1
Fifth stage
Medicine
Lec-2
د . منوع
1/1/2014
Common poisoning
Paracetamol poisoning
Paracetamol in overdosage can cause severe cenrilobular hepatic necrosis.
The toxic dose is 10 – 15 gm, while fatal fulminant hepatic failure is usually associated
with ingestion of 25 gm.
Paracetamol is metabolized to a toxic reactive metabolite. However, this metabolite is
detoxified by binding to glutathione. When the level of glutathione depletes, toxicity is
expected.
Symptoms of toxicity include nausea, vomiting, diarrhea, and right upper abdominal
pain.
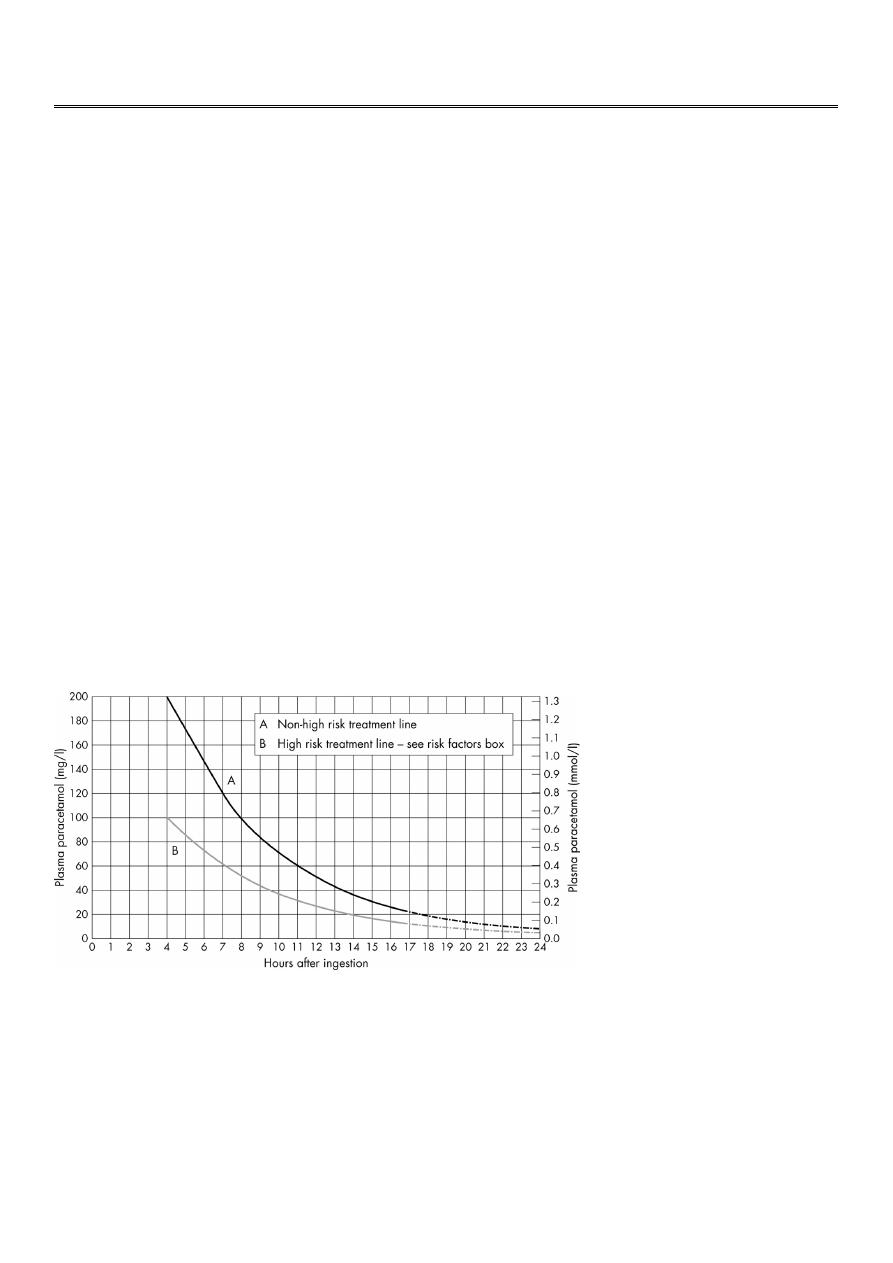
Management of paracetamol poisoning
If the patient presents within 1 hour, activated charcoal is administered.
Antidote administration is guided by the results of paracetamol serum level, plotted
against time
The antidote works by providing glutathione to detoxify paracetamol toxic metabolite.
The serum level of paracetamol should be taken 4 hours after ingestion.
If the patient presents after 8 hours, the antidote should be started before the result
of the serum level is available, because its efficacy diminishes after 10 h of ingestion.
For patients who present after 15 h, antidote therapy is started, liver function tests
and prothrombin time is asked, and liver transplantation center is consulted.

2
The antidote of choice is N. acetylcysteine which is highly protective if given in the
first 10 hours.
The dose is:
150mg/kg in 200 ml N.S. /15min.
50mg/kg in 500 ml N.S. /4h.
100mg/kg in 1 litre N.S. /20 h.
Alternatively, methionine 12 gm is given orally every 4 hours, to be repeated 4 times.
Aspirin (salicylate) poisoning
Aspirin is toxic when ingested at doses greater than 150 mg/kg.
Nausea, vomiting, tinnitus, and deafness are the initial manifestations.
Direct stimulation of the respiratory tract causes hyperventilation (central
hyperventilation).
Moderately severe poisoning is associated with peripheral vasodilatation, profuse
sweating, petechiae, and subcojunctival haemorrhage.
Serious poisoning is associated with metabolic acidosis, renal failure, CNS depression
(agitation, confusion, coma, and fits). Cerebral and pulmonary oedema may develop
Management of aspirin poisoning
Activated charcoal is used in multiple doses for adsorption of the ingested drug.
Metabolic acidosis is treated with 8.4% NaHCO
3
.
IV normal saline is required to control severe dehydration (from sweating and vomiting).
Fluids should be given with caution to avoid precipitating pulmonary oedema.
In severe poisoning, urinary alkalinization is needed; one litre of 1.26% NaHCO
3
is
infused over 3 hours, keeping urine pH around 7.6 – 8.5. Alkaline urine facilitates aspirin
excretion.
Haemodialysis is very effective in removing salicylate, and correcting acid base
imbalance
Organophosphorus poisoning
OPs are widely used as pesticides in agriculture, and as chemical warfare agents.
There are 3 million cases worldwide each year around 300000 deaths.
OP inactivate acetylcholine estase (AchE) enzyme by phosphorylation leading to
accumulation of acetyl choline (Ach) at cholinergic synapses (muscarinic, nicotinic, and
central).
3
Muscarinic effects:
miosis bradycardia (tachycardia in 20% of cases)
bronchorhoea salivation
lacrimation abdominal pain
bronchoconstriction
Nicotinic effects:
muscle fasciculation
hyperreflexia
flaccid paralysis and hyporeflexia
CNS effects:
headache dizziness
confusion coma
fits respiratory depression
Management of OP poisoning
Atropine (1.8 – 3 mg) is injected as a bolus immediately (3 -6 ampoules), repeated every
5 minutes until atropinization (clear lung, dry tongue, normal pulse rate, and dilated
pupils).
Once atropinization is complete, 20 – 30% of the bolus dose required is infused/ hour.
Treatment should be continued for several days to avoid relapse.
Atropine is a muscarinic receptor antagonist, effective in relieving the muscarinic effects
of the toxins only.
Oxime derivatives (pralidoxime and obidoxime) reactivate phosphorylated AchE, and can
reverse the nicotinic effects of OP toxins.
CNS effects are treated by diazepam for convulsions, oxygen and ventilatory support for
respiratory failure
Delayed complications of OP poisoning
After the acute cholinergic crisis is over, some patients develop an intermediate
syndrome (around 48 hours later). Muscle weakness and respiratory paralysis develop
due to downregulation of the nicotinic receptors due to accumulated Ach.

4
Rarely, OP induced delayed polyneuropathy may occur 1 – 3 weeks after the initial
exposure due to degeneration of long myelinated nerve fibers. The disability it causes
may recover partially after 1- 2 years.
Digoxine poisoning
Clinical features:
nausea, vomiting, diarrhoea
visual symptoms
confusion
hyperkalaemia
variable brady-, tachyarrhythmia.
Treatment:
Specific antidote (digoxine antibody Fab fragments)
Continuous ECG monitoring
Volume replacement in case of hypotension (
enotropics)
Correction of hypokalaemia and hypomagnesaemia
Atropine for bradyarrythmias
Tachyarrythmias, accordingly
Tricyclic antidepressants poisoning
Clinical features:
hypotension and variable arrhythmias (negative enotropic effect and arrythmogenic)
warm dry skin
convulsions
Treatment:
volume replacement
vasopressor agent
cotiuous ECG monitoring
sodium bicarbonate (NaHCO3) 8.4%; in case of prolonged QRS complex or
tachyarrhythmias
5
Selective serotonin reuptake inhibitors (SSRIs)
These drugs are less cardiotoxic than TCAD.
However, in large doses SSRIs can still cause hypotension and arrhythmias, as well as
fever.
The treatment of toxicity is similar to TCAD.