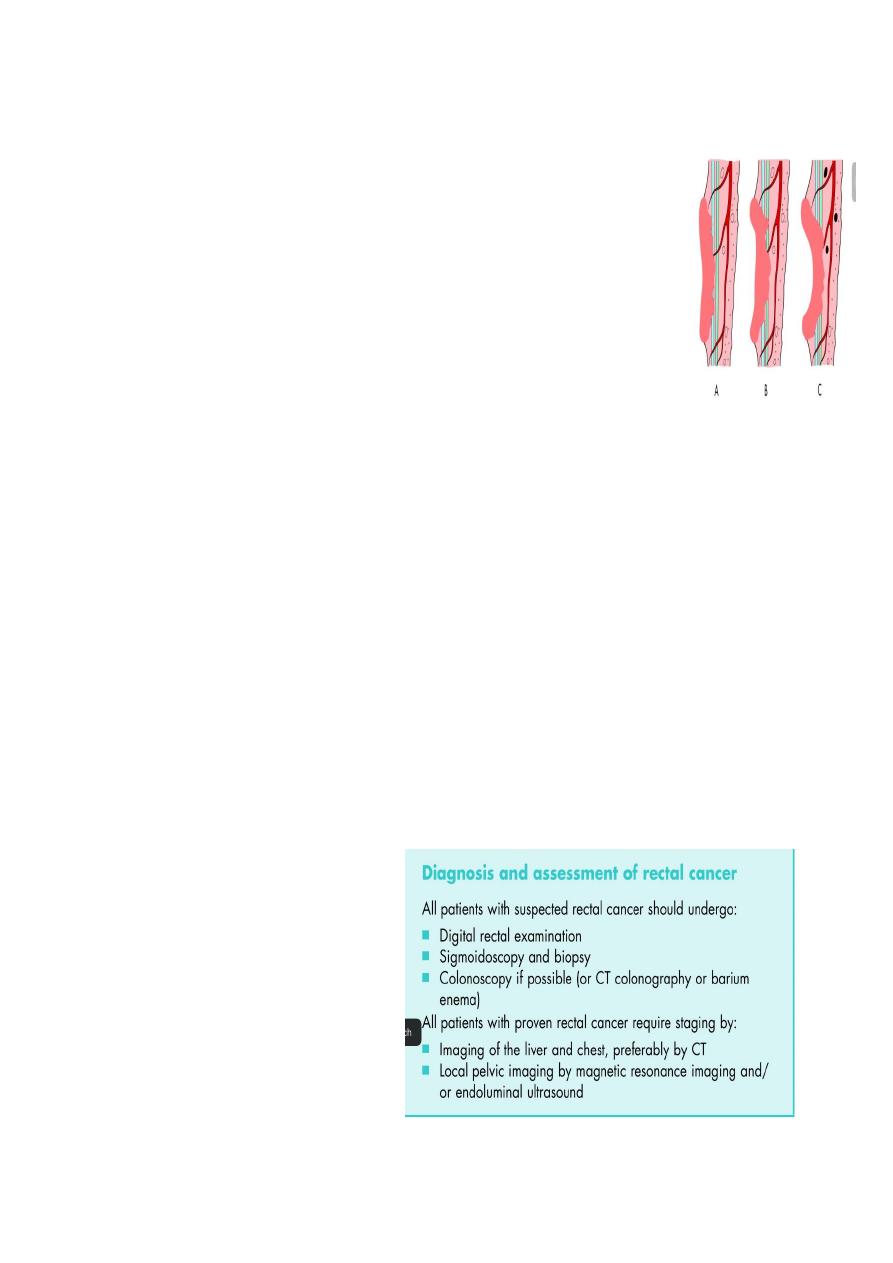
1. Local spread:
Local spread occurs circumferentially rather than in a longitudinal direction. After the
muscular coat has been penetrated, the growth spreads into the surrounding
mesorectum, but is initially limited by the mesorectal fascia.
2
2. Lymphatic spread:
Lymphatic spread from a carcinoma of the rectum above the peritoneal reflection
occurs almost exclusively in an upward direction.
3. Venous spread
4. Peritoneal dissemination
Stages of progression
Dukes classified carcinoma of the rectum
TNM staging
Histological grading:
Low grade, well-differentiated 11 per cent prognosis good;
Average grade, 64 per cent prognosis fair;
High grade, undifferentiated tumours 25 per cent prognosis
poor.
Clinical feature:
Early symptoms of rectal cancer
Bleeding per rectum
Tenesmus
Early morning
Investigations
:
1. Abdominal examination
2. Rectal examination
3. Proctosigmoidoscopy
4. biopsy
5. Colonoscopy
3
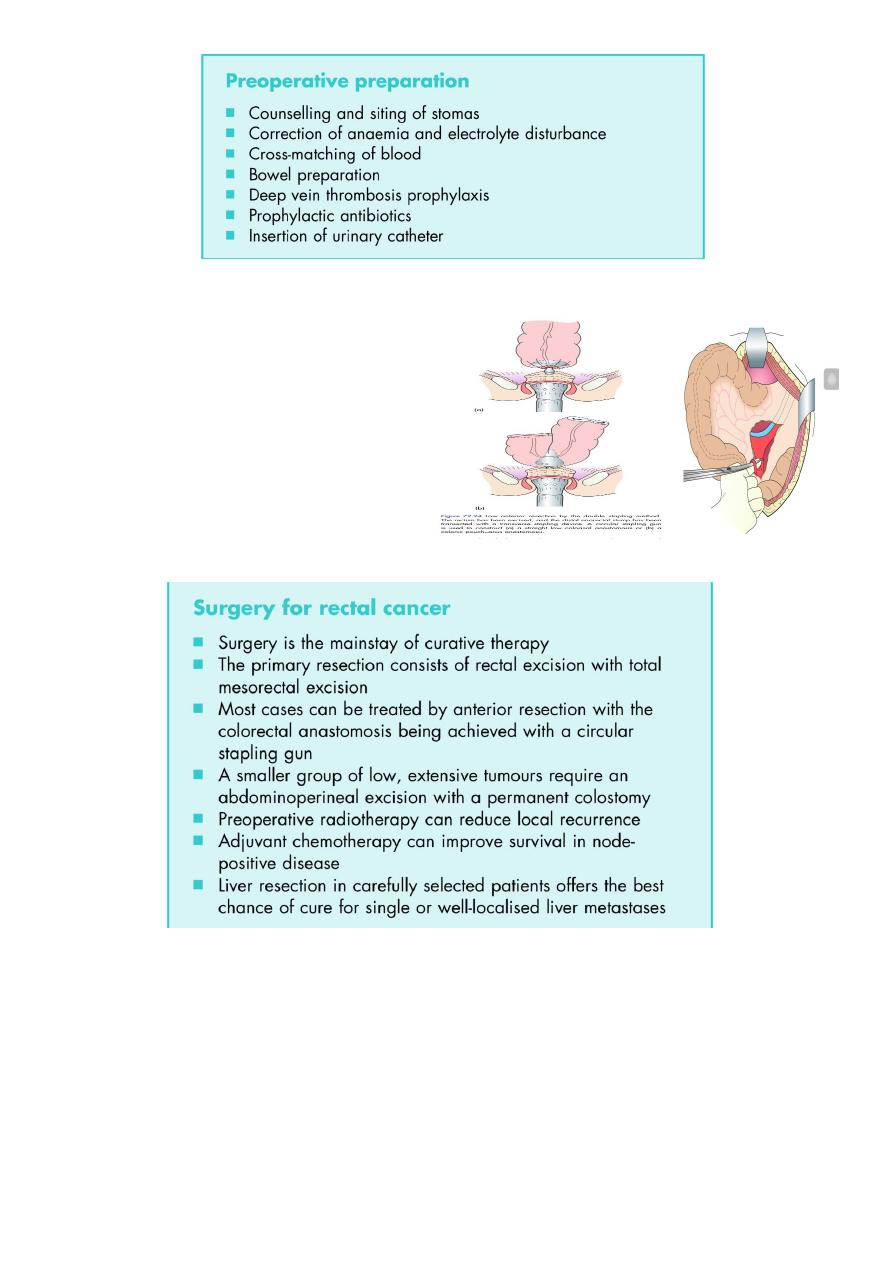
Treatment :
Surgery :
Anterior resection
Abdominoperineal resection
Endoluminal stenting
Palliative colostomy
Summary:
Radiotherapy
Chemotherapy

4
Carcinoid tumor:
Carcinoid tumour originates in the submucosa, with the mucous membrane over it
being intact. Consequently, it seldom pro- duces evidence of its presence in the early
stages, when it presents as a small plaque-like elevation. The incidence of clini- cal
malignancy, i.e. the occurrence of metastases, is 10 per cent.
Further reading 1235
This is much less than that for carcinoid tumour of the small intestine, but it is greater
than that for carcinoid tumour of the appendix. Multiple primary carcinoid tumours
of the rectum are not infrequent. The neoplasm is of slow progression, and usually
metastasises late. Large carcinoids (over 2 cm) are almost always malignant.
Treatment
Local excision is sufficient treatment for small carcinoids. Resection of the rectum is
advisable if the growth is more than 2.5 cm in diameter, if recurrence follows local
excision or if the growth is fixed to the perirectal tissues. Even when metastases are
present, resection may prolong life