1
4th
stage
Surgery
Lec-3
د.احمد ابراهيم
16/4/2016
Anal conditions
③
HAEMORRHOIDS [PILES]
In Greek Haima means blood
Rhoos means flowing
In latin pila means a ball (pile)
Hemorrhoids
Cushions of tissue and dilated varicose veins occurring in relation to the anal canal,
usually swollen and inflamed.
Precipitating factors:
o Constipation.
o Diarrhea.
o Pregnancy.
o Straining.
o Aging.
Over 2/3 of healthy people report having hemorrhoids.
Hemorrhoids tend to become worse over the years, never better, unless intervention
Pathology:-
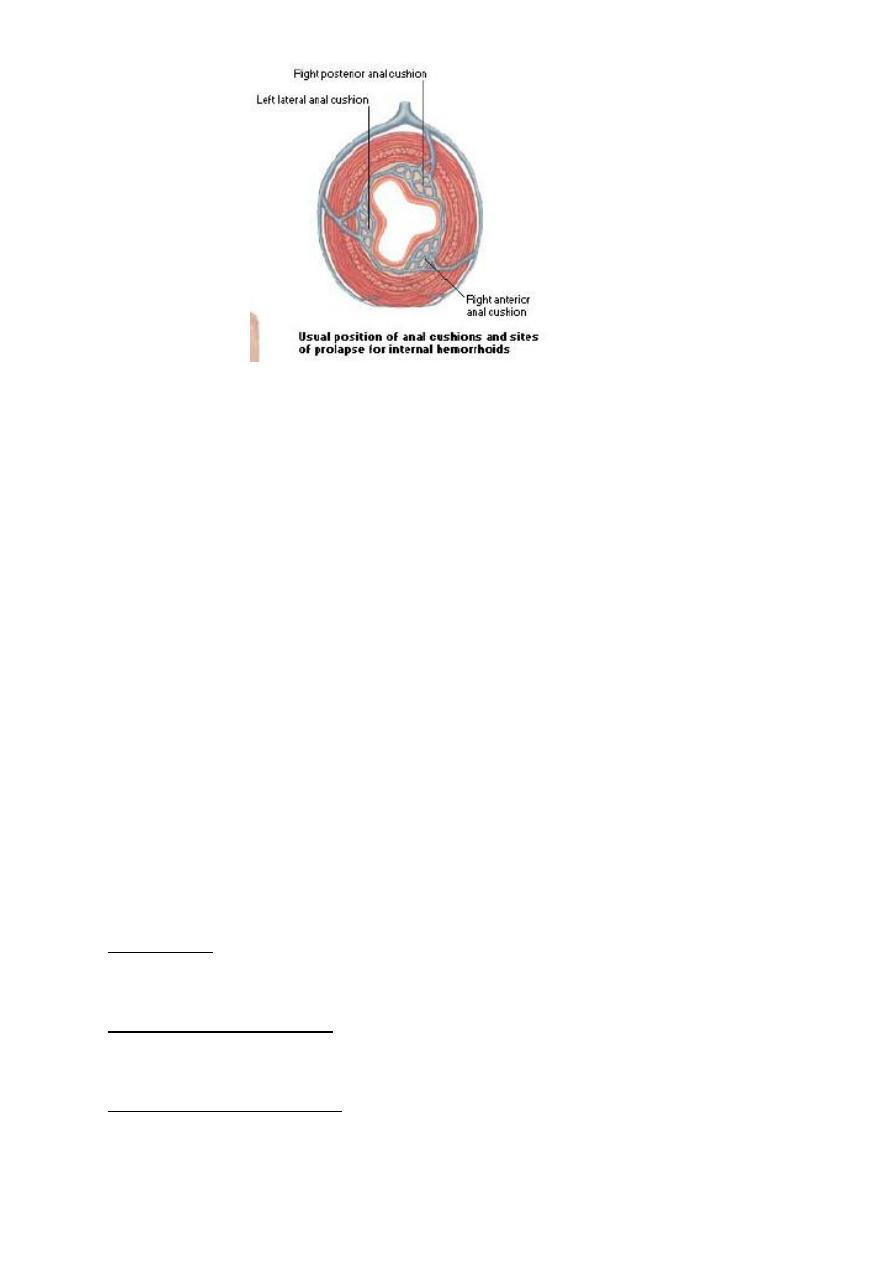
Normally the terminal branches of the superior haemorrhoidal vessels form a
vascular plexus beneath the epithelial lining of the anal canal called the anal
cushions, these cushions are usually arranged at 3, 7, 11 o'clock with the patient in
the lithotomy positions around the anal canal.
2
Any process impairs venous return will promote stasis.
Which can be produced by either:
1. systemic or by portal venous hypertension (CHF or cirrhosis).
2.Increase Intra-abdominal pressure also impairs venous return (ascites, pregnancy,
straining, and tumors).
Haemorrhoids may be external or internal, to the anal orifice.
The external is covered by skin, while the internal lies beneath the anal mucous
membrane.
When the two varieties are associated, they are known as interoexternal
haemorrhoids.
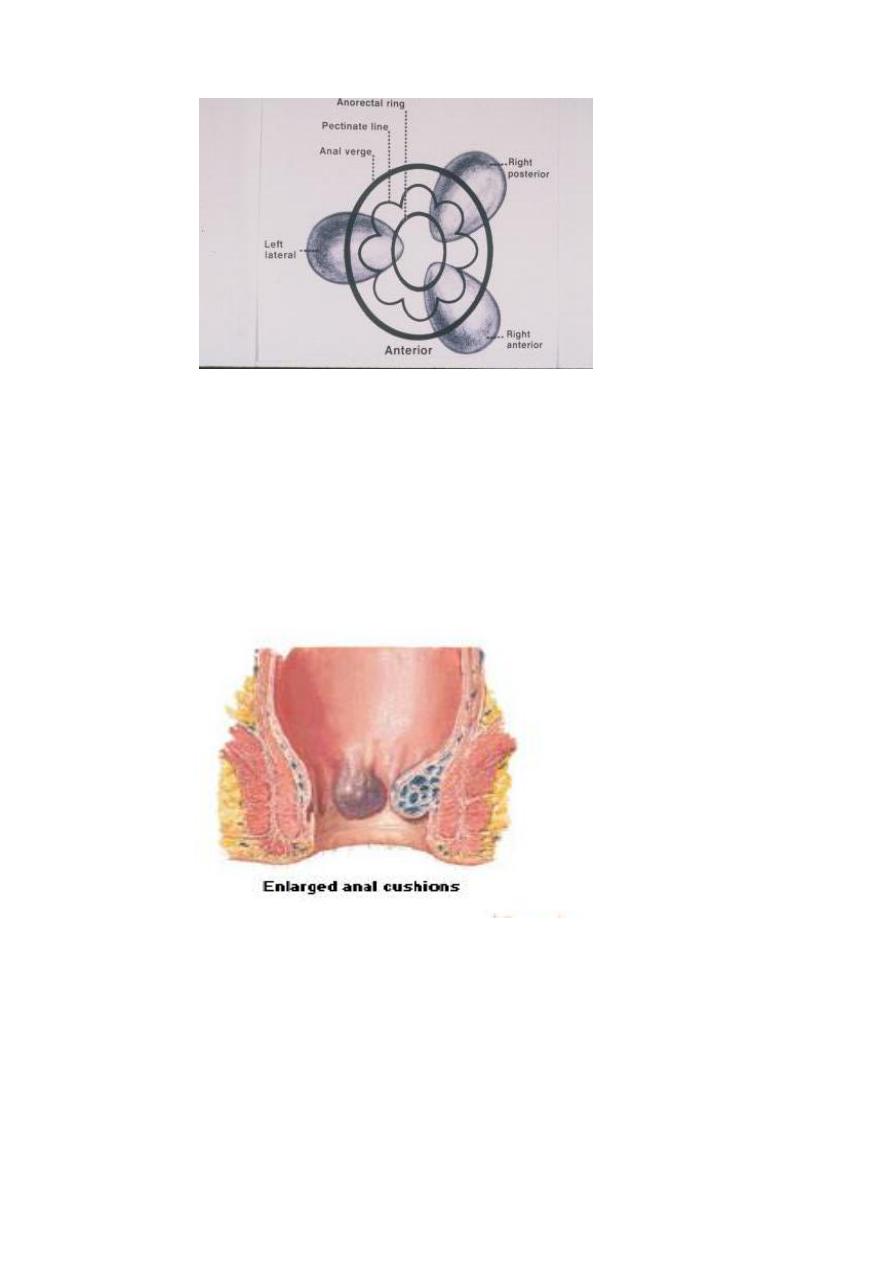
Each principal haemorrhoid divided into three parts:
The pedicle is situated at the anorectal ring.
seen by a proctoscope, covered with pale pink mucosa.
The internal haemorrhoid, which commences just below the anorectal ring.
It is bright red or purple, covered by mucous membrane.
The external haemorrhoid lies between the dentate line and the anal margin.
It is covered by skin, through which blue veins can be seen, unless fibrosis occurred.
3
In between these three primary hemorrhoids there may be smaller secondary
hemorrhoids.
Straining causes these cushions to slide downwards and internal hemorrhoids
develop in the prolapsing tissues.
Congestion, enlargement, and prolapse of the cushions constitute hemorrhoids.
Etiology:-
– Primary, no definite cause.
– Secondary, there is definite cause.
4
Primary: -
– Genetic factors. (Hereditary)
The condition frequently seen in members of the same family that there must be a
predisposing factor, such as a congenital weakness of the vein walls.
– Anatomical factors
Due to loss of elastic fibers in the anal cushions.
Secondary hemorrhoids may occur with:
– Pregnancy due to increase intra-abdominal pressure and the relaxing effect of
progesterone on the smooth muscle in the walls of the veins, plus an increased
pelvic circulating volume.
– Pelvic tumor [ Ca rectum ].
– Chronic straining at defecation ( chronic constipation) or
– Straining at micturation consequent upon a stricture of the urethra or an
enlarged prostate.
Clinical Picture:-
Bright red painless bleeding per rectum
occurs with straining, at the end of defecation, fresh bright red, jet or drops that are
separate from stools.
Prolepses
pile enlarge and descend down.
Anal discharge (pruritus)
Itching due to mucous discharge .
Pain and discomfort
usually piles painless, pain due to complication or associated fissure.
Reflex symptoms
are commonly present pain along thighs.
5
3
rd
Degree Prolapse
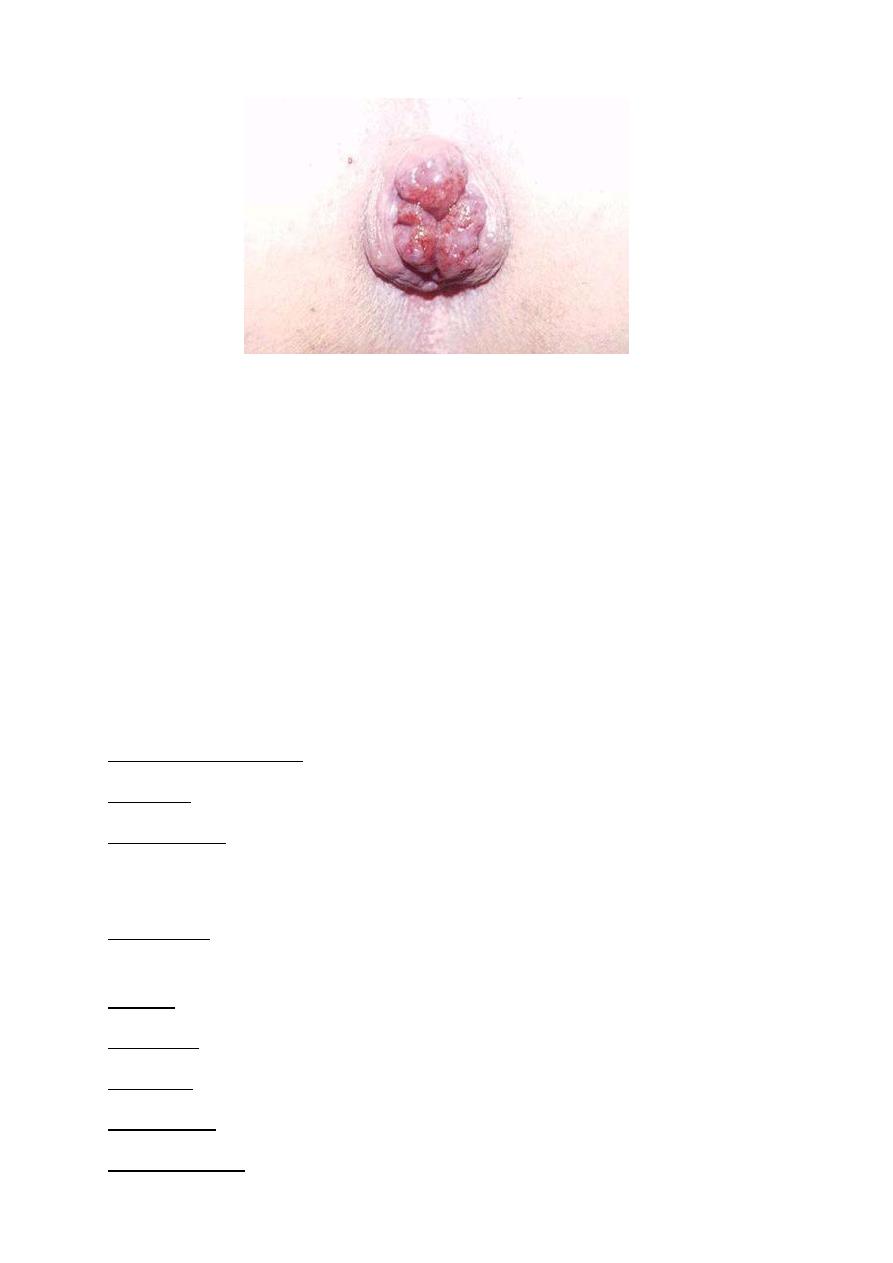
6
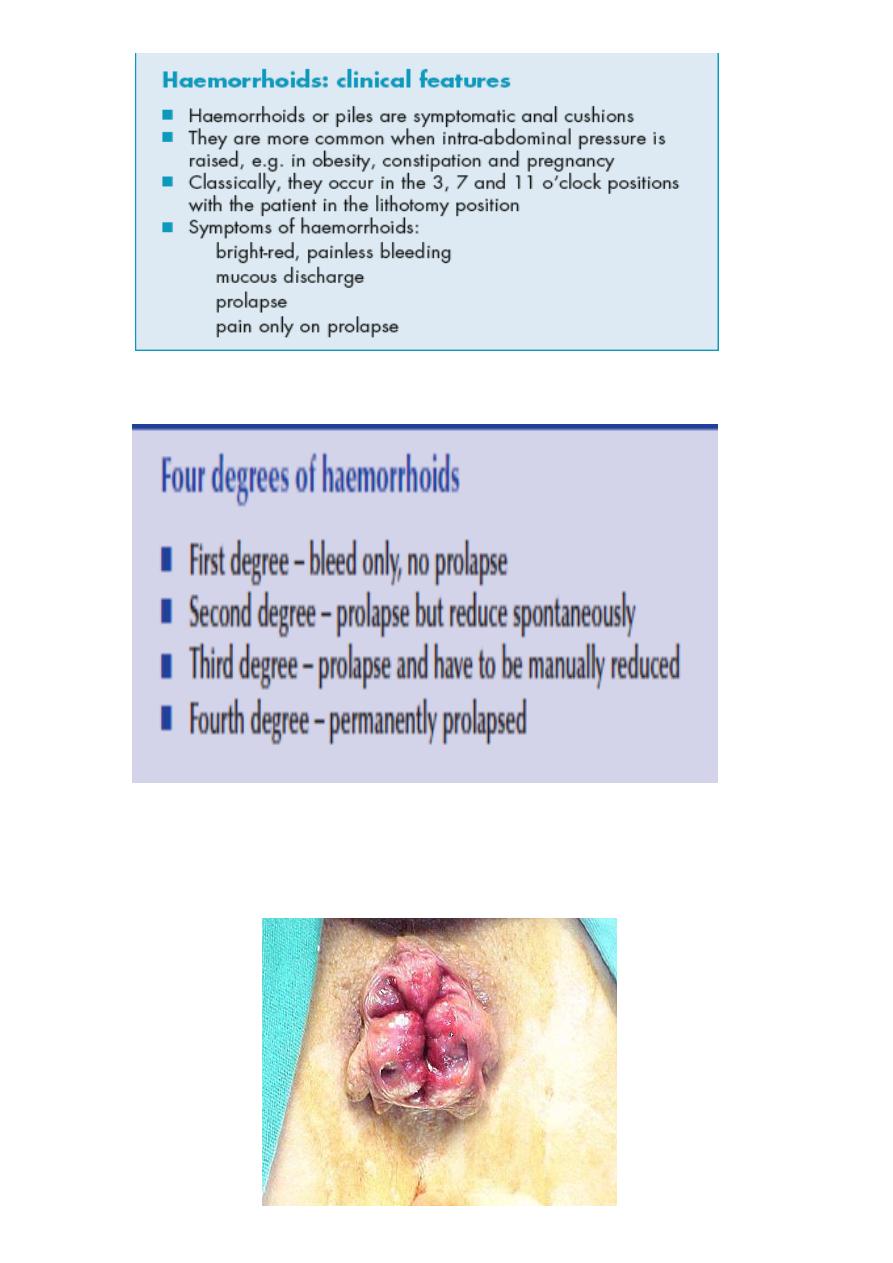
4
th
Degree Prolapse
Examination:-
Early cases no abnormality can be seen on examination of anal verge.
Proctoscopy there may be internal haemorrhoid .
In late cases prolapsing piles can be seen in 3, 7, 11 position there are mother
piles, there may be daughter piles between the main three ones.
Uncomplicated piles are impalpable on PR but important to do it to exclude
malignancy.
Sigmoidoscopy to exclude cancer.
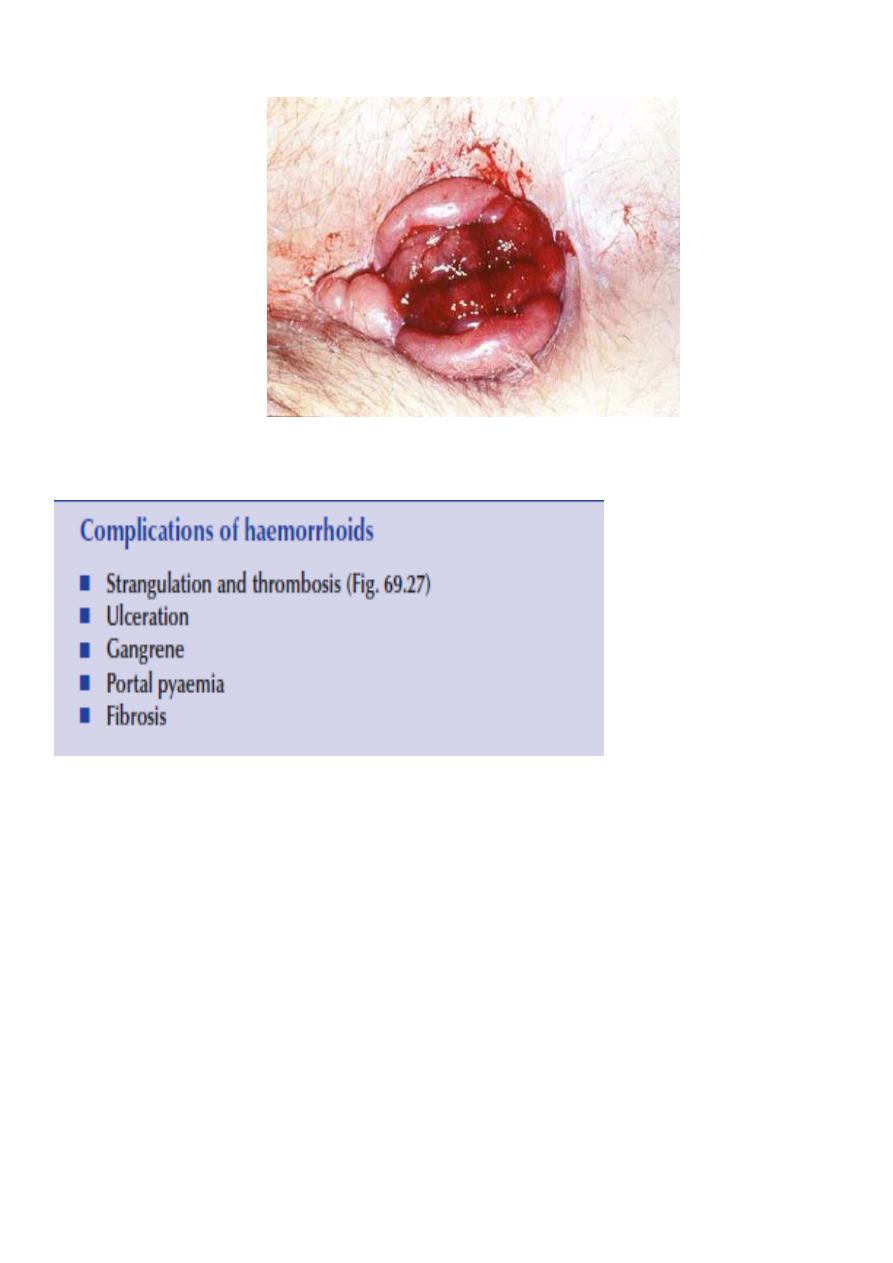
Complications:-
Profuse haemorrhage.
Anaemia.
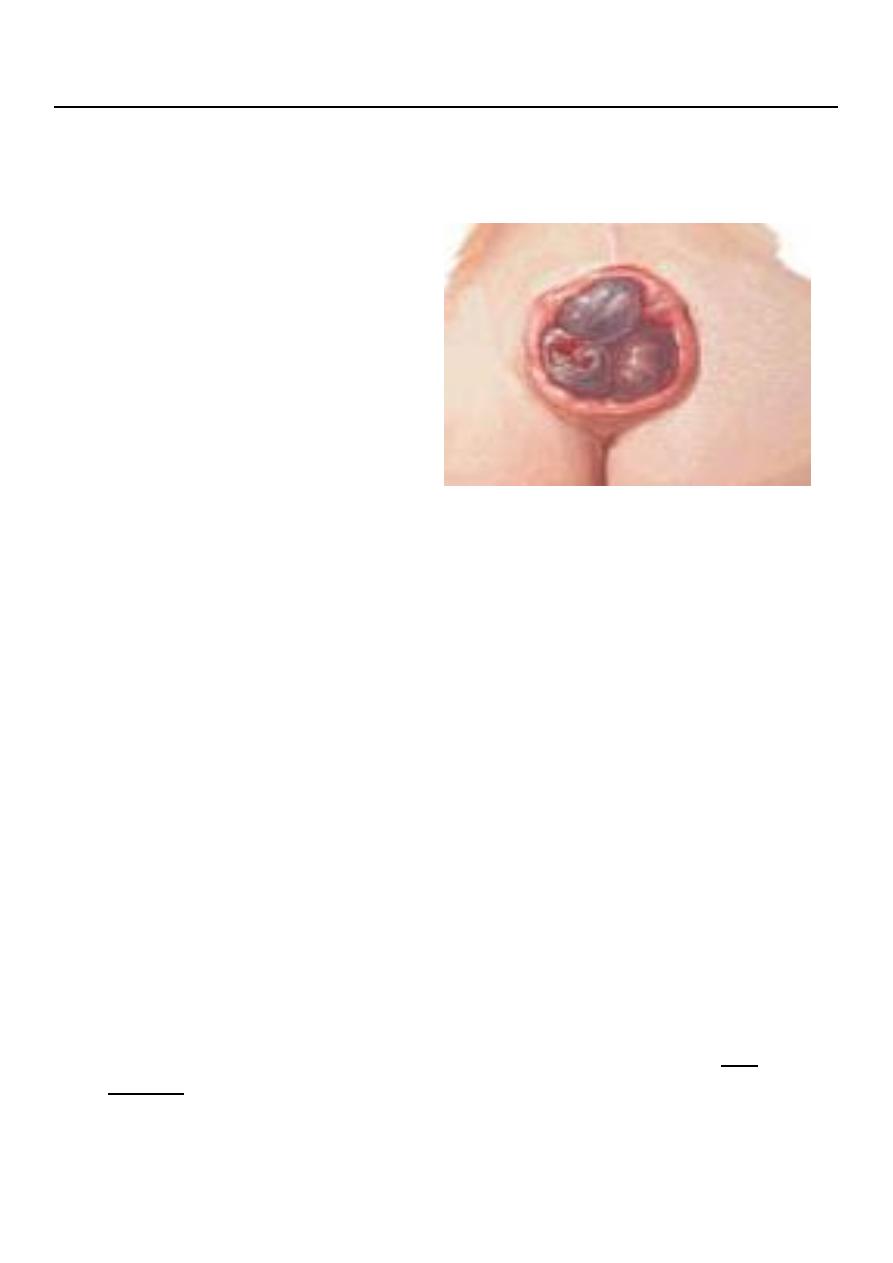
Strangulation when internal piles prolapse and become gripped by the external
sphincter this will interfere with venous return and become very tender, swollen and
very painful.
Thrombosis after strangulation, thrombosis occur and the piles look dark purple or
black.
Fibrosis may occur after thrombosis.
Ulceration may follow strangulation and thrombosis.
Gangrene if strangulation tight it lead to gangrene of piles and sloughing.
Suppuration due to infection after thrombosis.
Portal pyaemia is rare.
7
Perianal Edema
Management Of Haemmorriods
Exclusion of other causes of rectal bleeding, especially colorectal malignancy, is the
first priority.
o In the absence of a specific cause, important measures:
Normalizing bowel and defaecatory habits (only evacuating when the natural desire
to do so arises).
Adopting a defaecatory position to minimise straining.